Article Text

Abstract
Objective Women with cardiac disease becoming pregnant have an increased risk of obstetric and fetal events. The aim of this study was to study the incidence of events, to validate the modified WHO (mWHO) risk classification and to search for event-specific predictors.
Methods The Registry Of Pregnancy And Cardiac disease is a worldwide ongoing prospective registry that has enrolled 2742 pregnancies in women with known cardiac disease (mainly congenital and valvular disease) before pregnancy, from January 2008 up to April 2014.
Results Mean age was 28.2±5.5 years, 45% were nulliparous and 33.3% came from emerging countries. Obstetric events occurred in 231 pregnancies (8.4%). Fetal events occurred in 651 pregnancies (23.7%). The mWHO classification performed poorly in predicting obstetric (c-statistic=0.601) and fetal events (c-statistic=0.561). In multivariable analysis, aortic valve disease was associated with pre-eclampsia (OR=2.6, 95%CI=1.3 to 5.5). Congenital heart disease (CHD) was associated with spontaneous preterm birth (OR=1.8, 95%CI=1.2 to 2.7). Complex CHD was associated with small-for-gestational-age neonates (OR=2.3, 95%CI=1.5 to 3.5). Multiple gestation was the strongest predictor of fetal events: fetal/neonatal death (OR=6.4, 95%CI=2.5 to 16), spontaneous preterm birth (OR=5.3, 95%CI=2.5 to 11) and small-for-gestational age (OR=5.0, 95%CI=2.5 to 9.8).
Conclusion The mWHO classification is not suitable for prediction of obstetric and fetal events in women with cardiac disease. Maternal complex CHD was independently associated with fetal growth restriction and aortic valve disease with pre-eclampsia, potentially offering an insight into the pathophysiology of these pregnancy complications. The increased rates of adverse obstetric and fetal outcomes in women with pre-existing heart disease should be highlighted during counselling.
- Congenital heart disease
- Valvular heart disease
- Pregnancy
- Prediction
Statistics from Altmetric.com
Introduction
The physiological changes that occur to ensure adequate blood perfusion of the uteroplacental circulation during pregnancy require significant cardiovascular adaptations. A normal heart has the reserve to adjust to these requirements, but the capacity of an already functionally compromised cardiovascular system is uncertain. Indeed, several studies have highlighted the risk of deterioration in cardiac function in pregnant women with heart disease and documented an increased risk of obstetric and fetal events.1 Cardiac events have been studied in depth and can be partly predicted by the modified WHO(mWHO) risk classification (c-statistic of 0.71).2 3 The mWHO stratifies patients mainly according to their cardiac diagnosis and on some clinical parameters such as ventricular function and New York Heart Association (NYHA) class. The expected risk of an adverse event is low compared with the normal population in mWHO class I, but the risk rises progressively with each class and women in mWHO class IV are at extremely high risk and should avoid pregnancy.
In women with congenital heart disease (CHD), increased adverse neonatal events have been reported, including preterm birth and low birth weight in particular.4 5 Genetic and epigenetic causes have been hypothesised to play a role in the pathophysiological mechanism of preterm birth6 and myocardial dysfunction and cyanosis were predictors of overall adverse neonatal outcome in women with CHD.4 Interestingly, previous studies found an association between cardiac function and abnormal uteroplacental blood flow, suggesting that pre-existing heart disease may cause abnormal placental development or perfusion.7 These data suggest that the mWHO classification may be able to predict obstetric and fetal risk in women with pre-existing heart disease. The aim of our study was to report the incidence of obstetric and fetal events in patients with cardiac disease, and to evaluate the discriminative power of the mWHO classification in predicting adverse obstetric or fetal outcome. In addition we will search for event-specific predictors.
