Article Text

Abstract
Objective Abnormal body mass index (BMI) is associated with higher mortality in various cardiovascular cohorts. The prognostic implications of BMI in adults with congenital heart disease (ACHD) are unknown. We aim to assess the distribution of BMI and its association with symptoms and survival in the ACHD population.
Methods We included 3069 ACHD patients (median age 32.6 years) under follow-up at our institution between 2001 and 2015. Patients were classified based on BMI as underweight (<18.5), normal weight (18.5–25), overweight (25–30) or obese (>30), and symptoms, exercise capacity and mortality were assessed.
Results Overall, 6.2% of patients were underweight, 51.1% had normal weight, 28.2% were overweight and 14.6% were obese. Higher BMI values were associated with lower all-cause and cardiac mortality on univariable Cox analysis, and this effect persisted after adjustment for age, defect complexity, cyanosis and objective exercise capacity. Higher BMI was especially associated with better prognosis in symptomatic ACHD patients (HR 0.94 (95% CI 0.90 to 0.98), p=0.002) and those with complex underlying cardiac defects (HR 0.96 (95% CI 0.91 to 0.997), p=0.048) In patients with a complex cardiac defect who had repeated weight measurements, weight loss was also associated with a worse survival (HR 1.82 (95% CI 1.02 to 3.24), p=0.04).
Conclusions ACHD patients with a higher BMI had a lower mortality. The association between BMI and mortality was especially pronounced in symptomatic patients with complex underlying cardiac defects, suggesting that cardiac cachexia may play a role. Indeed, weight loss in complex ACHD patients was linked to an even higher mortality.
- Adult Congenital Heart Disease
- Body Mass Index
- prognosis.
Statistics from Altmetric.com
Key messages
What is already known on this subject?
Obesity is emerging as a global epidemic and its prevalence has increased over the past few decades worldwide. While it has been established that obesity increases the risk of premature mortality and various morbidities, its impact on chronic conditions is less clear and in fact unknown in adults with congenital heart disease (ACHD).
What might this study add?
The results of this study suggest that especially symptomatic ACHD patients and those with complex underlying cardiac defect could have a superior short and midterm prognosis with BMI values that would formally by considered unhealthy (ie, consistent with overweight/mild obesity).
How might this impact on clinical practice?
ACHD patients with complex underlying cardiac defect should be made aware that evidence on the adverse prognostic impact of overweight or mild obesity is currently lacking for their condition and that unintentional weight loss is likely to be associated with worse prognosis.
Introduction
Obesity is emerging as a global epidemic and its prevalence has increased at an alarming rate in the last few decades worldwide.1 While numerous studies have established that obesity increases the risk of premature mortality and predisposes to diseases such as diabetes, hypertension or cardiovascular disease in the general population,2–5 its impact in chronic life-long conditions is less clear. In contrast to the widely held public belief that obesity invariably shortens life expectancy, there is recent evidence that the optimal body size might be different between normal individuals and those with long-standing chronic disease, in whom a higher body mass index (BMI) may be associated with a better outcome. This so-called ‘obesity paradox’6 has linked higher BMI to better survival in a variety of chronic diseases, such as chronic heart failure (HF),7 8 kidney disease and chronic obstructive pulmonary disease.9
Limited and conflicting data on the prevalence of obesity in adults with congenital heart disease (ACHD) exist and the association between BMI and outcome has not yet been established.10–12 The aim of our study was to establish the distribution of BMI and its association with outcome in a large contemporary cohort of ACHD patients.
Methods
Study patients
We retrospectively reviewed data on all patients with congenital heart disease under active follow-up at the Royal Brompton Hospital, London, between 2001 and 2015, based on available administrative and clinical databases. All patients older than 14 years of age in whom data on height and weight were electronically available were included. Whenever possible, data collected at the time of cardiopulmonary testing was favoured over other data sources to allow accounting for physical fitness. In patients with more than one exercise test during the study time frame, information from the most recent test was used for analysis.
