Article Text

Abstract
Atrial fibrillation (AF) is directly implicated in embolic stroke and suspected in a large proportion of cryptogenic stroke. The current stroke-prevention strategy in embolic and cryptogenic stroke starts with arrhythmia detection, followed by risk stratification and treatment for those deemed to be at increased risk. This approach is practical and widespread; however, more recent findings have questioned its validity. Arrhythmia detection is dependent on the length and fidelity of monitoring. Long-term monitoring using implanted recorders improves arrhythmia detection in patients with cryptogenic stroke. A large proportion of patients with cryptogenic stroke, however, were shown not to have any AF. Moreover, in patients with permanent pacemakers who also experienced thromboembolic events, AF did not always precede thromboembolisation. These results raise cause and effect questions about the role of AF, the arrhythmia, in thrombus formation and embolisation. Moreover, risk estimation scores; such as Congestive heart failure, Hypertension, Age, Diabetes and previous Stroke or Transient Ischaemic Attack, Vascular disease and female sex category (CHA2DS2-VASc), have a suboptimal predictive accuracy and the mechanism relating their individual components to thrombogenesis is unknown. Given these limitations, a more comprehensive and mechanistic evaluation of atrial disease is needed to better identify patients at risk for stroke and AF. Atrial fibrosis, quantified using late gadolinium enhancement cardiac MRI, is associated with reduced atrial function, stroke and the presence of left atrial thrombus in patients with AF. Biomarkers such as B-type natriuretic peptide, cardiac troponin have also been linked to increased thromboembolic risk and AF.
- Stroke
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia in adult cardiology with an estimated prevalence of over 3.0 million Americans and 6.0 million Europeans and a projected increase in prevalence in the coming few decades.1 ,2 Cardioembolic stroke attributable to AF accounts for up to 30% of all ischaemic strokes.3 Subclinical AF is often suspected in cryptogenic stroke, or embolic stroke of unknown source, which accounts for another 30% of ischaemic strokes.
Documentation of AF has been the corner stone of primary and secondary prevention of embolic and cryptogenic stroke. Ambulatory cardiac monitoring, of widely variable duration, is often undertaken following stroke or transient ischaemic attack for this purpose. Once AF is diagnosed, risk stratification scores, mostly based on clinical parameters, are used to estimate an annualised risk of thromboembolic events. Preventive therapy, commonly with oral anticoagulation, is subsequently instituted for those deemed at high risk. While this approach is practical and widely used, recent studies have exposed some significant limitations and highlighted a need for a more mechanistic approach linking the arrhythmia and clinical risk factors to actual thromboembolic events.
In the subsequent paragraphs, we review recent findings that challenge this practice paradigm and introduce new and more mechanistic perspectives linking both thromboembolisation as well as the clinical arrhythmia of AF to a diseased fibrotic atrium, suggesting that a single disease process may be responsible for both of these important clinical problems.
Current practice paradigm for cardioembolic stroke
AF is an established diagnosis at the time of, or diagnosed following stroke in 25–30% of cases.4 When AF is not present on presentation, yet clinically suspected, ambulatory monitoring is instituted for diagnosis. Once this is established, risk stratification scores, such as the CHA2DS2-VASc score, a composite score that includes Congestive heart failure, Hypertension, Age, Diabetes and previous Stroke or Transient Ischaemic Attack, Vascular disease and female sex category, are used to estimate an annualised thromboembolism risk. Bleeding risk is also estimated using scores such as the HAS-BLED score, a composite score that includes Hypertension, Abnormal renal or liver function, Stroke, Bleeding, Labile international normalized ratio (INR), Elderly (age) and Drug or alcohol use. Based on a risk-to-benefit assessment, often involving a shared decision making process with the patient, oral anticoagulation is instituted when the thromboembolic risk exceeds that of bleeding. More recently left atrial appendage occlusion has been shown to be a viable alternative to anticoagulation.5 This practice paradigm is summarised in figure 1.

The current paradigm for prevention of AF-related thromboembolic events. AF, atrial fibrillation.
Association of AF and thromboembolic events
The rate at which AF is diagnosed using external monitors in patients with cryptogenic stroke varies between 4% and 23% depending on the duration of monitoring.6 Conventional ambulatory monitoring is often fraught with errors because of its limited duration and undersampling of AF, an arrhythmia that is commonly paroxysmal. Other limitations include poor data quality due to lead loss, patient compliance with wearing the monitor, which is often a difficult task to perform shortly after sustaining an ischaemic stroke. The use of implantable loop recorders is one alternative approach used to overcome these limitations. These devices assure continuous and long-term (up to 3 years) monitoring without the use of external electrodes. The CRYSTAL-AF study used implantable monitors for AF diagnosis following cryptogenic stroke. It demonstrated superiority in documenting AF compared with the external conventional monitors. At 3 years, AF was diagnosed in 30% of patients with cryptogenic stroke using the loop recorder,7 a threefold increase compared with conventional monitors. While this is a significant improvement in the ascertainment of the arrhythmia, the fact that AF was absent in 70% of patients with cryptogenic stroke is a rather surprising finding. Acknowledging that not all cryptogenic stroke is due to cardiac thromboembolism,8 CRYSTAL-AF findings raise questions about the role of AF in this type of stroke.
