Article Text

Abstract
Background Apical hypertrophic cardiomyopathy (ApHCM) is considered a ‘benign’ form of hypertrophic cardiomyopathy, with limited data on the long-term outcome. However, the clinical impact of atrial fibrillation (AF) in ApHCM is largely unknown. The hypothesis was that AF is common and has a prognostic implication in ApHCM.
Methods The occurrence of AF and outcome was assessed in 306 consecutive patients with ApHCM (68% male, 62±11 years).
Results AF occurred in 77 patients with ApHCM (prevalence, 25.2%; annual incidence, 4.6%/year) and was independently predicted by old age and large left atrium (>45 mm). Among 70 AF patients indicated with anticoagulation, 53 patients (76%) received warfarin. During a follow-up of 5.5±2.0 years, the patients with AF had a higher incidence of all-cause death, cardiovascular death and strokes (11.7% vs 1.3%, 6.5% vs 0.9% and 19.5% vs 2.6%, respectively, all p<0.05) than those without AF. When adjusted by the age and gender, those with AF still had an increased risk for all-cause death (HR 6.58; 95% CI 1.65–26.16, p=0.007) and strokes (HR 5.13; 95% CI 1.85 to 14.18, p=0.002). AF was detected before the time of stroke in 8 (53%) out of 15 patients with both AF and stroke. In addition, six out of eight patients were on anticoagulation at the time of stroke. The cause of death was a stroke in three (33%) out of nine patients with AF.
Conclusion In patients with ApHCM, AF was common and was associated with a substantial risk for strokes and mortality suggesting that AF should be carefully managed in ApHCM.
- apical hypertrophic cardiomyopathy
- atrial fibrillation
- stroke
Statistics from Altmetric.com
Introduction
Apical hypertrophic cardiomyopathy (ApHCM) is a relatively rare type of hypertrophic cardiomyopathy (HCM), in which the hypertrophy predominantly affects the apex of the left ventricle (LV).1 In contrast to the other forms of HCM, ApHCM is considered as a ‘benign’ form of HCM, rarely associated with the occurrence of cardiovascular mortality and morbidity.1 2 However, more recent studies suggest that cardiovascular complications, such as myocardial infarctions and arrhythmias, are not uncommon even in ApHCM.3
Atrial fibrillation (AF) is the most common arrhythmia in HCM.4 5 Patients with HCM have a fourfold to sixfold greater likelihood of AF development compared with the general population.6 AF has been known to be associated with a high risk of strokes and systemic embolic events,7–9 and also with heart failure-related mortality.5 However, the incidence of AF and its impact on patients with ApHCM, who may have a different clinical course compared with the other types of HCM, have not been fully characterised, and there are divergent data.10 11 Therefore, this study was designed to assess the prognostic implications of AF and to identify the predictors of AF occurrence in an ApHCM cohort.
Methods
Study design and population
The study subjects were identified through a search of electrical medical record of Severance Hospital, Yonsei University College of Medicine, which serves as a large tertiary referral centre. The final study population was first selected retrospectively by searching patients with HCM or ApHCM from 2005 to 2009, and to confirm the diagnosis, the echocardiography was reviewed for each patient. In a total of 1226 patients who were diagnosed with HCM or ApHCM, 36.5% (447 patients) had apical type of HCM. Among those, patients were excluded if (1) the follow-up duration was less than a year (n=104) or (2) initial ECG at the time of diagnostic TTE was not available (n=37).
As a result, the occurrence of AF and the outcome in 306 consecutive patients with ApHCM were studied. The clinical records were collected for the demographic characteristics, coronary risk factors and symptoms including the New York Heart Association (NYHA) classification at the time of the diagnosis of ApHCM. In addition, the ECG and echocardiography results at the time of the diagnosis were also reviewed. The patients were divided into two groups, those with and without AF, according to the presence of ECG-documented AF at any time during the follow-up period. The Ethics Committee of our institution approved the study, and a written informed consent was waived by the Institutional Review Board.
