Article Text

Abstract
Objective In severe aortic valve stenosis (AS), low left ventricular (LV) stroke volume has been associated with increased cardiovascular (CV) mortality, but this association has not been explored during progression of AS in a large prospective study.
Methods In 1671 patients from the Simvastatin Ezetimibe in Aortic Stenosis (SEAS) study, the association of stroke volume indexed for body surface area (SVI) with major CV events during a median of 4.3-year follow-up was assessed in Cox and time-varying Cox regression analyses. Low SVI was defined as <35 mL/m2.
Results Peak aortic jet velocity in the total study population was 3.1 ±0.7 m/s. Low SVI was found in 23% at baseline and associated with higher age, body mass index (BMI), heart rate and global LV load, and with lower mean aortic gradient, aortic valve area index, energy loss index, LV mass and ejection fraction and more often inconsistent AS grading (all p<0.05). A 5 mL/m2 lower SVI at baseline was associated with higher HRs of major CV events (n=544) (HR 1.09, 95% CI 1.05 to 1.13, p<0.001) and higher total mortality (n=147) (HR 1.08, 95% CI 1.01 to 1.16, p=0.038), independent of age, sex, atrial fibrillation, mean aortic gradient, LV ejection fraction, LV mass, BMI and study treatment. Adjusting for the same covariates, low SVI at baseline and in-study low SVI were also associated with increased rate of major CV events.
Conclusion In patients with AS in the SEAS study, lower baseline SVI was associated with higher HR of major CV events and total mortality independent of major confounders.
Trial registration number NCT00092677: Results
- Stroke volume
- Stroke index
- Aortic valve stenosis
- Prognosis
Statistics from Altmetric.com
Introduction
In aortic valve stenosis (AS), low left ventricular (LV) stroke volume index (SVI) may lead to reduced transvalvular flow and subsequent underestimation and inconsistency in grading of AS, even in patients with normal LV ejection fraction.1–3 Both the American College of Cardiology/American Heart Association and the European Society of Cardiology guidelines for the management of AS emphasised the influence of low LV SVI on assessment of AS severity and outcome in patients with severe AS.4 5 Several studies have demonstrated that among patients with symptomatic severe AS, the subgroup with low flow had worse outcome than patients with normal flow, in spite of a normal LV ejection fraction.6–10 Similarly, lower SVI has also been associated with increased CV risk in treated hypertensive patients with electrocardiographic LV hypertrophy, independent of other prognostic factors such as systolic blood pressure, LV mass and geometry, antihypertensive treatment, diastolic function and presence of atrial fibrillation.11
In a previous analysis from the large, prospective Simvastatin Ezetimibe in Aortic Stenosis (SEAS) study, we found that asymptomatic patients with low-gradient ‘severe’ AS had a comparable prognosis to patients with moderate AS irrespective of SVI.12 Thus, in this group of patients with the combination of low mean aortic gradient (<40 mm Hg) and an aortic valve area of <1.0 cm2 in the presence of normal ejection fraction, SVI was not of prognostic implication. However, the association of lower SVI with outcome has not been reported from the total SEAS population. This was the aim of the present analysis.
Methods
Patient population
The SEAS study was a multicenter prospective double-blind, placebo-controlled study in 1873 patients with mild to moderate asymptomatic AS, defined as aortic valve thickening and peak aortic jet velocity ≥2.5 and ≤4.0 m/s randomised to treatment with simvastatin and ezetimibe followed up over a median of 4.3 years.13 Patients with other significant valvular heart disease, systolic heart failure, established coronary, cerebral and/or peripheral vascular disease, diabetes mellitus, planned aortic valve replacement or coronary revascularisation, renal insufficiency, active liver disease, uncontrolled endocrine or metabolic disorders or patients with other indications or contraindications to lipid-lowering therapy were excluded from the study. The study design, patient characteristics and main outcome results have been published previously.13–15 The study was performed in accordance with the Helsinki Declaration. Written informed consent was obtained from all participants, and the study protocol was approved by regional ethics committees in all participating countries.
The present analysis was performed in the 1671 (89%) patients in whom SVI could be assessed on echocardiography at the baseline and at least one follow-up visit (figure 1). Patient characteristics including body composition and laboratory tests were assessed at inclusion and at annual visits, and all laboratory analyses were performed at the central laboratory, PPD Global Central Labs (Zaventum, Belgium).14 Obesity was defined as body mass index (BMI) ≥30 kg/m2 and glomerular filtration rate (GFR) was estimated using the simplified Modification of Diet in Renal Disease formula.