Data from implanted pacemakers raise similar questions. When a pacemaker lead is present in the atrium in patients with cardiac implanted electronic devices (implantable atrial or atrioventricular cardiac pacemakers and/or defibrillators), intracardiac atrial electrical signals are recorded with the highest sensitivity and specificity to diagnose the presence of AF. Studies evaluating patients with such devices, which have also had thromboembolic events, show that AF or other rapid atrial rhythm episodes often do not precede these embolic events. Some AF episodes predated the embolic events by several months, while others did not occur until after their embolic events.9 While there may occasionally be some electromechanical delay between atrial rhythm change and contractile dysfunction, this does not fully explain these findings. It is also very unlikely that the association of AF and stroke is due to chance.
Taken together, the findings from implantable loop recorders and pacemakers suggest that the presence of AF may not be a necessary component in the pathophysiology of thrombogenesis and embolisation.
Current risk stratification for stroke inaccurately estimates thromboembolic risk
While cryptogenic stroke is generally thought to be embolic, sources of embolisation include the heart, the aortic arch and venous emboli paradoxically traversing through an intracardiac defect. With a significant proportion of cryptogenic strokes suspected to be cardio-embolic, the same risk scores used for AF-related stroke are invoked. The CHA2DS2-VASc scores, is the most commonly used thromboembolism risk stratification tools in AF.2 ,10 It relies on patient clinical parameters and comorbidities to estimate the risk for future strokes. While scores are simple and easy to use, they are also known to have poor predictive accuracy. A comparative analysis showed all scores, including older and currently used ones, to have an area under the curve of less than 70%, leaving significant room for improvement.11 ,12 More importantly, the pathophysiological mechanism behind the statistical association of the clinical factors included in risk stratification, and thrombogenesis is not known.
What is known about the mechanism of thrombosis in AF?
The mechanistic process of thrombus formation in AF is not fully understood. It has been suggested that thrombogenesis in AF is similar to other vascular beds where a Virchow's triad of stasis, hypercoagulability and tissue injury is present for thrombus to form.13 Of this triad, the most commonly ascertained finding is that AF is associated with a decrease in mechanical atrial contraction, most commonly in the left atrial appendage.14 Induced, short episodes of AF during electrophysiology testing were also found to be associated with an increase in biomarkers of endothelial dysfunction and activation of platelets and clotting factors.15 With AF absent in a large proportion of cases of cryptogenic stroke and often not preceding thromboembolic events in patients with pacemaker, a deeper look at the underlying diseased atrium may offer a mechanistic insight of thrombogenesis in AF.
AF-associated tissue changes
AF is associated with tissue as well as overall atrial chamber structural remodelling.16 This remodelling process is integral to the pathophysiology of AF and constitutes the substrate required for its maintenance.
The mechanism of atrial fibrosis in AF is likely to be multifactorial.10 Studies have linked atrial disease to cardiac factors (genetic, valvular, ischaemic, infiltrative, inflammatory) as well as extra-cardiac (hypertension, obesity, sleep apnoea, autonomic) factors.17–19 New evidence suggests a role for epicardial adipose tissue in atrial fibrosis through a local paracrine effect.20 Voltage mapping, which samples electrical signals from atrial tissue, has been proposed as an invasive method to assess and stage the extent of atrial disease based upon the premise that diseased tissue would yield a low voltage signal.21
Late gadolinium enhancement MRI (LGE-MRI) is an established, non-invasive imaging method for fibrotic scarring in the ventricle following myocardial infarction.22 It uses washout kinetics of gadolinium to generate different levels of enhancement in healthy compared with fibrotic tissue. When applied to the atrium, this technique provides a non-invasive method to assess fibrosis of atrial tissue.23 Several studies have demonstrated this to be both feasible and reproducible in assessing atrial fibrosis.24 Currently, LGE-MRI has been increasingly used in clinical decision making for rhythm management of patients with AF, as extensive atrial tissue fibrosis quantified using LGE-MRI is associated with poor response to arrhythmia treatment with catheter ablation.25 LGE-MRI identified regions of enhancement were demonstrated to represent atrial fibrosis by obtaining biopsies from patients undergoing cardiac surgery.26 The extent of fibrosis was also higher in persistent AF and longer time from AF diagnosis, compared with paroxysmal phenotypes. Atrial fibrosis detected with LGE-MRI was also found, although to a lesser extent, in a control group of patient without AF,26 suggesting that fibrosis precedes the onset of the arrhythmia and that it is a progressive disease.