Methods
The Registry Of Pregnancy And Cardiac disease (ROPAC) is a large, prospective and global registry. A detailed report of study design has been published previously.3 8 Patients in this interim analysis were included from January 2008 to April 2014. Patients in whom cardiac disease had been diagnosed during pregnancy were excluded. Patient informed consent was obtained when required by the local independent review board.
Data collection
Patient characteristics collected before pregnancy included age, diagnosis, ECG rhythm, risk factors (smoking, diabetes, hypertension), previous interventions, medication, parity, obstetric history and, if available, echocardiographic parameters. Follow-up was available for all patients up to 1 week after delivery. The originating countries were divided into developed and emerging countries according to the International Monetary Fund.9 Country of residence was included as an independent variable in further analysis (defined as ‘living in an emerging country’).
Every patient was stratified according to the mWHO classification, as stated in the latest guidelines by two authors (IMvH and JWR-H).10 mWHO class I implies no increased risk of events during pregnancy compared with the general pregnant population; class II has a small increased risk; class II-III a moderate increased risk; class III a significantly increased risk; class IV bears an unacceptable high risk of complications and consensus suggests that pregnancy should be avoided.
End points
Obstetric events were defined as maternal non-cardiac death up to 1 week postpartum, pregnancy induced hypertension (new-onset >140/90 mm Hg at two occasions), pre-eclampsia (including pre-eclampsia, eclampsia or HELLP syndrome) and haemorrhagic complication, which could be either postpartum haemorrhage (defined as increased blood loss, >500 mL after vaginal delivery or >1000 mL after caesarean delivery, up until 24 hours postpartum) or other major haemorrhage (defined as a bleeding resulting in at least 1 g/dL decrease in haemoglobin, the need for blood transfusion or end-organ damage such as haemorrhagic cerebrovascular accident or retinal bleeding). A fetal event was either premature birth <37 weeks, small-for-gestational-age (<10th centile), poor Apgar score (<7 at 1 min), fetal death ≥14 weeks of gestation or neonatal death up to 1 week after delivery. Induced and spontaneous preterm birth were also analysed separately.
A cardiac event was defined as a combined end point, including: cardiac arrest, cardiac death, new episode of arrhythmia requiring treatment, heart failure, thromboembolic event, aortic dissection, endocarditis, acute coronary syndrome, hospitalisation for cardiac reason or a cardiac intervention. Cardiac event rates are published elsewhere.3
Analysis
Categorical variables are presented as frequencies and percentages and differences between groups were assessed using χ2 tests. Continuous variables are presented as mean and SD, or as median and first and third quartiles as appropriate, and differences were assessed using Student’s t-test or Mann-Whitney U tests depending on the data distribution.
The mWHO classification was assessed for its ability to predict obstetric and fetal events in the total cohort, and also in patients with CHD and valvular heart disease separately. The discriminative power of the mWHO classification was checked by receiver operating characteristic (ROC) curves and c-statistics. A c-statistic of 0.5–0.7 represents low discriminative power; 0.7–0.9 represents moderate discriminative power; >0.9 represents a high discriminative power.11
In the total cohort, and in CHD and valvular heart disease separately, predictors of separate end points were searched for by univariable logistic regression analysis. Variables with a p value <0.10 were entered into multivariable logistic regression analysis, provided that there was no collinearity between independent variables. One independent variable could be entered per 10 events. Results are presented as OR, (95% CI) and p value. Multiple imputation was used to handle missing data within the following baseline variables: age, systemic ventricular dysfunction (ejection fraction <40%), hypoxia (<90%), parity, singleton or multiple pregnancy, atrial fibrillation, hypertension, diabetes mellitus, signs of heart failure, smoking and NYHA class. It was assumed to be plausible that all these variables were missing at random. The Bonferroni method was used to correct for multiple hypothesis testing in the multivariable analysis of the separate end points (corrected α=0.05/n, with n=number of hypotheses/end points tested). All analyses were performed with SPSS V. 21.0 (IBM, Armonk, New York, USA).