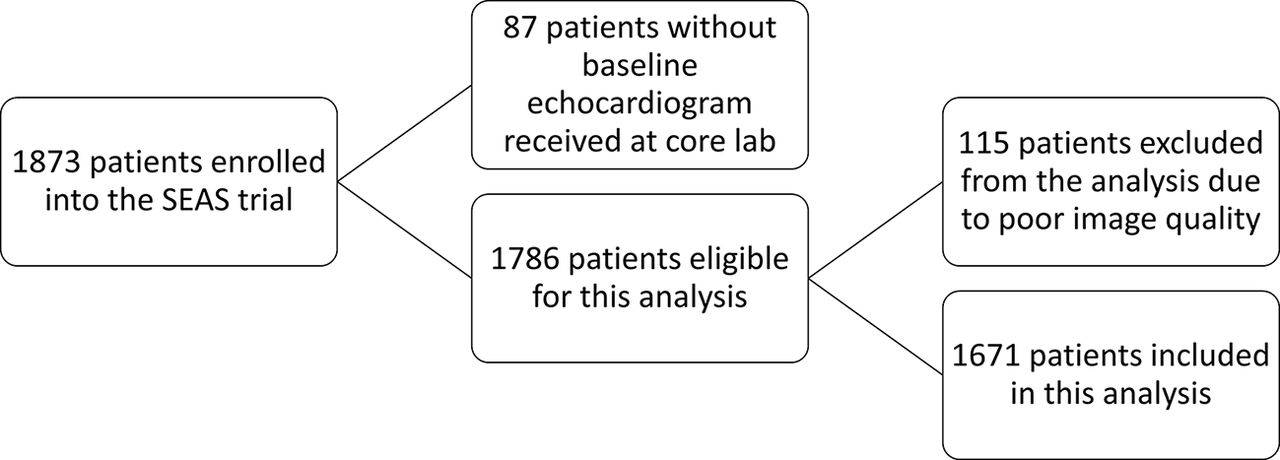
Diagram of the cohort included in this analysis. SEAS, Simvastatin Ezetimibe in Aortic Stenosis.
Echocardiography
Echocardiography was performed at 173 SEAS study sites in seven European countries following a standardised protocol.15 All echocardiograms were interpreted by blinded primary readers and 94% proof read by the same experienced reader at the SEAS echocardiography Core Laboratory at Haukeland University Hospital, Bergen, Norway. Reading was performed off-line on dedicated workstations with Image Arena software (TomTec Imaging Systems GmbH, Unterschleissheim, Germany).
Quantitative echocardiography, including assessment of AS severity, was done following the joint European Association of Echocardiography and American Society of Echocardiography guidelines,4 5 16 and inconsistently graded AS was defined as aortic valve area <1.0 cm2 and mean gradient <40 mm Hg.2 LV hypertrophy was identified by sex-specific cut-off values >46.7 g/m2.7 in women and >49.2 g/m2.7 in men, as previously prognostically validated.17 Energy loss (EL) and energy loss index (ELI) were calculated by previously validated equations.18 SVI was calculated by Doppler and indexed for body surface area. A SVI <35 mL/m2 was defined as low in accordance with current guidelines.4 5 LV function was assessed from LV ejection fraction calculated by the biplane Simpson’s method. Aortic root diameter was measured at the sinotubular junction, and small aortic root was defined using a prognostically validated method.19
Endpoints
All study endpoints were classified by an independent endpoint committee blinded to the study treatment.13 The pre-specified primary SEAS study endpoint was a composite of major CV events, including AS-related events (combined aortic valve replacement, hospitalisation for heart failure due to progression of AS and CV death) and ischaemic CV events (including CV death, nonfatal myocardial infarction, hospitalisation for unstable angina, coronary revascularisation and non-haemorrhagic stroke).14 Secondary endpoints were AS-related events and ischaemic CV events analysed separately. Total mortality was a tertiary study endpoint.
Statistics
Statistical analysis was performed using IBM SPSS, version 23.0. Continuous variables are presented as mean±SD and categorical variables as percentages. Groups with low and normal SVI were compared by t-test and Chi-square statistics as appropriate. Correlates of SVI were identified by Pearson’s correlation coefficients. Kaplan-Meier plots, Cox and time-varying Cox regression analysis were used to assess associations of SVI with hazard rates of major CV events, and censor time was the occurrence of the first event. Cox analyses are reported as HR and 95% CI, and the proportional hazard assumption was met. All models were adjusted for age, sex, atrial fibrillation, mean aortic gradient, LV ejection fraction, LV mass, BMI and study treatment. Cox models assessing CV or all-cause mortality were also adjusted for any preceding aortic valve replacement. In an alternative model, we also adjusted for presence of inconsistently graded AS. In the time-varying Cox regression analysis, changes in SVI, aortic mean gradient, LV mass and ejection fraction during progression of AS was updated at each visit during follow-up. Two-tailed p<0.05 was considered statistically significant in all analyses.
