Article Text

Abstract
Objective Dabigatran and rivaroxaban are novel oral anticoagulants (NOACs) approved for stroke prevention in atrial fibrillation (AF). Although NOACs are more convenient than warfarin, their lack of monitoring may predispose patients to non-persistence. Limited information is available on NOAC non-persistence rates and related clinical outcomes in clinical practice.
Methods We conducted a retrospective cohort study using administrative data from Ontario, Canada, from January 1998 to March 2014 of patients with AF who were dispensed dabigatran or rivaroxaban. Non-persistence was defined as a gap in dabigatran or rivaroxaban prescriptions ≥14 days. A multivariable Cox proportional hazards model was used to estimate the primary composite outcome of stroke, transient ischaemic attack (TIA) and mortality associated with non-persistence.
Results The cohort consisted of 15 857 dabigatran (age 80.7±6.7 year) and 10 119 rivaroxaban users (age 77.0±7.1 year) with women comprising 52% of each medication group. At 6 months, 36.4% of patients were non-persistent to dabigatran, while 31.9% of patients were non-persistent to rivaroxaban. Stroke/TIA/death was significantly higher for those non-persistent to dabigatran (HR 1.76 (95% CI 1.60 to 1.94); p<0.0001) or rivaroxaban (HR 1.89 (95% CI 1.64 to 2.19); p<0.0001) compared with those who were persistent. Risk of stroke/TIA was markedly higher in non-persistent patients to dabigatran (HR 3.75 (95% CI 2.59 to 5.43); p<0.0001) and rivaroxaban (HR 6.25 (95% CI 3.37 to 11.58); p<0.0001) than those persistent.
Conclusions NOAC non-persistence rates are high in clinical practice, with approximately one in three patients becoming non-persistent to dabigatran or rivaroxaban within 6 months after drug initiation. Non-persistence with either dabigatran or rivaroxaban is significantly associated with worse clinical outcomes of stroke/TIA/death.
- Atrial fibrillation
- Medication adherence
- Quality and outcomes of care
- Cardiac arrhythmias
- Resuscitation science
- Diseases
- Health services
- Research approaches
Statistics from Altmetric.com
- Atrial fibrillation
- Medication adherence
- Quality and outcomes of care
- Cardiac arrhythmias
- Resuscitation science
- Diseases
- Health services
- Research approaches
Introduction
Antithrombotics are essential therapy in atrial fibrillation (AF) to prevent stroke and systemic embolism in high-risk patients.1 Adherence with prescribed antithrombotics is vital to the effectiveness of these agents for AF stroke prevention. Lack of adherence with warfarin has long been recognised in clinical practice, and is thought to be due to the inconvenience of frequent warfarin monitoring, dietary restrictions and numerous drug interactions.1 2 Dabigatran and rivaroxaban are novel oral anticoagulants (NOACs) that in pivotal randomised trials were non-inferior to warfarin for stroke and systemic embolism prevention, with dabigatran 150 mg twice daily superior for this outcome.3 4 For this same degree of efficacy of NOACs to be translated into clinical practice, it is imperative that patients are as adherent with NOACs in the real-world setting as they were in clinical trials. Although the lack of routine monitoring with NOACs may be seen as an advantage, patients taking NOACs may have less contact with clinicians, providers may be less aware of patients’ medication-taking behaviours, and, therefore, NOAC non-persistence may be anticipated in clinical practice.5
In the RE-LY trial, 1-year discontinuation rates for dabigatran were 15%–16% at 1 year, while in ROCKET-AF, 2-year rivaroxaban permanent discontinuation rates were 23.7% and any discontinuation was 57%.3 4 6 Non-persistence is often higher in real-world settings compared with clinical trials due to the higher intensity of oversight and monitoring that patients receive in clinical trials. Currently, the information available on NOAC non-persistence in clinical practice from studies examining individual agents shows that 23%–49% of patients are non-persistent with dabigatran and 19%–42% of patients are non-persistent to rivaroxaban.6–12 It is important to determine whether NOAC adherence rates are similar to those in the landmark clinical trials, or whether we find higher non-persistence in clinical practice. Furthermore, it is essential to determine whether NOAC non-persistence in clinical practice is associated with adverse clinical outcomes. Non-persistence with chronic medications are often highest early in therapy, as we have previously shown with statins.13 Therefore, our study objective is to ascertain rates of dabigatran and rivaroxaban non-persistence, and associated clinical outcomes, early after drug initiation, in a large, population-based cohort of older patients with AF.