Clinical data
Data containing information on diagnosis, age, gender, height, weight, New York Heart Association (NHYA) functional class, blood pressure and cyanosis were collected. Patients with cyanosis were defined as those with oxygen saturation of <90% at rest or patients who were known to desaturate with exercise. In patients undergoing cardiopulmonary exercise testing (87.6% of the population), data on peak oxygen uptake (pVO2), VE/VCO2 slope and blood pressure response to exercise were included. Patients underwent exercise testing on a treadmill using a modified Bruce protocol as previously published.13 14 The severity of the cardiac defect was categorised based on the Bethesda system as ‘simple’, ‘moderate’ or ‘complex’.15 Patients with multiple defects but without Eisenmenger syndrome were classified as complex. BMI was calculated as body weight (in kg) divided by squared height (in metres). As recommended by WHO, patients were classified based on BMI as underweight (<18.5 kg/m²), normal weight (18.5–24.9 kg/m²), overweight (≥25–29.9 kg/m²) and obese (≥30 kg/m²).16
Longitudinal analysis
If more than one weight recording over time was available in a patient, the two most recent values were used to calculate temporal weight/BMI changes. Also, the difference between the last weight measurement and the median of all weights recorded during the study period in a given patient was calculated to account for the fluctuation in weight over time. Data on overall mortality were retrieved from the Office for National Statistics, which registers all UK deaths. The cause of death was established from medical records and death certificates by one investigator (G-PD). As this was a retrospective analysis based on data collected for routine clinical care and administrative purposes (UK National Research Ethics Service guidance), individual informed consent was not required. The study was approved by the Research and Governance Committee at our institution.
Statistical analysis
Data are presented as numbers/percentages for categorical variables, while mean±SD values or median and IQR are given for continuous variables depending on data distribution. The association between BMI and mortality was assessed using univariable and multivariable Cox proportional hazards regression analysis. The proportional hazards assumption was verified using generalised linear regression analysis, testing for a non-zero slope of the scaled Schoenfeld residuals in addition to visual inspection of the graphs of the regression. Relevant clinical parameters were tested for significance on univariable analysis. All parameters that were significantly related to prognosis on univariable analysis (p<0.05) were subsequently included in multivariable time-dependent models. Parameters of cardiopulmonary exercise testing as well as weight and BMI are highly correlated with each other. Therefore, only pVO2 and BMI were included in the multivariable analysis to avoid issues with multicollinearity. For all analyses, a two-tailed p-value <0.05 was used for statistical significance. Analyses were performed with the use of R V.3.1.0 (R Foundation for Statistical Computing).
Results
Overall, 3086 patients were included in the current analysis. 48% of patients were female and the median age of the study group was 32.6 years (table 1). The majority of patients had normal weight (51.1%), while 6.2% of patients were underweight, 28.2% were overweight and 14.6% classified as obese based on BMI. Obese patients were significantly older (41.1 (IQR: 27.8–50.5) vs 31.9 (23.4–43.5) years; p<0.0001) and had higher systolic and diastolic blood pressure values compared with non-obese subjects (125 (115 – 136) vs 118 (108 – 125) mm Hg and 80 (70 – 85) vs 74 (67 – 80) mm Hg; p<0.0001 for both). In contrast, underweight subjects were more likely to be cyanotic (13.1 vs 6.5%; p=0.0009), have complex cardiac disease (33.9 vs 22.4%; p=0.0005) or be more symptomatic (46.3 vs 34.5% NYHA class ≥3; p=0.003) compared with the remaining patients. In addition, a higher BMI was directly correlated with age (ρ=0.27; p<0.0001), systolic (ρ=0.27; p<0.0001) and diastolic blood pressure (ρ=0.31; p<0.0001).
A small minority of patients had underlying syndromes (Down syndrome 1.1%; Di George 0.7%; Noonan or Turner syndrome 0.1%). These patients had significantly lower body weight (60.8 (55.3–73.4) vs 70.1 (60.1–82.3) kg; p<0.0001) and height (160 (148 – 168) vs 170 (163 – 178) cm; p<0.0001) but similar BMI (25.2 (21.3–27.7) vs 24.0 (21.4–27.5) kg/m²; p=0.27) compared with the remainder. The highest proportion of underweight patients was in Eisenmenger syndrome (16.0%), followed by patients with a Fontan palliation (12.0%), patients after arterial switch operation for transposition of the great arteries (9.2%) and other complex cardiac defects (8.7%). In contrast, the highest rate of obese patients was seen in patients with atrial septal defect (19.1%), followed by atrioventricular septal defect (18.0%), valve/outflow tract disease (17.4%) and tetralogy of Fallot (15.1%).