Results
This registry included 2966 pregnancies in women with structural cardiac disease from 99 centres in 39 countries, between January 2008 and April 2014. The cardiac diagnosis was known before conception in 2742 pregnancies, and these pregnancies were included in this analysis. Baseline characteristics are shown in table 1. CHD was present in 1599 (58.3%, table 2) women; valvular heart disease in 862 (31.4%, table 2); a cardiomyopathy in 161 (5.9%); ischaemic heart disease in 17 (0.6%); aortopathy in 95 (3.5%); and idiopathic pulmonary arterial hypertension in 8 (0.3%) women.
Baseline characteristics
Specific congenital and valvular heart diseases
Obstetric and fetal complications
Of the 2742 pregnancies, 231 (8.4%) pregnancies were complicated by one or more obstetric events, and one or more fetal events occurred in 651 (23.7%) pregnancies. Table 3 shows obstetric and fetal events in women with and without a cardiac event during pregnancy.
Obstetric and fetal events in women with and without a cardiac event
Maternal non-cardiac mortality
Non-cardiac maternal mortality occurred in two patients (0.07%). One patient with rheumatic aortic and mitral valve disease and elevated pulmonary arterial pressures was delivered by caesarean section at 35+3 weeks because of fetal distress. The neonate died shortly after delivery. Frank pus was found in the uterus, and the mother died of septic shock 2 days later. The second patient had idiopathic pulmonary arterial hypertension. She was treated with heparin in the first trimester and with warfarin during the second and third trimesters before she was switched back to unfractionated heparin before term. An elective caesarean section was performed at 38+0 weeks. During delivery, she developed shock due to an acute pulmonary embolism and the patient died shortly after delivery. The neonate survived and was healthy.
mWHO classification
Figure 1 shows the adverse obstetric and fetal events that occurred in each mWHO-class. The c-statistic for the mWHO-classification was 0.601 (95% CI 0.563 to 0.639) for obstetric events and 0.561 (95% CI 0.536 to 0.586) for fetal events, which means a low discriminative power. The ROC curves are presented in figure 2. The ROC curves of the mWHO classification for prediction of obstetric and fetal events in patients with CHD and valvular heart disease separately all show a poor discriminative power (see online supplementary figure 1). The mWHO classification did not perform better in emerging or advanced countries.

Obstetric and fetal events per mWHO class. mWHO, modified WHO.

ROCs mWHO classification. Obstetric events c-statistic 0.601, 95% CI 0.561 to 0.639. Fetal events c-statistic 0.561, 95% CI 0.536 to 0.586. ROC, receiver operating characteristic; mWHO, modified WHO.
Predictors of separate events
The frequencies of separate events within each diagnostic group and in relation to baseline characteristics are shown in online supplementary table 1. The results of the univariable and multivariable analyses are shown in online supplementary tables 2 and 3, for all patients in this cohort, and for patients with CHD and valvular heart disease separately. C-statistics for the new models are shown in online supplementary table 3. Indeed, part of the models showed a better discriminative power for predicting the separate end points, than the mWHO classification (and the new models) predicted combined end points.
The results for pre-eclampsia, fetal/neonatal death, spontaneous preterm birth and small-for-gestational-age are depicted in figure 3. The main findings of the multivariable analysis in patients with CHD and valvular heart disease are presented in figure 4 and figure 5.

Predictors of obstetric and fetal events. NYHA, New York Heart Association.