Methods
Study design and data sources
We conducted a retrospective cohort study using linked administrative data from hospital admissions and prescription claims from Ontario, Canada between 1 January 1998 and 31 March 2014. In 2015, Ontario had a population of about 13.8 million, of whom ~2.2 million were 65 years and older. This latter group has universal access to acute hospital services, physicians’ services, and prescription medications covered by the provincial formulary. Low income patients pay a maximum of $C2 copayment per prescription, and higher income seniors pay $C100 annual deductible, then a maximum of $C6.11 copayment per prescription, with no copayment differential for brand/generic products. Hospital administrative databases in Ontario include data on all admissions to acute care hospitals. Unique encrypted patient identifiers allow linkage between hospitalisation records and prescription claims databases. Data on diagnosis and related procedures of patients were obtained from the government hospital discharge database, the Canadian Institute for Health Information (CIHI). Most responsible primary and secondary diagnoses are coded using the International Classification of Disease 9th Revision or 10th Revision codes (ICD 9/10). Information on patients’ outpatient prescription medications were obtained from the provincial drug claims database, the Ontario Drug Benefit Plan, which is the drug plan for patients aged ≥65 years. Vital status was obtained from the Ontario Registered Persons and CIHI databases.
Study population
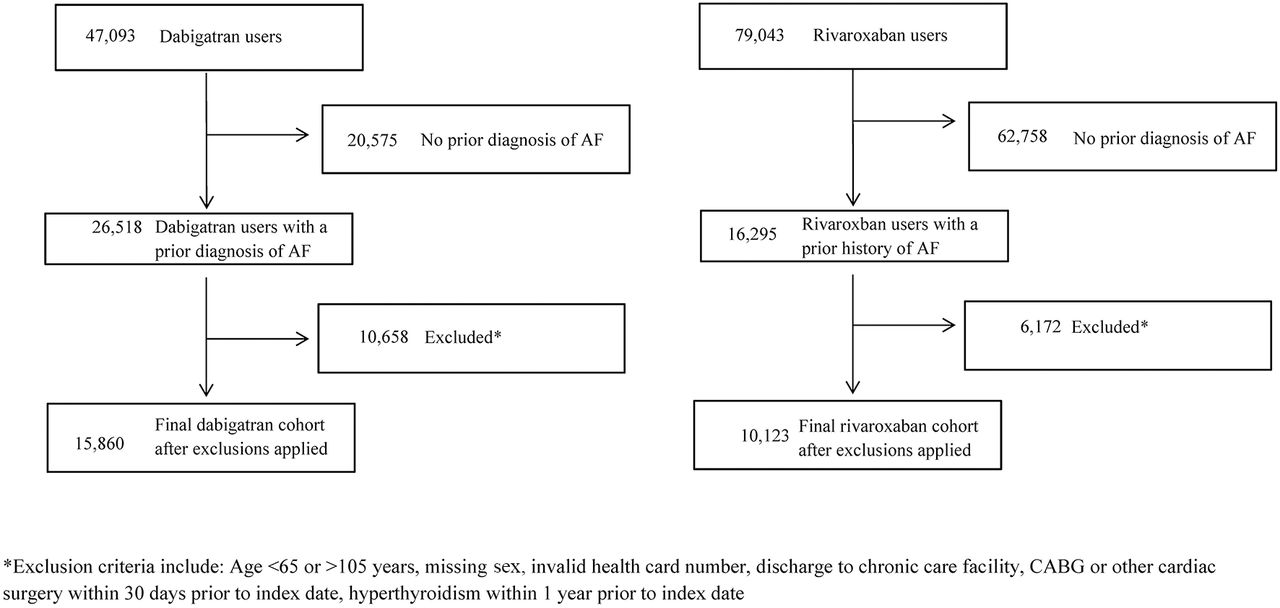
The cohort was constructed with the inclusion of all patients who were discharged alive from hospital with a most responsible diagnosis of AF or a major comorbid diagnosis (secondary diagnosis) of AF (ICD-9/10 revision, codes 427.3, 427.31 or 427.32/I48) between 1 January 1998 and 1 March 2014. The analysis was restricted to patients aged ≥65 years due to availability of prescription claims data. Use of dabigatran and rivaroxaban was ascertained using drug identification numbers identified in the prescription claims database, which has been determined to be a reliable source of drug utilisation.14 Dabigatran and rivaroxaban were available on formulary as of April 2012 and July 2012, respectively; therefore, all patients were new users of these agents under study. Apixaban was available on formulary as of August 2013, and edoxaban is not available in Canada. All patients who had one or more dabigatran or one or more rivaroxaban prescriptions between 1 April 2012 and 31 March 2014 and had an AF diagnosis between 1998 and 2014 that was prior to the NOAC prescription were included in the cohort. We excluded apixaban as a separate cohort due to its late addition to formulary resulting in insufficient follow-up duration (figure 1).