Diagnosis
The diagnosis of ApHCM was made and then confirmed by reviewing the image of echocardiography at the time of diagnosis, when there was (1) the demonstration of asymmetric left ventricular hypertrophy (LVH) involving predominantly the LV apex in the absence of any clinical condition that may lead to LV hypertrophy, (2) apical wall thickness ≥15 mm in at least a single segment or a ratio of maximal apical to posterior wall thickness ≥1.3 at end-diastole and (3) hypertrophy without any predominant basal LV involvement.12–14 The types of ApHCM were also described as ‘pure’ in the case of isolated asymmetric apical hypertrophy and ‘mixed’ in the case of coexistent hypertrophy of the interventricular septum.12–14
Electrocardiography
The 12-lead ECG recorded closest to the echocardiographic examination was reviewed. The standard intervals and presence of LVH on the ECG were studied. The corrected QT interval was measured in lead V2.15 Documentation of AF was based on the ECG recordings obtained either after the acute onset of symptoms or fortuitously during routine medical examinations in the asymptomatic patients. AF was defined as paroxysmal or chronic according to the guidelines.16
Echocardiography
The left atrial (LA) dimension during end-systole and standard left ventricular dimensions during end-diastole and end-systole, as well as the LV wall thickness were obtained from two-dimensional images according to the standards of the American Society of Echocardiography.17 The maximal apical wall thickness was obtained from the standard apical four-chamber and two-chamber views during end-diastole. The LA volume index was measured using the prolate ellipsoid method.18 Pulsed-wave Doppler echocardiography of the mitral inflow and tissue Doppler imaging from the apical four-chamber view with 2–5 mm sample volumes placed at the septal corner of the mitral annulus were used to determine the peak velocity of the early diastolic filling (E), late filling (A), peak systolic velocity (S′) and early diastolic velocity (E′).19
Follow-up
The patients had an ECG follow-up every 3–6 months, and they were asked to visit the outpatient clinic at any time if they had any symptoms suspicious of having an arrhythmia, such as palpitations, chest discomfort or irregular heartbeats and were checked by a 12-lead ECG and 24 hours Holter monitoring. In the case of an AF occurrence, the patients were referred to electrophysiologists. The relevant clinical data and echocardiographic findings were also evaluated at regular visits.
The latest follow-up was obtained from the medical records. The mortality was classified as cardiovascular if it was attributable to myocardial infarctions according to the guideline, sudden cardiac death, arrhythmias (documented ventricular fibrillation or ventricular tachycardia with pulseless collapse), congestive heart failure (mortality during hospitalisation caused by heart failure) or strokes. Sudden cardiac death was defined as an unexpected and instantaneous death within 1 hour after a previously stable condition.
Statistical analyses
The continuous variables were tested for a normal distribution by the Kolmogorov-Smirnov test; continuous data are reported as the mean and SD. We compared the continuous variables using a Student’s t-test or Mann-Whitney U test between groups. The categorical variables were summarised as percentages and compared with the Fisher’s exact test or χ2 test as appropriate. The correlation analyses between normal and non-normal variables were tested using the Pearson’s and Spearman’s correlation coefficients, respectively. A logistic regression analysis was performed to estimate the predictors of AF. Cox regression analysis and Kaplan-Meier survival curve were used for survival analysis. A two-sided p value of <0.05 was considered significant, with CI of 95%. All statistical analyses were performed with SPSS V.23.
Results
Baseline characteristics
The study group consisted of 306 patients (207 males, mean age at the time of the diagnosis, 62±11 years) who were followed up for 5.5±2.2 years. Overall, AF was documented in 77 patients with a prevalence of 25.2%. Of the 77 patients with AF, 51 (66%) developed AF before the initial ApHCM diagnosis, including 36 in whom AF constituted the initial manifestation of ApHCM and led to the diagnosis. In contrast, 26 patients developed AF during the follow-up period (new-onset AF). The mean duration from the initial diagnosis of ApHCM to the occurrence of AF was 3.0±1.7 years (8 months to 7 years) with an annual incidence of 4.73%/year over a 5.5-year follow-up. At the final visit, the type of AF was paroxysmal in 25 (32.5%) patients, persistent in 1 patient and chronic in 51 (66.2%) patients.