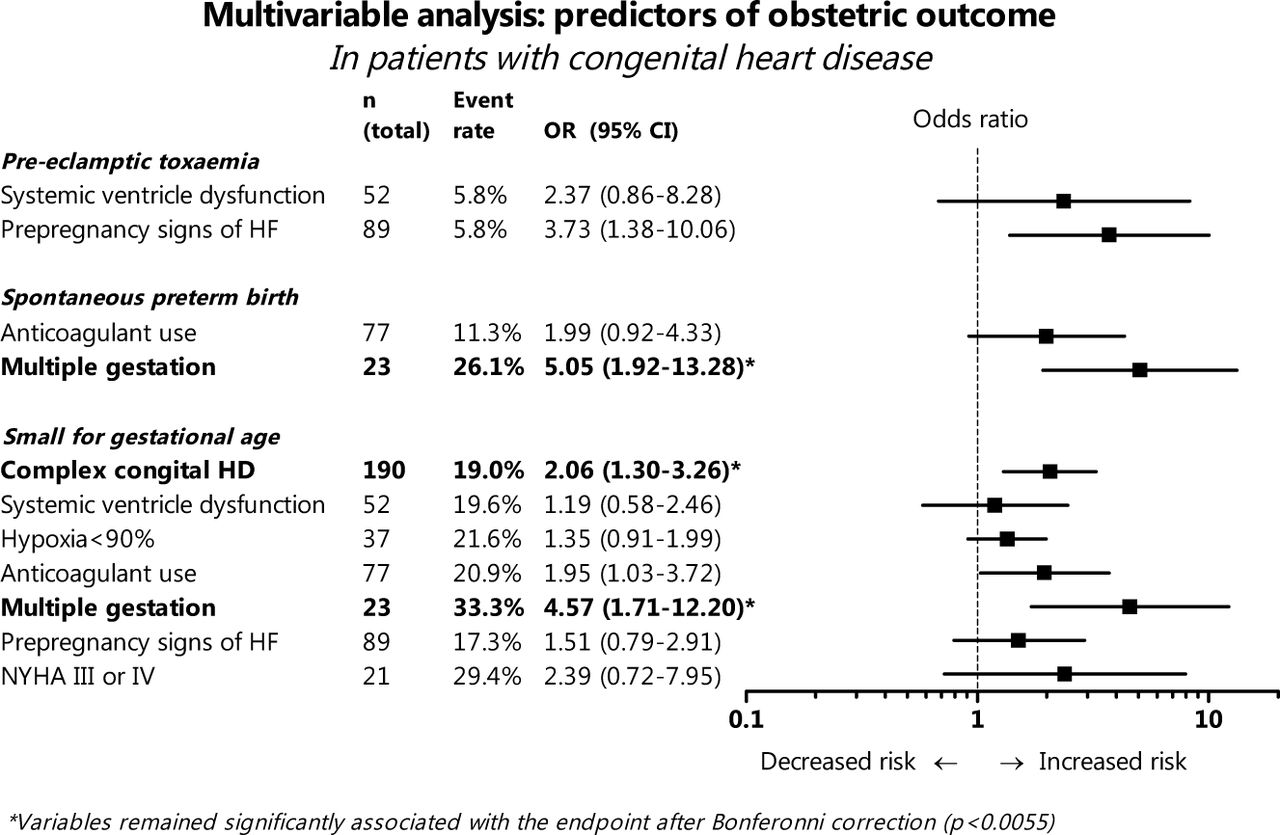
Predictors of obstetric events in patients with congenital heart disease. NYHA, New York Heart Association.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Predictors of obstetric events in patients with valvular heart disease.
Discussion
This is the largest prospective cohort of pregnant women with known structural heart disease to date, reporting an obstetric event rate of 8.4% and fetal event rate of 23.7%. The mWHO classification failed to accurately predict these events, although a gradual increase of events can be observed throughout the mWHO classes. As in the general population, twin pregnancy and pregestational diabetes are important predictors of adverse fetal outcome. Pre-eclampsia is more often seen in women with aortic valve disease, while spontaneous preterm birth is more common in patients with CHD and small-for-gestational-age neonates, in particular in complex CHD. Women who suffer from a cardiac event during pregnancy are at increased risk of most obstetric and fetal complications. These findings may help to accurately inform women about the risks of obstetric and fetal problems when they contemplate pregnancy.