Flow chart of dabigatran and rivaroxaban cohorts.
Non-persistence measure
Patients were categorised into two separate exposure cohorts, according to whether they initiated dabigatran or rivaroxaban. Therefore, we could compare the impact of non-persistence within each cohort, that is, compare patients persistent versus non-persistent to dabigatran, and separately, compare patients persistent versus non-persistent to rivaroxaban. Date of first dabigatran or rivaroxaban-filled prescription after first AF hospitalisation was set to be the index date. Patients were considered non-persistent if there was a gap of 14 days or greater between dabigatran prescriptions for those originally in the dabigatran cohort, with analogous methods for the rivaroxaban cohort.15–17 Dabigatran is a reversible, direct thrombin inhibitor, with a half-life of 12–17 hours in healthy subjects; most patients eliminate >95% of the drug within 4 days.18 19 Rivaroxaban is a reversible, direct factor Xa inhibitor with a half-life of 5–9 hours in healthy subjects and 11–13 hours in the elderly.20 Given the short half-lives of these agents (much shorter than warfarin) and a clear correlation between plasma drug concentrations and degree of anticoagulant effect, stopping dabigatran or rivaroxaban for 14 or more days is considered a clinically meaningful gap in anticoagulation therapy, at which point an increased risk of thromboembolic events might be expected to occur.18–20 We conducted a sensitivity analysis with non-persistence defined as a gap of ≥30 days between prescriptions. For those patients who had 6 months total duration of follow-up available, we also determined the proportion of patients who adhered continuously without gaps of 14 days or greater to calculate a time-specific 6-month non-persistence rate. We also examined oral anticoagulant filling patterns following dabigatran/rivaroxaban non-persistence, including, restarting the same agent, switching between dabigatran and rivaroxaban and from dabigatran/rivaroxaban to warfarin or apixaban.
Outcomes
The primary clinical outcome was a composite of stroke, transient ischaemic attack (TIA) or death, using ICD 9/10 codes (stroke/TIA (362.3, 434, 435, 436, G45, excluding G45.4, H34.1, I63, I64)). We also estimated the events of stroke/TIA as a secondary outcome. We compared outcomes between those persistent and non-persistent to dabigatran and compared those persistent and non-persistent to rivaroxaban. Follow-up for outcomes in the non-persistent group started at the time of non-persistence of the dabigatran/rivaroxaban prescription and continued until the outcome was reached or the end of the study period. In this way, we ensured that outcomes were only attributed to the non-persistent group after they became non-persistent.