Atrial fibrosis identified using LGE-MRI has been linked to stroke, atrial mechanical dysfunction and presence of thrombus in the left atrial appendage.
Atrial fibrosis and atrial mechanical function
Atrial fibrosis, assessed LGE-MRI, has been associated with atrial mechanical dysfunction assessed echocardiographically with speckle tracking to evaluate atrial wall deformation or strain. Wall strain is sampled from different areas of interest, typically laterally on the atrial free wall, and curves are generated when strain is plotted against time for the duration of the cardiac cycle. Normally, contracting atria have a high deformation index or strain while atria with reduced contractility have a reduced deformation. High levels of atrial fibrosis measured by LGE-MRI, in patients with a history of AF, were associated with reduced atrial strain, indicating that atrial fibrosis is associated with reduced mechanical atrial function.27 ,28 The relationship between atrial strain and fibrosis is illustrated in figure 2.
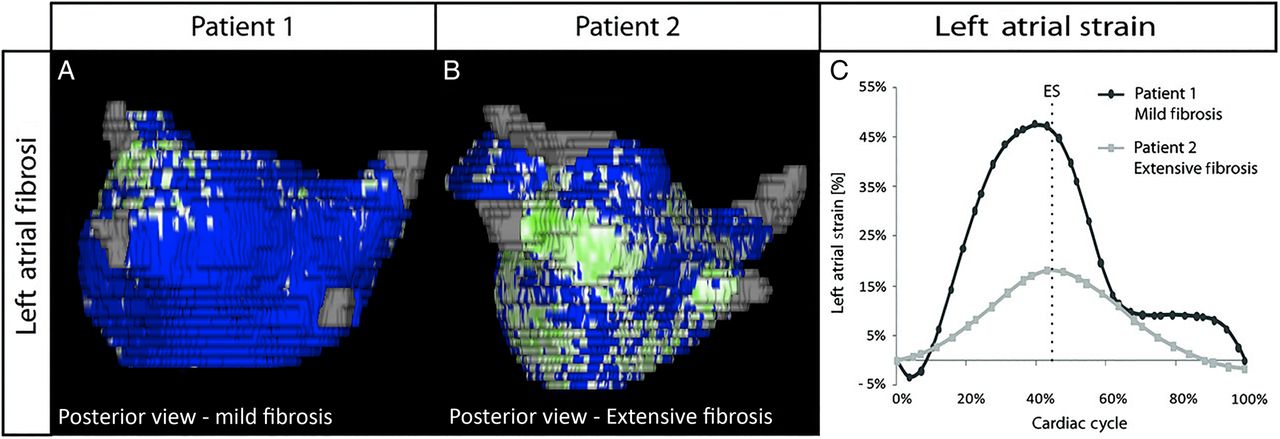
Left atrial strain is reduced in patients with atrial fibrillation and advanced fibrosis. Late gadolinium enhancement MRI of the left atrium demonstrates higher fibrosis in patient 2 compared with patient 1. Left atrial strain is lower in patient 2 compared with patient 1. Reproduced with permission from Kuppahally et al.27
Relationship of atrial fibrosis with spontaneous echocardiographic contrast and appendage thrombus
Transoesophageal echocardiography (TEE) is often used in patients with persistent AF prior to undergoing cardioversion or catheter ablation, especially when the duration of arrhythmia and that of therapeutic anticoagulation cannot be ascertained. When these patients also underwent LGE-MRI to quantify atrial fibrosis, findings of spontaneous atrial echocardiographic contrast and left atrial appendage thrombus were associated with significantly higher atrial fibrosis compared with patients with normal transoesophageal examinations.29 Figure 3 shows a comparison of atrial fibrosis levels between the three transoesophageal echocardiography groups. Moreover, left atrial appendage involvement with fibrosis was associated with reduced blood flow velocities exiting from the appendage. It has been previously demonstrated that decreased left atrial appendage velocity is associated with a higher risk of stroke and embolic events.30 The presence of extensive atrial fibrosis, defined with a cut-off value of 20% of the atrial wall, improved a prediction model for the presence of appendage thrombus on transoesophageal echocardiography by 16%. Atrial fibrosis >20%, added to a prediction model for appendage thrombus, improved the area under the curve compared to the CHA2DS2-VASc alone (0.80 vs 0.67).29

Association between atrial fibrosis and left atrial appendage thrombus. Patients with atrial fibrillation and appendage thrombus have higher atrial fibrosis compared with patients without appendage thrombus or spontaneous echocardiographic contrast.