Demographics and baseline characteristics of the study population
Association between weight, BMI and mortality
Over a median follow-up period of 2.54 years (IQR 0.65–5.31 years) 178 patients (5.8%) died. The majority died due to cardiac causes (n=121), while the leading non-cardiac causes of death were pneumonia (n=10), haemorrhage (n=10), cancer (n=7), sepsis (n=7) and cerebrovascular accidents (n=5). On univariable Cox proportional hazards analysis, a higher patient weight (HR 0.984 (95% CI 0.975 to 0.993)/kg; p=0.0007) and a higher BMI (HR 0.963 (95% CI 0.933 to 0.994)/kg/m²; p=0.02) were associated with better outcomes (figure 1). A higher BMI was associated with lower all-cause mortality in symptomatic patients (ie, NYHA 2 and above) and in those with complex underlying congenital cardiac defect (figure 2). A trend towards lower mortality at higher BMI values was seen in patients with cyanosis and those with medium complexity cardiac defects.
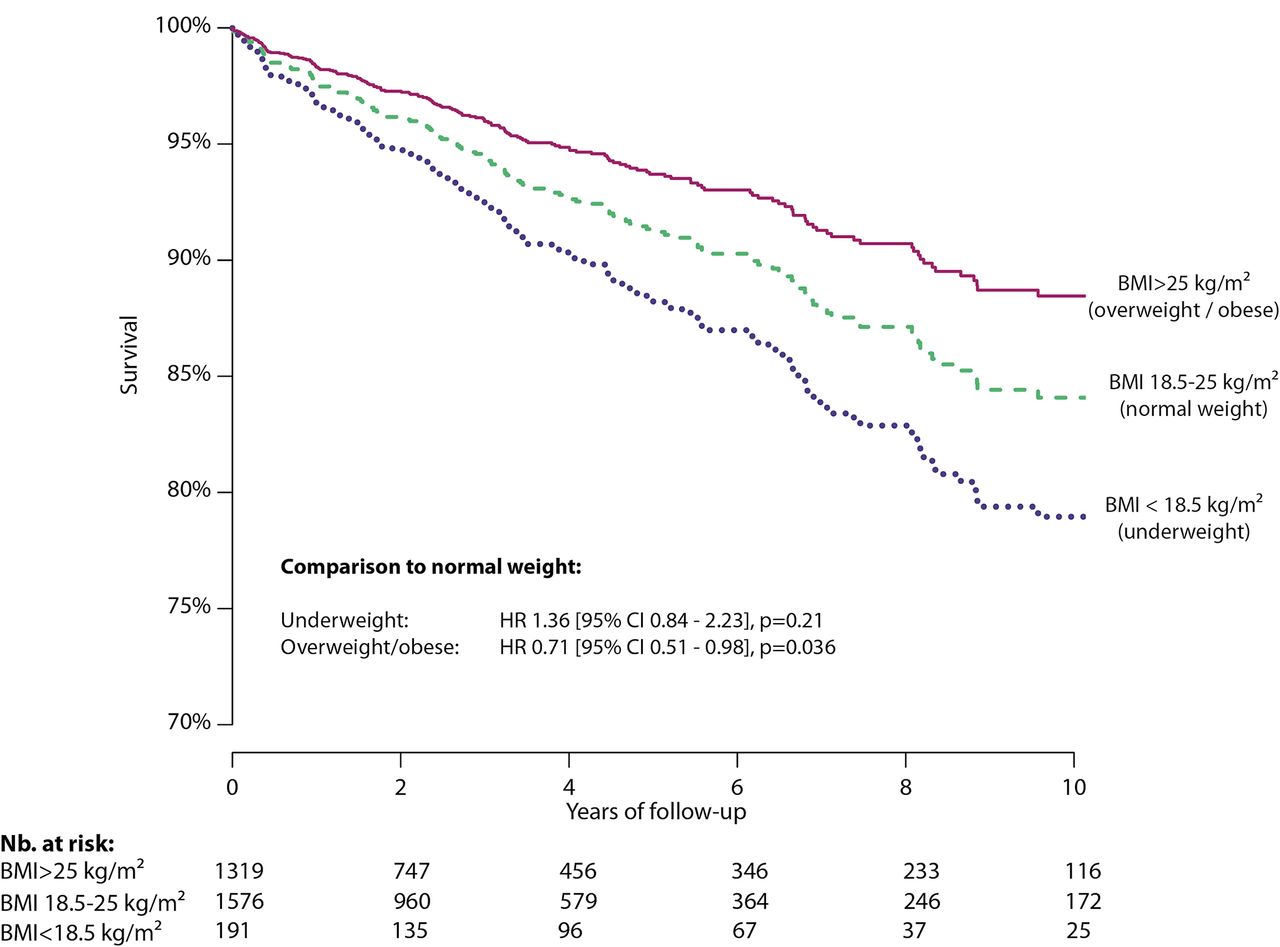
Survival by body mass index (BMI, kg/m²) based on the results of the Cox analysis. Compared with normal weight patients (ie, BMI 18.5–25 kg/m²), underweight patients tended to have worse outcome, while overweight/obese patients as a group had on average a significantly superior prognosis.

HR of death (all-cause mortality) stratified by the presence of cyanosis, complexity of heart disease and symptoms (NYHA functional class>1). HRs with 95% CI are presented. NYHA, New York Heart Association.
Closer inspection of the association between BMI and outcome revealed a non-linear, U-shaped relationship. The lowest risk of mortality was formally observed at a BMI of 34.1 kg/m². When the median BMI of 24 kg/m² was used as a reference value, the relative hazard of death was increased for BMI values below this threshold but was lower for patients with a BMI between 24 kg/m² and approximately 30 kg/m². Only, severely obese patients had higher relative risk compared with those with a median BMI (figure 3).

Association between HR of death and BMI as a continuous variable, illustrating excess mortality in underweight and severely obese patients. The median BMI of the population (24 kg/m²) was set as the reference value.