Statistical analysis
We used descriptive statistics to describe the baseline characteristics of the cohort. For all patients regardless of follow-up duration, we determined the mean time ±SD to dabigatran/rivaroxaban non-persistence, censoring for death and end of the study period. We constructed multivariable logistic regression models to identify whether age, sex, rural residence, education level, prior warfarin use, CHADS2 score, chronic kidney disease, physician type, hypertension, coronary artery disease, diabetes, prior stroke/TIA or prior history of bleeding were significant risk factors for dabigatran/rivaroxaban non-persistence.
We constructed multivariable Cox proportional hazards models for the clinical outcomes to evaluate the association with dabigatran/rivaroxaban non-persistence. Patients were considered non-persistent if there was a gap of 14 or more days between dabigatran prescriptions for those originally in the dabigatran cohort, with analogous methods for the rivaroxaban cohort. The Cox model was adjusted for the following covariates: age at index date, sex, rural residence, education, most responsible physician specially from AF hospitalisation, comorbidities (hypertension, coronary artery disease, heart failure, diabetes, cerebrovascular disease, bleeding history, depression (as identified by antidepressant use within 1 year prior to the index date)), number of concomitant medications in 90 days prior to first dabigatran/rivaroxaban prescription, number of different physicians seen in year prior to dabigatran/rivaroxaban prescription, time since first AF diagnosis and length of index AF hospitalisation. Covariates were obtained from hospital discharge abstracts from the most recent hospital admission (median time between admission and index date of 959 days and 902 days in the dabigatran and rivaroxaban cohorts, respectively), unless specified otherwise, and concomitant medications were obtained from the prescription claim databases for the specified time frames prior to the index date of first dabigatran/rivaroxaban prescription. We conducted a sensitivity analysis using propensity score-adjusted Cox proportional hazards models for each medication for the composite and cerebrovascular outcomes. The propensity score was developed with the covariates used in the non-persistence predictor model, with the propensity score added as a covariate to the Cox models. We also conducted sensitivity analyses of warfarin naïve versus prior warfarin user subgroups to determine if prior experience with an anticoagulant was associated with improved outcomes.
Statistical analyses were performed using SAS V.9.3. All statistical tests were two sided and a p value <0.05 was considered statistically significant. The study received institutional review board approval from McGill University, Western University of Health Sciences, and Sunnybrook Health Sciences Centre.
Results
The cohort consisted of 15 857 dabigatran users and 10 119 rivaroxaban users, with women comprising 52% of each medication group. Mean age was 80.7±6.7 years for dabigatran and 77.0±7.1 years for rivaroxaban patients. Common comorbidities included hypertension, coronary artery disease, diabetes and heart failure. High-risk CHADS2 scores (score ≥2) occurred in 63.4% of dabigatran users and 64.3% of rivaroxaban users. More than half of patients were prior warfarin users in the last year before being dispensed dabigatran (52.6%) or rivaroxaban (55.7%) (table 1).
Patients characteristics at baseline
For those with 6 months follow-up, 6-month non-persistence was 36.4% for dabigatran and 31.9% for rivaroxaban (p<0.001 between groups). Median time to non-persistence was 240 days (IQR: 78–523) for dabigatran and 140 days (IQR: 52–283) for rivaroxaban for all patients started on these agents. After non-persistence according to our 14-day gap definition, all patients were tracked for subsequent anticoagulant drug prescriptions for the duration of follow-up. In those who were non-persistent to dabigatran, 11.6% switched to warfarin, 5.6% switched to rivaroxaban, 0.9% switched to apixaban, 8.9% completely stopped all anticoagulant therapy and 73.0% restarted dabigatran. In those who were non-persistent to rivaroxaban, 13.7% switched to warfarin, 3.2% switched to dabigatran, 2.5% switched to apixaban, 17.7% completely stopped all anticoagulant therapy and 62.9% restarted rivaroxaban.