The comparisons of the clinical characteristics at baseline between the patient with and without AF are presented in table 1. The patients with AF were older (68±11 vs 60±11 years, p<0.001), had more heart failure (48 vs 28%, p=0.002) and had a worse (NYHA class more than II) symptomatic status (46 vs 27%, p=0.002) than those without AF. Among those with AF, anticoagulation was used in 45 (58%) patients at the time of diagnosis of AF. Antiarrhythmic therapy and ablation therapy were performed in 28 (36%) and 8 (10%) patients, respectively. Three (3.9%) patients received permanent pacemaker implantation.
Baseline characteristics
The patients with AF had a noticeably larger LA dimension (46±7 vs 40±5 mm, p<0.001) and LA volume index (45.6±20.7 vs 30.1±8.9 mL/m2, p<0.001). There was no difference in any of the other findings between the two groups. None of the patients had an LV outflow obstruction. Mitral regurgitation more than moderate grade was detected in seven patients in AF group (9%, including one patient with severe mitral regurgitation) and in seven patients who remained NSR (3%).
Predictors of the development of AF
Table 2 shows the univariate and multivariable analyses for the development of AF. In the univariate analysis, the age, an NYHA class of more than two and a larger LA size were correlated with AF (all p<0.05). When adjusted for the age, gender and NYHA class at the time of the diagnosis in the multivariable analysis, the risk factors for AF were an advanced age (OR 1.07, 95% CI 1.04 to 1.11, p<0.001), NYHA class ≥2 (OR 1.92, 95% CI 1.09 to 3.39, p=0.023), larger LA dimension (OR 1.16, 95% CI 1.10 to 1.23, p<0.001) and the LA volume index (OR 1.10, 95% CI 1.07 to 1.14, p<0.001).
Univariate and multivariable analyses for correlates of atrial fibrillation (the age, gender and NYHA functional class at the time of the diagnosis were adjusted in the multivariable analysis)
To determine the risk factors for new-onset AF (n=26), we excluded patients who had AF before or concurrently with the diagnosis of ApHCM (n=51). In the multivariable analysis, only the LA size (OR 1.11, 95% CI 1.03 to 1.20, p=0.006) and the LA volume index (OR 1.07, 95% CI 1.03 to 1.11, p=0.001) size independently predicted the development of AF.
Impact of AF on the clinical course of ApHCM
The comparisons of the outcome between the patients with and without AF are presented in table 3. Overall, there were 12 deaths and 7 cardiovascular deaths (consisting of 4 patients with stroke, 2 sudden cardiac deaths and 1 arrhythmic death) during the follow-up period. The patients with AF had a higher incidence of both all-cause death (11.7% vs 1.3%, p<0.001) and cardiovascular death (6.5% vs 0.9%, p=0.012) than those without AF. The cause of death was a stroke in three (33.3%) out of nine patients with AF. AF was five times more common in patients with strokes than in those without (71.4% vs 21.8%, p<0.002). Of the 229 patients with ApHCM who remained in sinus rhythm, only 6 (2.6%) patients experienced strokes throughout the follow-up. However, 15 (19.5%) out of 77 patients with AF had strokes with an annual incidence of 2.7%.
The comparison of the outcomes between the patients with and without AF
Interestingly, AF was detected in seven patients after stroke. The duration between stroke and the detection of AF was within 30 days in four patients. However, the remaining three patients developed AF after 1.3 to 7.8 years of stroke (median 7.12 years).
The baseline characteristics of patients who were already diagnosed with AF before stroke (n=70) are presented in table 4. Stroke occurred in eight patients (%). Among them, six (75%) patients were on warfarin, and the remaining two patients were not on anticoagulation due to recent gastrointestinal bleeding event. In six patients with anticoagulation, three patients fulfilled the targeted international normalised ratio (INR) (2–3), while the INR of the remaining three patients were below the target range. All three patients briefly stopped warfarin before the development of stroke due to prolonged INR (>4).