In addition to weight and BMI, age, disease complexity, cyanosis, higher NYHA functional class, pVO2 (both absolute and percentage predicted) and VE/VCO2 slope were significantly associated with all-cause mortality on univariable Cox analysis in the study population. Systolic and diastolic blood pressure did not show significant association with all-cause mortality (table 2).
Univariable predictors of all-cause mortality
On multivariable analysis, BMI emerged as a significant predictor of outcome independently of age, complexity, cyanosis, NYHA class and pVO2 (table 3). Logarithmic or quadratic transformation of BMI to account for a non-linear association between BMI and outcome did not alter the results of the analysis. Similarly to all-cause mortality, a higher BMI was associated with lower cardiac mortality on univariable (HR 0.958 (95% CI 0.922 to 0.996)/kg/m², p=0.03) and multivariable (HR 0.953 (95% CI 0.908 to 0.999)/kg/m², p=0.047) Cox proportional hazards analysis.
Multivariable predictors of all-cause mortality
Longitudinal association between weight changes and mortality
Repeated weight measures were available in 1757 patients. The median time between weight measurements was 2.87 years (IQR 1.36–4.40 years). The median change in weight between the two most recent weight measurements was only+0.31 kg/year of follow-up (IQR −0.40–1.46 kg/year of follow-up). Therefore, we compared those patients who maintained or increased their weight between these last two weight measurements with those who exhibited a weight loss. Weight loss was associated with a significantly higher mortality in patients with complex underlying cardiac defects (HR 1.82 (95% CI 1.02 to 3.24), p=0.04) (figure 4). The association between weight loss and worse outcome in complex patients was confirmed when the difference between last weight and median body weight during the study period was assessed on Cox analysis (HR 1.04 (95% CI 1.002 to 1.08) per kg negative weight difference between last weight and median weight, p=0.04). In contrast, no association between weight loss and outcome could be established in patients with simple or moderate cardiac complexity (p=0.89 and p=0.29, respectively).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival of patient with repeated weight measurements stratified by complexity of underlying heart disease modelled based on the results of Cox proportional hazards analysis. Patients were split by those with and without weight loss between repeated measurements. HRs and 95% CI are provided.