The only significant factor for non-persistence with dabigatran was male sex. Significant factors for rivaroxaban non-persistence were male sex, urban residence (vs rural), no prior warfarin use, no history of prior stroke/TIA and internist rather than a general practitioner prescriber (table 2).
Factors associated with dabigatran and rivaroxaban non-persistence
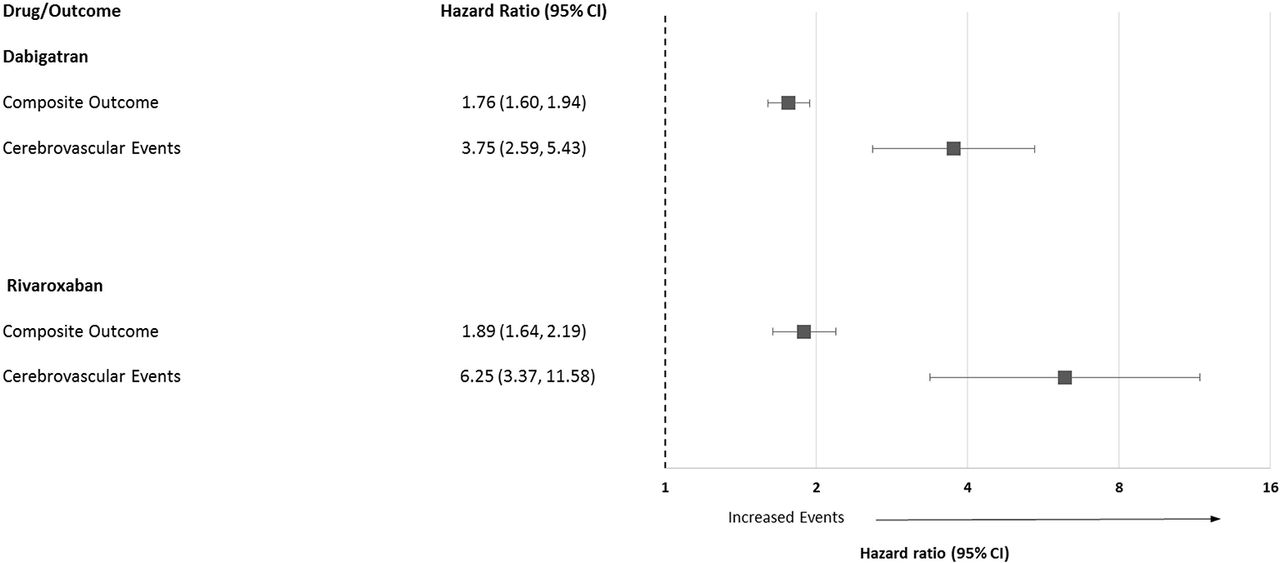
During a mean follow-up of 533 days, 1700 (11.2%) patients died, 130 (0.8%) patients had a cerebrovascular event and 1740 (11.6%) patients had a composite outcome in the dabigatran cohort, while during a mean follow-up of 273 days, 810 (8.5%) patients died, 46 (0.5%) patients had a cerebrovascular event and 817 (8.6%) patients had a composite outcome in the rivaroxaban cohort. Dabigatran non-persistence was associated with a significantly increased risk of the composite of stroke/TIA/death (adjusted HR 1.76 (95% CI 1.60 to 1.93), p<0.0001) compared with those who were persistent to the medication. Dabigatran non-persistence was also associated with a nearly fourfold increased risk of the stroke or TIA (adjusted HR 3.75 (95% CI 2.59 to 5.43), p<0.0001). (table 3, figure 2) Rivaroxaban non-persistence was associated with a significantly increased risk of the composite of stroke/TIA/death (adjusted HR 1.89 (95% CI 1.64 to 2.19), p<0.0001) compared with those who were persistent to the medication. Rivaroxaban non-persistence was also associated with more than sixfold increased risk of the stroke or TIA (adjusted HR 6.25 (95% CI 3.37 to 11.58), p<0.0001, see table 4 and figure 2).
{kind=link}
{kind=link}
Clinical outcomes associated with lack of medication persistence.