Baseline characteristics of patients diagnosed with AF before the time of stroke (n=70)
Figure 1 shows the Kaplan-Meier survival curves for cardiac events according to the presence of AF. Patients with AF had a significantly lower cumulative survival-free rate of total deaths (p<0.001), cardiovascular death (p=0.003) and strokes (p<0.001) than those without AF. To find the impact of AF on all-cause death, cardiovascular death and strokes in patients with ApHCM, a Cox regression analysis was performed. When adjusted for the age and gender, the patients with AF had a significantly higher risk of all-cause death (HR 6.58; 95% CI 1.65 to 26.16, p=0.007) and strokes (HR 4.86; 95% CI 1.71 to 13.86, p=0.003), but not cardiovascular death (HR 5.02; 95% CI 0.88 to 28.53, p=0.07).

Kaplan-Meier survival curve of the overall survival (A), cardiovascular (CV) death-free survival (B) and stroke-free survival (C) according to atrial fibrillation (AF). Patients with AF had a significantly lower cumulative survival-free rate of total deaths (p<0.001), CV death (p=0.003) and strokes (p<0.001) than those without AF.
Finally, after excluding 51 patients who had AF before the diagnosis of ApHCM, patients with AF also had a lower cumulative survival-free rate of total deaths (p=0.002), cardiovascular death (p<0.001) and strokes (p<0.001) (figure 2).

Kaplan-Meier survival curve of the overall survival (A), cardiovascular (CV) death-free survival (B) and stroke-free survival (C) according to atrial fibrillation (AF) after excluding patients who had AF before the diagnosis of apical hypertrophic cardiomyopathy. Patients with AF also had a lower cumulative survival-free rate of total deaths (p=0.002), CV death (p<0.001) and strokes (p<0.001).
CHA2DS2-VASc score as a predictor of strokes in ApHCM
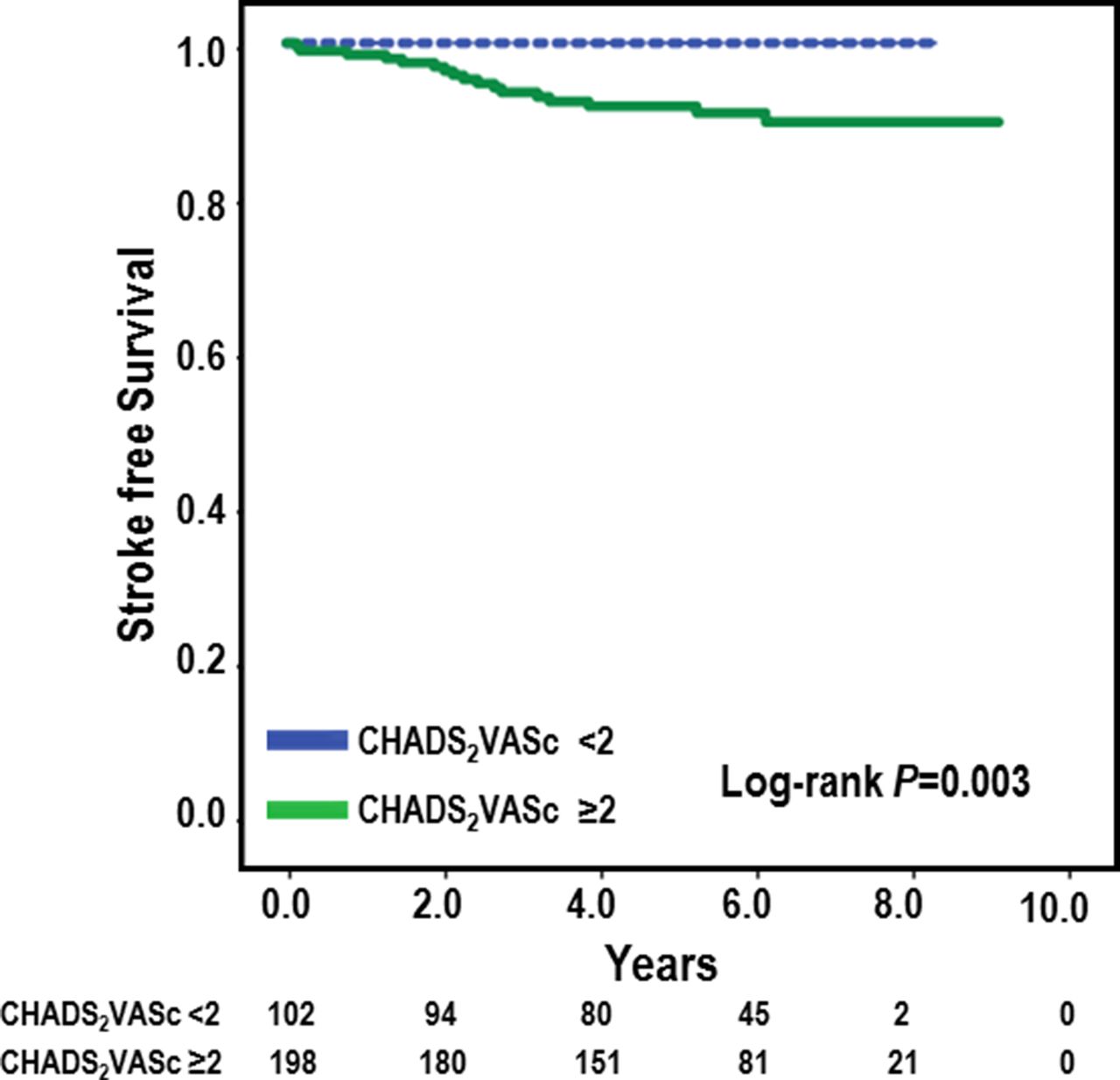
We also analysed the clinical utility of the CHA2DS2-VASc score system in settings of ApHCM. In the patients with AF, the mean CHA2DS2-VASc score was 4.5±1.1. Among the patients with AF, those who experienced strokes had a significantly higher CHA2DS2-VASc score compared with those who did not have a stroke (5.6±1.7 vs 3.0±17, p=0.002). All the patients with strokes (whether they had AF or not) had a CHA2DS2-VASc score higher than 2 (figure 3).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curve of stroke-free survival in overall patients with a high (≥2) CHA2DS2-VASc score than those with a low (<2) CHA2DS2-VASc score (p=0.003).