Relationship of atrial fibrosis and stroke
The relationship between stroke and LGE-MRI quantified fibrosis was evaluated retrospectively in a cohort of patients with AF.31 Patients with AF and a prior history of stroke had a higher degree of fibrosis compared with those who had AF without a history of stroke (figure 4). Moreover, patients at the highest quartile of fibrosis (>20%) had the highest likelihood of previous stroke.

Association between atrial fibrosis and stroke. Patients with atrial fibrillation (AF) and a history of stroke have higher atrial fibrosis compared with those who have AF without a history of stroke. Adapted with permission from Daccarett et al.31
ECG and echocardiographic parameters
ECG assessments of atrial disease, such as P wave duration and P wave terminal force, have been evaluated in cohort studies showing an association with stroke outcomes.32 An enlarged left atrium could lead to an increase in P wave duration as well as a deeper and wider terminal portion of the P wave in lead V1 on 12 lead ECG. This approach has a low sensitivity and specificity due to the fact that ECG signals, especially atrial signals, are affected by body habitus, lead position, lung pathology (eg, emphysema) and obesity. Moreover, the analysis of P wave forces currently still lacks standardisation and validation across different cohorts.33
Echocardiographic assessment of atrial size is also commonly performed, typically using a transthoracic study. Large atrial size has been linked to embolic and cryptogenic initial and recurrent stroke.34 Increase in atrial volume, indexed to body size, has been correlated with increase in atrial fibrosis; however, this association is not a linear one with some patients demonstrating high fibrosis while still showing modest increases in atrial volume.26
Serum markers of increased stroke risk
Measurements of B-type natriuretic peptide (BNP) and the N-terminal fragment of BNP indicate that elevated values are associated with risk for development of AF as well as stroke, even in the setting of normal ventricular function.35 ,36 BNP is also more elevated in patients with suspected cardioembolic stroke when compared with patients who have non-cardioembolic stroke. The mechanism behind this association, especially in the absence of left ventricular dysfunction, is not readily discernable. Natriuretic peptide biology is complex with several volume and pressure loading conditions affecting their synthesis and secretion.37 It is plausible that myocardial stretching due to pressure or volume overload, leads to atrial fibrosis which in turn leads to reduced atrial mechanical function and subsequent stasis and thrombosis. BNP is also secreted from brain tissue and it may be elevated in the setting of stroke, rendering the prognostic or predictive impact of these measured values of limited utility in the setting of acute stroke.
Similarly, elevated levels of cardiac troponin,38 C-reactive protein39 and interleukin-640 have been linked to higher risk of cardioembolic stroke in large trials of patients with AF. Cardiac troponin is a marker of myocardial cell death, which may herald a reparative fibrotic process. Tracing troponin elevation back to an atrial fibrotic process is very difficult as the ventricular myocardial mass is significantly larger, and more likely to be the source of this troponin elevation. C-reactive protein and interleukin-6 are not cardiac specific.
Chronic kidney disease and proteinuria are also associated with increased stroke risk in AF.41
Summary and future directions
The current approach to management of patients with embolic and cryptogenic stroke is focused on the detection of AF. New evidence suggests that both stroke and AF are associated with atrial structural changes including atrial fibrosis and associated dysfunction. Serum biomarkers of myocardial cell death, stretch and inflammation are also associated with stroke. These findings lead us to propose a new perspective on thromboembolic stroke that is focused on atrial disease, rather than rhythm abnormality. Clinical risk factors, in addition to genetic and other contributing factors lead to atrial fibrosis and an atrial myopathy. This myopathy can manifest electrically through AF, the arrhythmia, initiated by electrical triggers, as well as thromboembolic stroke through mechanical dysfunction and other factors that create a hypercoagulable milieu.
This new proposed paradigm, illustrated in figure 5, would offer a more mechanistic explanation of the association of clinical risk factors such as age, hypertension, diabetes, chronic kidney disease and others, with stroke as well as AF. The proposed associations need to be rigorously tested in large and diverse patient cohorts to establish a link between atrial fibrosis and thromboembolism, independent of the presence of AF. Once verified, this approach promises to refine our current risk assessment for thromboembolism and may lead to a more precise identification of high-risk patients who will likely benefit from treatment. Atrial fibrosis may also be a future therapeutic target to lower stroke as well as AF risk.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagram depicting proposed association between risk factors leading to atrial fibrosis and clinical outcomes of atrial fibrillation and thromboembolism. Risk factors contribute to formation and progression of atrial fibrosis. Once fibrosis is present, arrhythmic triggers together with the fibrotic substrate initiate and maintain the arrhythmia; thrombogenic triggers together with mechanical dysfunction associated with fibrosis lead to thromboembolisation.
References
Footnotes
Contributors NA contributed to the planning, conduct and reporting of the work described in the article.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.