Adjusted risk of composite outcome and cerebrovascular event associated with dabigatran non-persistence
Adjusted risk of composite outcome and cerebrovascular event associated with rivaroxaban non-persistence
Sensitivity analysis using the 30-day gap definition of non-persistence found consistent results of the same or greater magnitude of harm as our primary analyses with the 14-day definition. Dabigatran non-persistence using the 30-day gap definition for non-persistence was associated with increased risk of the composite outcome (adjusted HR 1.89 (95% CI 1.71 to 2.08) and stroke/TIA (adjusted HR 4.82 (95% CI 3.31 to 7.02)). Rivaroxaban non-persistence using the 30-day gap definition for non-persistence was associated with increased risk of the composite outcome (adjusted HR 2.18 (95% CI 1.86 to 2.55) and stroke/TIA (adjusted HR 6.17 (95% CI 3.26 to 11.69)). Propensity score-adjusted analyses showed results consistent with our primary analyses.
Subgroup analysis of prior warfarin users versus warfarin-naïve patients found no difference between groups with results consistent with the main study findings. The composite outcome was higher in non-persistent versus persistent patients in the dabigatran cohort (HR 1.77 (CI 1.52 to 2.06) and HR 1.79 (CI 1.59 to 2.02)) for both warfarin-naïve and prior warfarin users, respectively. Cerebrovascular events were also higher in non-persistent versus persistent patients in the dabigatran cohort (HR 2.89 (CI 1.65 to 5.05) and HR 4.55 (CI 2.75 to 7.51)) for both warfarin-naïve and prior warfarin users, respectively. The composite outcome was higher in non-persistent versus persistent patients in the rivaroxaban cohort (HR 2.11 (CI 1.68 to 2.65) and HR 1.80 (CI 1.48 to 2.17)) for both warfarin-naïve and prior warfarin users, respectively. Cerebrovascular events were also higher in non-persistent versus persistent patients in the rivaroxaban cohort (HR 5.24 (CI 2.07 to 13.28) and HR 7.22 (CI 3.13, 16.65)) for both warfarin-naïve and prior warfarin users, respectively.
Discussion
Our study found high rates of early non-persistence with dabigatran and rivaroxaban in clinical practice which was associated with adverse clinical outcomes. Approximately one in three patients was non-persistent to NOAC therapy within the first 6 months after initiation, in a clinical practice setting with minimal prescription cost burden for patients. Non-persistence rates with dabigatran were only slightly higher compared with rivaroxaban. At 36%, our 6-month dabigatran non-persistence rate is double the discontinuation rate of 15% seen with dabigatran in the RE-LY trial at 1 year, yet our 32% rivaroxaban 6-month non-persistence is only slightly higher than the annualised discontinuation rate of 29% with rivaroxaban reported in ROCKET-AF.3 4 Our findings are consistent with that shown in other populations, where rivaroxaban non-persistence rates of 19%–42% were generally higher in clinical practice than in the clinical trial setting, while dabigatran non-persistence rates of 23%–49% in clinical practice markedly exceeded that found in the strictly monitored setting of a clinical trial.6–12
The twice-daily dosing and frequent gastrointestinal side effects may contribute to dabigatran non-persistence in our study. It is recognised that as frequency of drug administration increases, non-persistence with medication use declines.21 A further barrier of dabigatran therapy that may predispose patients to non-persistence is its storage requirements. The Food and Drug Administration and Health Canada approved dabigatran with special storage and product handling requirements.18 19 Since dabigatran is sensitive to moisture, it must be kept in its original bottle or blister packaging.18 19 22 As patients often use pill organisers as a compliance aid, non-persistence with dabigatran may be more likely to occur in elderly AF patients who have a pill organiser system to manage their medications, and are then required to have their dabigatran in a separate bottle, isolated from their personal medication taking system.