Discussion
Main findings
The main finding of this study was that AF was common with an annual incidence of 4.73% in patients with ApHCM. Second, the risk factors for AF were an advanced age, symptomatic heart failure and an enlarged LA. Finally, AF was associated with a substantial risk of stroke and cardiovascular mortality. This study clearly showed that the risk of stroke, cardiovascular mortality and even the all-cause mortality strikingly increased when patients with ApHCM develop AF. This finding suggests that a close follow-up and management of AF in patients with ApHCM are warranted.
AF in patients with ApHCM
The prevalence and annual incidence of AF in our study was 25.2% and 4.73%/year, respectively. These are comparable with a previous study reported by Olivotto et al 5 where the prevalence of AF in HCM was reported to be 22% with an annual incidence of 2%. However, their study included all types of HCM, and the proportion of each type was not specified. Eriksson et al 3 reported that the prevalence of AF was 12% during a mean follow-up of 13.6 years in patients with pure ApHCM. The high prevalence of AF in this study can be explained by the fact that the patients in the study by Eriksson et al 3 were much younger (mean age at the time of the diagnosis 46.1±15.1 years) than our patients. Also, half of the patients in our study had AF at the time of the diagnosis of ApHCM, and the symptoms of AF might have facilitated the diagnosis of AF in those patients. Consistently, the annual incidence in AF was comparable to other studies.
Predictors of AF in patients with ApHCM
Along with an advanced age, the most powerful predictor was the LA dimension. Mild LA enlargement (ie, 40–45 mm) is common in HCM due to an impaired diastolic function caused by thickened and noncompliant ventricular chambers.20 21 However, previous studies, where all types of HCM were enrolled, showed that an enlarged LA is not only the consequence of impaired diastolic function but also the strongest predictor of AF.5 22 LA enlargement is also known to be related to AF recurrence after radiofrequency ablation in non-valvular AF.23 Our study showed that the LA dimension can predict the development of AF in patients with ApHCM, a relatively rare form of HCM. This is in line with the Framingham Heart Study24 and the Cardiovascular Health Study,25 where the LA dimension had a prognostic significance in predicting AF in the general population.