Results
Prevalence and characteristics of low SVI
In the total study population, mean SVI was 44±13 mL/m2 at baseline. Low SVI <35 mL/m2 was identified in 379 patients (23%) at baseline. Patients with low SVI were older, had higher BMI and heart rate and higher prevalence of obesity and atrial fibrillation than those with normal SVI (all p<0.05, table 1). Patients with low SVI had lower mean aortic gradient and LV ejection fraction and lower LV mass despite lower aortic valve area also after adjustment for pressure recovery in the aortic root (table 2). The prevalence of small aortic root did not differ between groups (table 2).
Baseline clinical characteristics for the total study population and group of patients with normal and low SVI
Baseline echocardiographic characteristics of the total study population and group of patients with normal and low SVI
Correlates of SVI
In bivariate correlations, lower SVI was associated with higher age (r=−0.10), BMI (r=−0.10) and heart rate (r=−0.12), and with lower aortic mean gradient (r=0.07), aortic sinus diameter (r=0.09), LV mass index (r=0.08), LV ejection fraction (r=0.07) and ELI (r=0.63, all p<0.01).
SVI and outcome
In patients with primary outcome events during follow-up (n=544), mean age was 68±10 years and 38% were women. Mean BMI was 26.8±4.4 kg/m2, 22% were obese and 77% had hypertension. They had lower SVI, LV ejection fraction and stress-corrected midwall shortening, while LVM and RWT were higher than patients without events (all p<0.05). In addition, peak aortic jet velocity and mean aortic gradient were higher, and AVA and EL were lower compared with patients without events (all p<0.05). In univariate analysis, lower baseline SVI was a significant predictor of higher HRs of major CV events, all-cause mortality, CV mortality, aortic valve related events and combined all-cause mortality and hospitalisation for heart failure (table 3). In Cox regression analysis, adjusting for age, sex, atrial fibrillation, mean aortic gradient, LV ejection fraction, LV mass, BMI and study treatment, lower SVI retained its association with higher HR of major CV events, including aortic valve related events and all-cause mortality (table 3). SVI retained its association with major CV events even after adjusting for inconsistently graded AS. In univariate time-varying Cox regression analysis, taking change in SVI during AS progression into account, lower in-study SVI was associated with increased risk of major CV events, combined all-cause mortality and hospitalisation for heart failure and aortic valve-related events (table 3). After adjusting for covariates including in-study mean aortic gradient, in-study LV ejection fraction, in-study LV mass, age, sex, atrial fibrillation, BMI and study treatment, lower in-study SVI remained a significant predictor of major CV events (table 3).
HR of 5 mL/m2 lower baseline and in-study SVI adjusted for baseline or in-study mean aortic gradient, ejection fraction, LV mass, age, sex, atrial fibrillation, BMI and study treatment, and for CV death and all-cause death also adjusted for aortic valve replacement
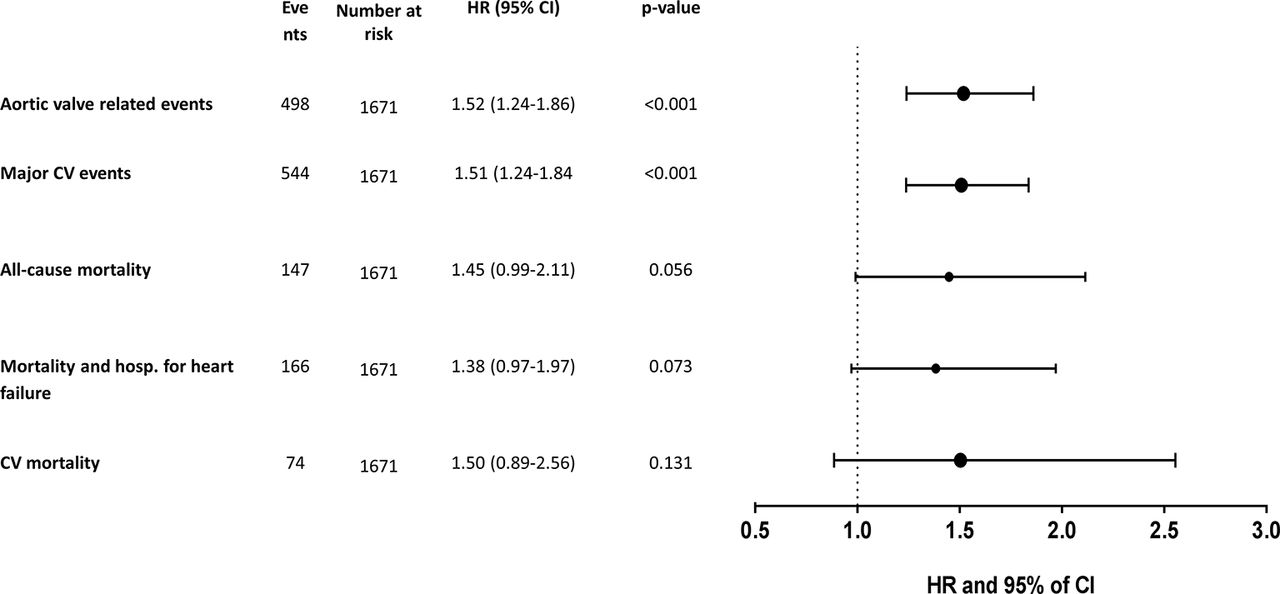