However, despite the additional inconveniences of dabigatran compared with rivaroxaban that might be considered to predispose a patient to dabigatran non-persistence, we found a rather small magnitude of difference between dabigatran and rivaroxaban non-persistence. Historically, non-persistence to warfarin was thought to be due to the inconvenience of frequent warfarin monitoring, dietary restrictions and numerous drug interactions, inconveniences that do not occur with dabigatran or rivaroxaban.1 2 However, our data show that early 6-month non-persistence to dabigatran and rivaroxaban are as high as 1-year non-persistence rates of 25%–32% in studies conducted in population-based clinical practice settings with warfarin, including a population-based study in Ontario.23 24 Although NOACs are commonly viewed as more effective and convenient replacements for warfarin, NOAC non-persistence in practice may limit the expected benefits.
In clinical practice, close monitoring is not mandated by guidelines for NOACs, unlike with warfarin, where frequent clinician contact is necessitated due to routine international normalized ratio (INR) monitoring. This lack of regular contact for patients receiving dabigatran or rivaroxaban may improve their convenience, but at the same time, may potentially increase patient’s risk of non-persistence. Without close monitoring and follow-up appointments, as is the norm with warfarin, patients taking NOACs in clinical practice may not actively seek an appointment with their healthcare provider to discuss medication intolerance and side effects, which may lead to drug non-persistence. Bleeding may occur with all anticoagulants, and gastrointestinal side effects have also been reported in clinical practice studies as a potential cause for dabigatran non-persistence, with rates of dyspepsia ranging from 6% to 33%.25 26 A recent study found that enhanced monitoring of patients after initiation through anticoagulation clinics and outpatient pharmacists within the Veterans Health Administration healthcare system for at least 3 months was associated with improved dabigatran adherence.5 The readily available structure of anticoagulation clinics that was established for monitoring warfarin therapy may provide a suitable mechanism for enhanced monitoring of the novel oral anticoagulants with the goal to improve adherence.
The high rate of dabigatran and rivaroxaban non-persistence in our study is especially concerning given that we also found that dabigatran and rivaroxaban non-persistence was associated with approximately an 80% increase in the risk of stroke, TIA or death. Furthermore, there was a four-fold higher risk of stroke/TIA with dabigatran non-persistence, and an even greater, sixfold increased risk of stroke/TIA with rivaroxaban non-persistence. We defined non-persistence as a 14-day gap in therapy and confirmed our findings as robust in our 30-day sensitivity analysis. Intermittent gaps in therapy, as per our non-persistence definition, were associated with adverse clinical outcomes. Our findings are consistent with the post-hoc ROCKET-AF analysis that found temporary interruption of rivaroxaban or warfarin was associated with increased risk of stroke events.27
After rivaroxaban non-persistence, a lower proportion of patients restarted rivaroxaban. In addition, there were nearly twice as many non-adherent rivaroxaban patients who completely stopped all anticoagulation therapy compared with dabigatran (17.7% vs 8.9%). This lack of stroke prevention with anticoagulation therapy after rivaroxaban non-persistence may have been related to reluctance to use anticoagulation in less healthy patients, and may have translated into the especially high risk of adverse cerebrovascular events, stroke and TIA, that we found in rivaroxaban non-adherers. While it is not known why patients were less likely to restart rivaroxaban than dabigatran after becoming non-persistent, it is possible for clinicians to monitor for non-persistence and consider the possible stroke prevention therapies in suitable patients to help reduce the risk of adverse clinical outcomes.