mWHO risk classification
The obstetric and fetal event rates are in line with findings of a previous prospective study in patients with any type of cardiac disease.12 Based on the gradual increase of event rate in each mWHO class, there seemed to be a relationship between the mWHO classification and fetal and obstetric outcomes, as was also shown in a previous publication.8 The high incidence of obstetric events in mWHO class III is mainly due to haemorrhagic complications in women with a mechanical valve who are treated with anticoagulants.13 Unfortunately, overall, the mWHO classification failed to show a sufficient discriminative power. This agrees with the results of a previous validation study in patients with CHD.14 Several explanations may explain the poor predictive power of the mWHO classification. First, it seems that a cardiac diagnosis as a risk factor is subordinate to the well established risk factors for obstetric and fetal events in the general population, such as maternal age, multiple pregnancy and nulliparity. The majority of the obstetric and fetal events are associated with these known risk factors, which may have a bigger impact in women with heart disease. This is supported by the high rate of events present in mWHO class I women. Second, the combined end point may be too inclusive and unsuitable for designing an accurate prediction tool, which is also clear from the fact that the new models do not perform well either for combined end points while they do for several separate outcomes (all presented in the online supplementary data). For instance, haemorrhage will usually have a different aetiology than pre-eclampsia. In addition, fetal complications can be either the result of primary maternal, fetal or both maternal and fetal deteriorating conditions. Combining events may obscure the actual link between heart disease and specific pregnancy related events.
Obstetric complications
Pre-eclampsia was more common in women with aortic valve disease and, as expected, in nulliparous women and those with pre-existing hypertension. Also, ventricular dysfunction was a significant predictor of pre-eclampsia in the univariable analysis, but none of these predictors were significant (after correction for multiple hypotheses testing) in the multivariable analysis. Subclinical ventricular dysfunction is often seen in patients with aortic valve disease, typically in stenotic lesions.15 However, pre-eclampsia, in particular early pre-eclampsia, is known to be associated with subclinical cardiac dysfunction, although the cardiac dysfunction is probably secondary to pre-eclampsia.16 Previous studies have reported poor placental function in association with subclinical ventricular dysfunction.7 Thus, the link between aortic valve disease and pre-eclampsia warrants further investigation, as the association may provide a valuable insight into the aetiology of pre-eclampsia and these women may benefit from prophylactic medication such as aspirin.17
Haemorrhage occurred more often in women with a mechanical valve13 and is mainly associated with anticoagulation. Another independent predictor specifically of postpartum haemorrhage in the subanalysis of patients with CHD, was complex disease, which has been described earlier.5 Anaemia, independent of antepartum haemorrhage, is a known predictor of postpartum haemorrhage18 and is also often encountered outside pregnancy in patients with complex CHD,19 offering another explanation for the predisposition to postpartum haemorrhage. It is unknown whether uterine atony, strongly associated with postpartum haemorrhage, is more prevalent in patients with complex CHD, still the more prudent use of oxytocin in the third stage and a low threshold to assisted deliveries in this group may contribute to the risk.20
Fetal/neonatal complications
The strongest predictor of fetal and neonatal complications in our cohort was multiple pregnancy, being an important predictor of fetal demise, and of preterm birth and small-for-gestational-age. In the general population, fetal/perinatal death is reported in about 0.8%–1.2% and increases about four to five times in twin pregnancies.21 In ROPAC fetal/neonatal death occurred in 0.8% of singletons and 10.9% of twins, which is an increase of 13.6. Preterm birth occurs in almost half of the twin pregnancies in the general population, which is at least seven times more often than reported in singleton pregnancies.21 In the current series, preterm delivery occurred in 37% of ROPAC twin and 12% of singleton pregnancies. So preterm birth is not more common in twins, in contrast to singletons. But more importantly, it seems that cardiac disease further increased the risk of fetal demise. This may be related to the higher incidence of small-for-gestational-age babies in ROPAC twins: 34% had a birth weight beneath the 10th centile, compared with 10% of singleton pregnancies. As an illustration, in the general population this rate only increases from about 10%–11% to 15%.22 23
An obstetric complication occurred in more than 58% of multiple pregnancies (all twin), which is not surprising based on the evidence,12 24 but it raises the question how to deal with twin pregnancy in women with a severe form of heart disease. Women should certainly be counselled about the risks. Twins should be avoided by performing single embryo transfer in case of in vitro fertilisation, and by carefully monitoring ovulation induction. However, it is not possible to prevent the spontaneous conception of twins. To our opinion, reduction or termination of pregnancy should be reserved for strict maternal reasons or social indications. We do not know whether the rate of pregnancy complications is much higher in multiple pregnancies in women with heart disease compared with multiple pregnancies in the general population, and future research is needed to study this.