In a secondary set of Cox regression analyses, the association of SVI <35 mL/m2 with outcomes was tested in univariate Cox regression. A SVI <35 mL/m2 at baseline was associated with a reduced event-free survival for major CV events (Log Rank 4.70, p<0.05), while there was no significant association with all-cause mortality (Log Rank 3.67, p=0.055; figure 2). After adjusting for main covariables, a baseline SVI <35 mL/m2 predicted an increased risk of major CV events of 51% (24%–84%; p<0.001), while no significant associations with CV or all-cause mortality were found (figure 3). In similar models, also in-study SVI <35 mL/m2 was associated with a 38% increased risk of major CV events in univariable analysis (HR 1.38, 95% CI 1.10 to 1.74, p<0.05), and a 47% increased risk of major CV events in multivariable analysis (HR 1.47, 95% CI 1.16 to 1.87, p=0.001), while no significant association with all-cause mortality was found.

Kaplan-Meier plot demonstrating event-free survival in patients with low and normal (SVI), respectively.
{kind=link}
{kind=link}
{kind=link}
Multivariate Cox regression of low baseline stroke volume index and association with cardiovascular (CV) events.
Discussion
This study demonstrates that in patients with AS without known diabetes, CV or renal disease participating in the SEAS study, lower SVI at baseline was associated with increased HR of major CV events and all-cause mortality, independent of major confounders, including mean aortic gradient, LV ejection fraction and LV mass.17 20 Secondary analyses also demonstrated that lower in-study SVI and SVI<35 mL/m2 were associated with higher HR of major CV events, expanding previous findings in patients with severe AS6 7 and in patients with essential hypertension and LV hypertrophy.11 These results support the implementation of assessment of SVI in the routine evaluation and follow-up also in asymptomatic patients with milder degrees of AS.
In a previous subgroup analysis from the SEAS trial, including only patients with inconsistently graded AS, with low mean aortic gradient and AVA <1.0 cm2, SVI did not add prognostic information.12 However, paradoxically low-flow low-gradient severe AS, reflecting the clinical entity of severe AS with low SVI, low aortic gradient and normal ejection fraction, has been identified as a high risk group, characterised by concentric remodelling, myocardial fibrosis and increased afterload.6 8 21 Several publications have identified low SVI as a predictor of poor survival in low-flow low-gradient severe AS with preserved LV ejection fraction,7 9 22 and currently low SVI has been implemented as a risk predictor in the guidelines for management of patients with severe AS.4 5 Most recently, Capoulade et al 20 demonstrated that lower LV ejection fraction and lower SVI were the most important echocardiographic predictors of mortality in a retrospective study of 1065 patients with AS. The present large study adds to the finding by Capoulade et al by demonstrating that also in a prospective study of initially mild to moderate AS, lower SVI was associated with increased HR of major CV events as well as higher CV and all-cause mortality, independent of LV ejection fraction, mean aortic gradient and LV mass, although the cut-off value SVI <35 mL/m2 performed less well in our population.