Our study reports the association between dabigatran and rivaroxaban non-persistence and adverse cardiovascular outcomes in a large diverse AF population. For the same level of efficacy of dabigatran in the RE-LY trial and rivaroxaban in the ROCKET-AF trial to be translated into clinical practice, the same level of dabigatran and rivaroxaban adherence in the real-world setting is needed. We have found higher levels of non-persistence in clinical practice, so it cannot be presumed that these NOACs will be as effective in clinical practice as was found in the landmark clinical trials. Our study with both dabigatran and rivaroxaban expands on prior research that found dabigatran non-persistence to be associated with increased risk of stroke and death in male veterans.28 We also found that both a 14-day and a 30-day gap was associated with adverse clinical outcomes, while others have found that stroke risk in patients with AF is correlated with length of NOAC non-persistence (gaps in anticoagulation therapy) and baseline CHADS2 scores.12 Adherence to cardiovascular medications is crucial to achieve expected clinical outcomes seen in clinical trials.29 30 Non-persistence with other cardiovascular medications, such as, statins and antihypertensives has been estimated to increase the risk of adverse cardiovascular disease events from approximately 40% to 80%.30 Our increased risk of stroke/TIA and death with dabigatran and rivaroxaban non-persistence in an AF population is consistent with these findings with other cardiovascular medications.
Our study has some limitations. Our measure of non-persistence relied on prescription claims for dabigatran and rivaroxaban in the administrative database. It is possible that patients who fill dabigatran or rivaroxaban prescriptions do not take their medications. However, prescription claims have been considered a suitable measure of medication non-persistence.13 Our study focused on early medication adherence. Rates of longer term adherence may show different patterns. The follow-up time was longer for persistent patients than non-persistent patients in both the dabigatran and rivaroxaban cohorts, which may result in an underestimation in the risk of stroke/TIA/death. While we adjusted for known confounders, it is possible that unknown or unmeasured confounders could be associated with both non-persistence and the outcomes of interest. While our study focuses on anticoagulation use, it is possible that some patients who were non-persistent may have switched to aspirin therapy. Since aspirin is available without a prescription, we could not track aspirin use accurately and aspirin use is not accounted for. Due to the use of administrative data, we can only hypothesise as to potential reasons for lack of adherence with dabigatran or rivaroxaban therapy. Future studies should be conducted to determine actual barriers to dabigatran and rivaroxaban adherence.
In summary, approximately one in three patients becomes non-persistent to dabigatran and rivaroxaban within 6 months. Dabigatran and rivaroxaban non-persistence rates in clinical practice are higher than those reported in the landmark AF stroke prevention clinical trials. Patients who were non-persistent to dabigatran and rivaroxaban therapy had a significantly higher risk of stroke/TIA/death than patients who remained persistent. Greater awareness by clinicians of possible dabigatran and rivaroxaban non-persistence, coupled with closer monitoring by anticoagulation clinics and pharmacists may be warranted to prevent premature discontinuation of therapy and associated adverse clinical outcomes.
Key messages
What is already known on this subject?
One-year non-persistence with dabigatran or rivaroxaban is 20–50%; dabigatran non-persistence is associated with stroke risk in male veterans.
What might this study add?
One in three patients is non-persistent within 6 months of starting dabigatran or rivaroxaban, and this non-persistence in routine clinical practice is significantly associated with an 80% increased risk of stroke/transient ischaemic attack/death in a broad atrial fibrillation population.
How might this impact on clinical practice?
Greater awareness of the potential for non-persistence by clinicians and closer monitoring by anticoagulation clinics and pharmacists may be warranted to prevent premature non-persistence and associated adverse clinical outcomes.
References
Footnotes
Contributors Study concept and design: CAJ, LP. Acquisition of data, integrity of data and accuracy of the data analysis, drafting of the manuscript and study supervision: CAJ. Analysis and interpretation of data: CAJ, LP, MAT, VE, MJE, ER, KHH, JVT, CA, MJE, LL, PMH, MT, HB, and LZ. Critical revision of the manuscript for important intellectual content: CAJ, LP, MAT, VE, MJE, ER, KHH, JVT, CA, MJE, LL, PMH, MT, HB, and LZ. Statistical analysis: LZ. Obtaining funding: CAJ, LP.
Funding LP is a James McGill Professor at McGill University. JVT is supported by a Canada Research Chair in Health Services Research and an Eaton Scholar award. MAT has received a fellowship award from CIHR. VE is supported by a Clinician Scientist award from the Canadian Institutes of Health Research. This study was funded by grant DC0190GP from CIHR and from grant 12GRNT8640001 American Heart Association.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.