Discussion
To our knowledge, this is the first report investigating the association between BMI and outcome in ACHD patients. Including more than 3000 patients followed at a single tertiary ACHD centre, we found that higher BMI was associated with a lower mortality, especially in symptomatic ACHD patients and in those with complex underlying heart defects, while underweight patients had a worse outcome. This association was independent of patient age, symptoms, cardiopulmonary exercise capacity and defect complexity. In addition, using repeated weight measurements in a subgroup of patients we show that weight loss was related to an increased risk of death in patients with complex cardiac defects.
Obesity in the general population and ACHD
The increasing prevalence of obesity is a recognised problem in most western societies.17 Obesity is risk factor for the development of cardiovascular disease, including coronary artery disease17 and HF.2 Alarmingly, ACHD patients share the hallmarks of HF in general, including exercise intolerance, increased levels of neurohormones and inflammatory markers.18 Furthermore, HF remains a leading cause of death in ACHD patients with its impact on mortality continuing to increase.19 This is due to an ageing population with increasingly complex congenital heart disease accompanied by the lack of effective HF treatment options. Although rare below 40 years of age, coronary heart disease is emerging as an important cardiac comorbidity in elderly ACHD patients and may also contribute to increased morbidity and mortality.20 Recent data suggest that metabolic syndrome is more common among ACHD patients than in the general population.21 As a consequence, it appears prudent and timely to be concerned about the potential detrimental impact of overweight/obesity on cardiac function and late outcome, especially in the sickest patient subgroups with ACHD.6 22 23 On the other hand, higher BMI values have been consistently linked to superior outcome in the setting of established HF due to acquired heart disease. Against this background, the current study clarifies the prognostic impact of BMI in ACHD during short-term and midterm follow-up. It raises the question of optimal weight management in the setting of ACHD, suggesting that the weight associated with lowest mortality may be dependent on the type and severity of underlying heart disease.
Prognostic value of BMI and ACHD
While asymptomatic ACHD patients and those with simple congenital heart defects seem to resemble the general (primary prevention) population, potentially benefiting from lower body weight, it appears that complex, symptomatic ACHD patients may fare better when maintaining a higher BMI similarly to patients with HF due to acquired heart disease. Indeed, in these patients the obesity paradox seems to be present in both those with reduced and preserved ventricular systolic function.24 The reasons for this association are not clear but may be linked to a higher metabolic reserve in the setting of consuming chronic disease. Furthermore, adipose tissue has been demonstrated to be a source of various progenitor cells and this could have beneficial impact in a subset of patients.25 We have previously demonstrated that ACHD patients with complex, cyanotic disease have reduced levels of endothelial progenitor cells.26 Based on our results, we do not advocate active weight gain or unhealthy lifestyle in ACHD patients but rather aim to draw attention to the counter-intuitive association between higher BMI and better outcome especially in the most vulnerable groups of patients with complex, symptomatic and cyanotic disease. In fact, our data do not support the notion that weight gain per se is associated with better outcome. All ACHD patients should be advised to remain active and lead a healthy lifestyle. This is especially true for patients with simple or moderate complexity cardiac defects. The importance of regular exercise and physical activity is supported by the notion that a higher pVO2 has been related to improved outcome independently of complexity of disease in previous studies, and had prognostic value independently of BMI in the current study.13 14 Furthermore, the association between BMI and outcome was independent of pVO2 in the current study, suggesting that mildly overweight patients with preserved exercise capacity may in fact have the best prognosis in the setting of ACHD.