Impact of AF on strokes and mortality in ApHCM
AF was a key determinant of strokes and cardiovascular mortality in this study. In over 5.5 years of follow-up, the patients with AF had a sixfold increase in the risk of ischaemic strokes compared with the patients who remained in sinus rhythm, and experienced far more cardiovascular death. This result is in line with a recent study where AF was a multivariable predictor of a decreased survival in patients with ApHCM.11 The development of AF may herald a clinical turning point, complicating or dominating the clinical course and long-term outcome.
Notably, among 15 patients with AF who experienced stroke, AF was detected after the stroke in seven patients and the duration between the diagnosis of AF and stroke was exceedingly longer in three patients—median 7.12 years. The fact that almost half of the patients who experienced stroke developed AF later in this study indicates that the prevalence of undetected AF maybe higher in patients with ApHCM. AF could be a coincidental finding in many patients, given their burden of underlying cardiovascular disease, which could independently cause ischaemic stroke and AF. Recent studies showed that atrial high-rate episodes detected by implantable devices, also called subclinical AF, are quite common in patients presenting with stroke.26 27 Although atrial high-rate episodes were associated with an elevated risk of AF, stroke and mortality in these studies,26 27 the prognostic and pathological significance of atrial high-rate episodes is still controversial.28 29 The high rate of patients diagnosed with AF after the stroke in this study may imply the need for more thorough surveillance for the development AF, at least in patients with ApHCM. Two large ongoing trials such as ARTESiA (Apixaban for the Reduction of Thrombo-Embolism in Patients With Device-Detected Sub-Clinical Atrial Fibrillation) and NOAH (non-vitamin K antagonist oral anticoagulants in patients with atrial high-rate episodes) will elucidate the clinical implication of subclinical AF and its relationship with stroke, and to guide appropriate management and monitoring strategies.28
Moreover, the fact that among eight patients who had AF at the time of stroke, six patients were already on oral anticoagulants with warfarin, and the INR values at the time were maintained in the target range also indicate that protection against strokes by oral anticoagulation was not absolute. This is in line with other clinical studies on AF in patients with structural heart disease,30 suggesting that the threshold for the initiation of anticoagulant therapy in ApHCM should be lower.
Limitations
First, as this is a retrospective study carried out at a single tertiary referral centre, inherent selection biases are inevitable. Moreover, ECG monitoring was done only during routine follow-up. Therefore, it is possible that a substantial burden of asymptomatic AF was not identified. Also, we cannot exclude the possibility that residual measured and/or unmeasured confounders may have influenced the results of this study. Finally, the number of deaths was relatively small, which limits to make a conclusion about the effect of AF in the mortality of patients with ApHCM.
Conclusion
AF is common in patients with ApHCM and has a powerful impact on the clinical course by increasing the risk of cardiovascular death and strokes. Therefore, patients with ApHCM require a longitudinal follow-up with careful monitoring for the development of AF, and a more aggressive therapeutic approach is warranted when AF develops.
Key messages
What is already known on this subject?
The clinical impact of atrial fibrillation (AF) in ApHCM is largely unknown. Therefore, we analysed whether AF has a prognostic implication in patients with ApHCM.
What might this study add?
AF occurred in 77 patients with ApHCM (25%; incidence, 4.6%/year) and was independently predicted by old age and a large left atrium (>45 mm).
Patients with AF had an increased risk for all-cause death (HR 6.58; 95% CI 1.65 to 26.16, p=0.007) and strokes (HR 5.13; 95% CI 1.85 to 14.18, p=0.002).
How might this impact on clinical practice?
AF was common in patients with ApHCM and was associated with a substantial risk for strokes and mortality, suggesting that the development of AF should be carefully monitored in ApHCM.
References
Footnotes
Contributors BJ and SEL designed and wrote the manuscript. JKP, JYK, HNP and MHL reviewed and gave the final consent to submit the manuscript.
Funding This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (NRF2012R1A2A2A02045367, 20100021993) and grants from the Korean Healthcare technology R&D project funded by the Ministry of Health & Welfare (HI12C1552, HI16C0058, HI15C1200).
Competing interests None declared.
Patient consent This is a retrospective study.
Ethics approval Yonsei University College of Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.