Premature deliveries are either spontaneous or iatrogenic. Symptomatic women (NYHA class III-IV), and women taking oral anticoagulants, were more likely to have an induced preterm delivery, which is consistent with recommendations made by the guidelines.10 Interestingly, women with CHD tended to go into spontaneous preterm labour. Both inflammatory processes, and uteroplacental ischaemia can initiate preterm labour.25 26 The (subclinical) failure of the heart to fully adapt to pregnancy in CHD may promote inflammation and in more severe cases lead to uteroplacental hypoperfusion and ischemia. Certainly, maternal hypoxia increases cytokines and oxygen free radicals, which may cause abnormal placentation.27 Indeed, uteroplacental flow has been shown to be abnormal in women with CHD.28
Small-for-gestational-age babies were mainly seen in women with complex CHD and in symptomatic patients (NYHA class III-IV). Maternal hypoxia was only found to be a predictor in univariable analysis, but its effect may have been influenced by the coexistence of complex CHD. Women with CHD and those with ventricular dysfunction should be very closely monitored with regard to fetal growth; preventative treatment like aspirin may need further investigation in this patient group.29 It is expected to be of less benefit if these women indeed rather suffer from low cardiac output as a cause of growth restriction, instead of insufficient deep placentation due to ischaemia.
Intrauterine death is associated with oral anticoagulant use as has been reported in a previous ROPAC study, describing pregnancy in women with a mechanical valve.13 Oral anticoagulant use in the first trimester predisposed women to an increased risk of fetal death in both the second and third trimesters. Miscarriages in the first trimester were excluded from this analysis, but have been reported in several groups of heart disease to be up to 40% in women with a Fontan circulation.5 Certainly, this excessive rate should be mentioned to women with complex disease.
Emerging countries
In this cohort, 33% of women came from a country with an emerging economy. In these women, fetal loss was more common, which is in line with previous studies of global pregnancy outcome and is partly explained by the limited access to obstetric and neonatal care, increased rates of prolonged pregnancies and infectious disease.30
In emerging countries, both induced and spontaneous preterm birth were less common than in developed countries. This is interesting as generally, spontaneous preterm birth is thought to be more common in low-income countries.31 Specialists in developed countries may be more likely to induce preterm birth as soon as the maternal condition deteriorates and women from these countries may have better and quicker access to obstetric care facilities. Also, a higher prevalence of spontaneous preterm birth was related to advanced age in a large global cohort,32 which may be the result of uterine dysfunction.33 However, in our study, age was not related to spontaneous preterm birth.
Differences between emerging and developed countries in maternal and fetal outcome in women with cardiac disease are intriguing and deserve attention in future research.
Limitations
Data were missing in no more than 5% of pregnancies, except for smoking (14% missing), systemic ventricular function (37.4% missing) and hypoxia (59.7% missing). These questions were added in the adjusted online case report form in 2012, and data are therefore missing at random. In previous studies, systemic ventricular function and hypoxia were suggested as potential important predictors4 and therefore we decided to include this predictor in the analysis. Missing variables were handled using multiple imputation, which is considered a reliable tool in such situations where large amounts of data are missing. However, firm conclusions cannot be drawn.