Non-linear association between BMI and outcome
The associations between underweight or cachexia and poor outcome have long been established as a risk factor for mortality in patients with chronic disease and HF22 27 and are, thus, not entirely surprising in the setting of ACHD. It is also plausible that patients at the highest end of the BMI spectrum (ie, morbid obesity) have poor survival prospects. Inspecting the resulting U-shaped relationship between BMI and all-cause mortality, however, reveals remarkably high BMI valued of 24–30 kg/m² to be associated with lowest overall mortality. These values (in the overweight/mild obesity range) should be interpreted with care, as the CIs are wide especially in obese subjects. In addition, the association may not hold especially in asymptomatic patients with corrected simple underlying defects as mentioned above. Of course, morbidly obese patients require special attention as they may benefit from specific intervention such as bariatric surgery to avoid metabolic syndrome and higher complication risks during required cardiac interventions and surgery.28 Overall, genetic aspects may also require further attention as it has been reported that BMI is highly determined by genetic factors.29 Therefore, it is possible—although speculative—that similar genes modify the propensity for obesity and act as protective factors in the setting of congenital heart disease.
Weight loss in ACHD
The association between weight loss and worse survival in patients with complex heart disease is especially intriguing. This is because, unlike the cross-sectional association between BMI and outcome, it illustrates that temporal changes in body weight may also provide prognostic information. Patients included in our study had weight measurements during routine, ambulatory appointments to avoid potential confounding effect of weight loss caused by reduction of oedema in hospitalised, decompensated patients on diuretic therapy. This finding is consistent with previous studies in the setting of HF. Wasting and cardiac cachexia have long been recognised as detrimental signs in the setting of chronic disease and this is confirmed in ACHD patients.
Limitations
Despite the large patient population, including follow-up times of up to 15 years, the median follow-up time was too short to comment on the possible association between adiposity and late sequelae, such as coronary heart disease and ischaemic stroke that may manifest at an older age. We are, thus, careful to comment on long-term impacts of BMI in this patient population with a median age of 32.6 years. Further long-term studies are therefore required to elucidate the association between body weight and atherosclerotic complications in ACHD patients. While BMI is the most widely used and accepted measure of obesity, it does not account for the wide variation in body fat distribution, body composition and may not reflect the associated health risk in different individuals and populations.2 16 30 Moreover, diuretic therapy could account for weight loss and bias the analysis in the most severely affected patients with cardiac decompensation. However, all patients included here had weight measurements as part of routine appointments rather than being admitted in a decompensated state. Therefore, it is unlikely that results are biased by decompensated, complex patients on diuretic therapy. Outcome was based on mortality in this study, while morbidity was not assessed. This may be increased in overweight patients despite a better survival. Also, the association between BMI and different adverse concomitant features that may influence the outcome, such as smoking and diabetes, has not been addressed in this study. Although our results were robust to adjustment for symptoms, disease complexity, cyanosis and cardiopulmonary exercise capacity, we cannot exclude the possibility that reverse causation plays a role in this setting. One may argue that patients with less severe disease could have a higher potential for weight gain, while patients with severe HF or consuming disease may be predisposed for cachexia. However, this is unlikely to affect the main result of this study, namely the positive association between body mass and better prognosis, but rather provide a different interpretation for the findings.
Conclusions
A higher BMI was associated with lower mortality in the current study. The association between BMI and outcome was especially pronounced in symptomatic patients with complex underlying cardiac defects. Furthermore, weight loss in this ACHD subgroup was linked to an even higher risk of mortality. Depending on the underlying cardiac defect, symptoms and factors that remain to be assessed (eg, genetic predisposition), the optimal BMI may differ in individual ACHD patients. Although a multitude of reasons may prompt patients towards losing weight or maintaining a normal body weight, including individual well-being and aesthetic considerations, an uncritical approach advising ACHD to lose weight simply to prolong survival is not supported by the current data.
References
Footnotes
Contributor GPD and MB planned and conducted the study and are responsible for the overall content as guarrantors. KD, AK, LS, EL, RAG and AU made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data. HB and MG made substantial contribution in analysis, drafting the article and revising it critically for important intellectual content. All authors gave final approval of the version to be submitted and any revised version.
Funding This study was supported by a research grant from the EMAH Stiftung Karla Voellm, Krefeld, Germany. GPD, AK, KD, MG and the Adult Congenital Heart Centre and Centre for Pulmonary Hypertension, Royal Brompton Hospital, London, UK have received support by Actelion UK, Pfizer UK, GSK UK, the British Heart Foundation and the NIHR Cardiovascular and Respiratory Biomedical Research Units.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.