Previous findings, including results from the SEAS trial, highlight that indices of AS severity and LV systolic function18 23 24 and higher LV mass are important in risk stratification in AS.17 In contrast, patients with AS with low SVI in our study were characterised by lower mean aortic gradient and lower LV mass, as could be expected, given the known association between SVI and LV mass. The lower LV mass in the low SVI group is in line with the results from another recent study on LV structure and function in mild-to-moderate AS with normal ejection fraction.25 The finding may reflect maladaptive LV remodelling, characterised by less hypertrophy and more fibrosis and particularly associated with reduced survival in women.26 Future studies in the subgroup of patients with AS with low SVI and normal ejection fraction assessing myocardial function by cardiac MRI or positron emission tomography are needed to fully understand the myocardial dysfunction in this challenging group of patients with AS. The presence of reduced global longitudinal strain and low stress-corrected midwall shortening in low-flow AS reported by others also supports that more severe myocardial disease may be present in such patients despite normal LV ejection fraction.27 However, in the present population of patients with low SVI, LV ejection fraction was significantly lower, while there was no significant difference in stress-corrected midwall shortening between patients with normal or low SVI.
Limitations
Previous haemodynamic studies have demonstrated that SVI assessed by Doppler echocardiography is an accurate and reproducible measurement compared with invasive measurements.28 In line with current guideline recommendations,4 5 Doppler-derived SVI was used in this analysis. However, in AS, correct assessment of SVI by Doppler is challenging. Measurement of aortic valve annular diameter can be difficult in heavy calcified valve cusps. The aortic annulus diameter may also be incorrectly measured by echocardiography assuming that the left LV outflow area is cylindrical, while computer tomography studies have demonstrated that it is often ovoid, and this may lead to underestimation of LV outflow area. Furthermore, correct location of the sample volume for Doppler recording of subvalvular flow may be influenced by pre-stenotic acceleration.29 In addition, LV hypertrophy involving the proximal part of the septum may cause changes in LV outflow tract structure and flow profile contributing to subvalvular increase in velocity, which may cause overestimation of the SVI. In accordance with these caveats, it was recently demonstrated that small LV outflow tract diameter was associated with low SVI,30 as also documented in the present study population. However, presence of a small aortic root did not differ between groups with normal and low SVI in the present study. In addition, patients with other valvular heart diseases were excluded from the SEAS trial; however, concomitant valvular heart disease may be an important confounding factor in assessment of SVI in patients with AS. Nevertheless, SVI assessment by the Doppler-derived method is recommended by current guidelines and is widely used in clinical practice to calculate aortic valve area and EL and in identifying patients with low-flow AS.4
Conclusion
In initially asymptomatic patients with mild-to-moderate AS without known CV disease, diabetes or renal failure, lower SVI was associated with higher all-cause mortality and higher HR of major CV events during a median of 4.3-year follow-up, independent of major confounders such as mean aortic gradient and LV mass. Our results add foundation for the recommendation to include assessment of SVI in risk stratification in AS. However, the optimal way to assess and normalise SVI in the clinical follow-up of patients with AS to avoid overestimation or underestimation of CV risk should be further explored.
Key messages
What is already known on this subject?
Lower stroke volume index (SVI) is an independent prognosticator in hypertensive patients without aortic valve stenosis (AS). In patients with severe AS, paradoxical low flow, low gradient AS with low SVI, low mean aortic gradient and preserved ejection fraction are identified by current guidelines as a clinical entity associated with inconsistency in grading and reduced survival.
What might this study add?
This study demonstrates that also in patients with initial mild-to-moderate AS, lower SVI was associated with an increased risk of major CV events (HR 1.09 pr. 5 mL/m2 lower SVI (95% CI 1.05 to 1.13, p<0.001) and total mortality (HR 1.08 pr. 5 mL/m2 lower SVI (95% CI 1.01 to 1.16, p=0.038), independent of other known risk predictors in AS such as mean aortic gradient, LV ejection fraction and LV mass.
How might this impact on clinical practice?
In management of patients with AS, assessment of SVI should be included in routine echocardiography. Low SVI during follow-up should be regarded as a marker of increased CV risk independent of AS severity and LV ejection fraction.
References
Footnotes
Contributors MTL, GdS and EG were involved in the conception and design as well as analysis and interpretation of data. All coauthors have revised the manuscript critically and approved it for submission to Heart.
Funding The SEAS Echocardiography Core Laboratory was supported by MSP Singapore Company, LLC, a partnership between Merck & Co, Inc, and Schering-Plough Corporation.
Competing interests EG received steering committee honorarium and funding for the echocardiography core laboratory from Merck Schering Plough during the study period 2002–8. KB received steering committee honorarium and speaker honoraria from Merck Schering Plough during the study period 2002–8. ABR received steering committee honorarium from Merck Schering Plough during the study period 2002–8. The other authors have no disclosures related to this study.
Patient consent Written informed consent was obtained from all participants.
Ethics approval Regional ethics committees in all participating countries.
Provenance and peer review Not commissioned; externally peer reviewed.