Miscarriage before 14 weeks was excluded from the analysis. The incidence of miscarriage widely ranges in literature concerning the overall healthy population. It is strongly influenced by inclusion bias and therefore hard to interpret. That is why, in line with previous literature, we chose not to include miscarriage in the first trimester as an end point.
Being aware of its inferiority, we analysed Apgar score at 1 min rather than at 5 min, because the first value was complete in almost all cases, while Apgar at 5 min was missing in more than half.
Conclusion
Women with cardiac disease are at high risk of adverse obstetric and fetal events. The mWHO classification conducted for women with structural heart disease is a good predictor for maternal outcome, but does not perform as well for obstetric and fetal events. The majority of events are associated with more general predictors such as twin pregnancy. Other associations were complex CHD leading to small-for-gestational-age babies, aortic valve disease predisposing to pre-eclampsia and the use of anticoagulants leading to fetal demise. Whether factors like twin pregnancy lead to a greater obstetric and fetal risk in women with heart disease than their healthy peers needs to be determined and may influence the counselling of these patients.
Key messages
What is already known on this subject?
In women with heart disease, increased adverse neonatal events have been reported, including preterm birth and low birth weight in particular. Interestingly, previous studies found an association between cardiac function and abnormal uteroplacental blood flow, suggesting that pre-existing heart disease may cause abnormal placental development or perfusion. These data suggest that the modified WHO classification, which stratifies patients according to their cardiac diagnosis and on some clinical parameters, may be able to predict obstetric and fetal risk in women with pre-existing heart disease.
What might this study add?
This study shows that the modified WHO classification does not perform well for prediction of obstetric and fetal events, with a c-statistic of 0.60 for obstetric events, and of 0.56 for fetal events. The majority of events in this cohort are associated with more general predictors such as twin pregnancy, nulliparity and prepregnancy hypertension. Other associations were complex congenital heart disease leading to small-for-gestational-age babies, aortic valve disease predisposing to pre-eclampsia and the use of anticoagulants leading to fetal demise.
How might this impact on clinical practice?
These findings may help to accurately inform women about the risks of obstetric and fetal problems when they contemplate pregnancy. Whether factors like twin pregnancy lead to a greater obstetric and fetal risk in women with heart disease than their healthy peers is to be determined and may influence the counselling of these patients.
References
Footnotes
Acknowledgements The authors thank all ROPAC investigators, who are listed in the online supplement. The authors also thank the EORP team for their contribution, in particular: Elin Folkesson Lefrancq (project officer) and Viviane Missiamenou (data manager).
Contributors JWR-H and RH were responsible for planning, study design, data collection, drafting the manuscript and critical revision of the manuscript.
IMvH, VD, CL, MM, DJM, LG, NMB, JC and MRJ contributed to data collection, drafting the manuscript and critical revision of the manuscript.
Funding Since the start of EORP, the following companies have supported the programme: Abbott Vascular Int. (2011-2014), Amgen Cardiovascular (2009-2018), AstraZeneca (2014-2017), Bayer (2009-2018), Boehringer Ingelheim (2009-2016), Boston Scientific (2009-2012), The Bristol Myers Squibb and Pfizer Alliance (2011-2016), The Alliance Daiichi Sankyo Europe GmbH and Eli Lilly and Company (2011-2017), Edwards (2016-2019), Gedeon Richter Plc. (2014-2017), Menarini Int. Op. (2009-2012), MSD-Merck & Co. (2011-2014), Novartis Pharma AG (2014-2017), ResMed (2014-2016), Sanofi (2009-2011), SERVIER (2010-2018). The companies that support EORP were not involved in any part of the study or this report.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Local IRBs.
Provenance and peer review Not commissioned; externally peer reviewed.