Article Text

Abstract
Background Transcatheter aortic valve implantation (TAVI), widely used to treat high-risk patients with severe symptomatic aortic stenosis, has recently been extended to younger patients at lower operative risk in whom long-term durability of TAVI devices is an important concern. Therefore, we conducted a systematic review and meta-analysis of observational studies addressing the frequency of structural valve deterioration (SVD) after TAVI.
Methods We searched Medline, Embase, Cochrane Database of Systematic Reviews, and Cochrane CENTRAL from 2002 to September 2016. We included observational studies following patients with TAVI for at least 2 years. Independently and in duplicate, we evaluated study eligibility, extracted data, and assessed risk of bias for SVD post-TAVI. Our review used the GRADE system to assess quality of evidence. We pooled incidence rates using a random effects model.
Results Thirteen studies including 8914 patients, with a median follow-up between 1.6 and 5 years, reported an incidence of SVD post-TAVI between 0 to 1.34 per 100 patient years. The pooled incidence of SVD was 28.08 per 10 000 patients/year (95% CI 2.46 to 73.44 per 100 patient years). Of those who developed SVD, 12% underwent valve re-intervention. Confidence in the evidence was moderate due to inconsistency among studies.
Conclusion Structural valve deterioration is probably an infrequent event within the first 5 years after TAVI. Ascertaining the impact of SVD and the need for valve-related re-interventions to inform recommendations for patients with a longer life-expectancy will require studies including a large number of patients with longer follow-up (>10 years).
- aortic stenosis
- systematic review
- meta-analysis
- transcatheter valve interventions
Statistics from Altmetric.com
INTRODUCTION
Although the durability of surgical aortic valve replacement (SAVR) with mechanical prostheses justifies their use in young adults, most older adults now receive bioprosthetic valves. Transcatheter aortic valve implantation (TAVI) provides a preferred alternative to SAVR for patients with a high or prohibitive surgical risk and for some low- and intermediate-risk patients.1 2 A systematic review that informed a rapid recommendation2 3 found that transfemoral TAVI, in comparison to SAVR, results in lower mortality and acute kidney injury at 2 years, and may reduce stroke rates4. Patients must, however, trade off these benefits of TAVI against the uncertain durability of TAVI valves beyond 2 years that contrasts with the known durability of SAVR bioprosthetic valves.2
For very old patients (eg, over 85), TAVI durability is not a major issue because their lifespan is limited irrespective of their valvular disease. TAVI durability becomes important in those with longer expected longevity; in such individuals, the risk of structural valve degeneration (SVD) over the longer term may offset the short-term advantages of TAVI. Therefore, we conducted a systematic review and meta-analysis addressing the frequency of SVD after TAVI.
METHODS
Data sources and searches
We developed our search strategy by modifying a previously published comprehensive systematic search.5 We searched in Medline, Embase, PubMed (non-Medline records only), Cochrane Database of Systematic Reviews, and Cochrane CENTRAL from conception to 5 September 2016. Appendix A presents the search strategy. We searched reference lists of included publications and previously published narrative reviews to identify additional references. Our review included additional studies published after the systematic search through suggestions from experts.
Study selection
Eligible studies, in any language, followed adult (≥18 years) patients with severe symptomatic aortic stenosis undergoing their first TAVI and reported on SVD. Our review included both prospective and retrospective studies published after 2006 (to capture contemporary valve technology). When more than one study reported on the same population and outcome, we used the study with the larger sample size. Two reviewers working in pairs independently screened titles and abstracts and, for potentially eligible studies, determined eligibility from full text articles. We conducted all screening using the Covidence systematic review software.6
We used—whenever authors reported—structural valve-related degeneration according to the Valve Academic Research Consortium-2 (VARC) definition7: the need for any repeat procedure (balloon-aortic valvuloplasty, TAVI or SAVR); increased mean aortic valve gradient >20 mm Hg, effective orifice area (EOA) <0.9–1.1 cm2 and/or Doppler velocity index (DVI) <0.35 m/s; or moderate or severe prosthetic valve regurgitation.7 When studies did not use the VARC definition but reported the proportion of patients with different ranges of mean aortic valve gradient, we considered any patient with a mean aortic valve gradient >20 mm Hg to have SVD.
Data abstraction and risk of bias assessment
Two reviewers working in duplicate used standardised forms to independently extract the following data: source; time frame of recruitment; number of events; definition of SVD; and population characteristics, including age, sex, history of coronary artery disease (CAD), chronic obstructive pulmonary disease (COPD), diabetes, hypertension, atrial fibrillation (AF), left ventricular ejection fraction (LVEF), New York Heart Association (NYHA) classification, prior coronary artery bypass grafting (CABG), prior myocardial infarction (MI), and logistic European System for Cardiac Operative Risk Evaluation (EuroSCORE).
The Quality in Prognostic Studies (QUIPS) tool, that includes criteria of patient selection, study attrition, prognostic factor measurement, outcome measurement, study confounding, and statistical analysis and reporting, provided an instrument for assessing risk of bias in individual studies.8 We used the individual criteria, rated as low, moderate, or high risk of bias, to inform the overall risk of bias in each study: five or six low-risk domains as overall low risk of bias, two or more high-risk domains as overall high risk of bias, and remaining studies as overall moderate risk of bias. To assess quality of evidence, this review used the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system for prognostic questions in which observational studies start as high quality of evidence but can be rated down for risk of bias, imprecision, inconsistency, indirectness, or publication bias.9 We checked for publication bias through visual assessment of funnel plots.
Data synthesis and statistical analysis
Using the number of events, sample size, and median follow-up time of each cohort, we calculated the incidence rate per 10 000 patient years for each study. When the median follow-up was not reported, we used an established algorithm to estimate individual patient data for survival analysis (see online supplementary material).10 Using this algorithm, we determined an estimate for the median length of follow-up. STATA’s (version 13.1) Metaprop’s DerSimonian and Laird random effects model, with a Freeman-Tukey transformation,11 provided the software to combine and present the study results using a two-sided p value of 0.05 as a threshold for statistical significance.
Our review assessed heterogeneity through visual inspection of point estimates and confidence intervals. We did not use I2 statistics to evaluate heterogeneity because, in prognostic studies with large sample sizes that result in precise estimates, I2 is typically very large even in the face of modest or even minimal inconsistency.9
To identify sources of heterogeneity, we performed post-hoc subgroup analyses to compare balloon-expandable and self-expandable TAVI, use versus non-use of VARC-2 for defining SVD, median follow-up greater than or less than 4 years, and reports of use of anticoagulation therapy. For assessing the association between valve type and incidence of SVD, we considered the proportion of patients on a self-expandable valve as a continuous variable. For the other independent variables, when studies had a mix of device types and a mixed portion of patients on anticoagulation therapy, we classified studies according to the dominant group (>60%). We conducted subgroup analyses using R (version 3.3.2) random effects univariable meta-regression with a Freeman-Tukey transformation. When we observed a significant association, we conducted a multivariate meta-regression (adjusted for the univariable significant interactions) to test for independence of the subgroup effect.
RESULTS
Study selection and characteristics
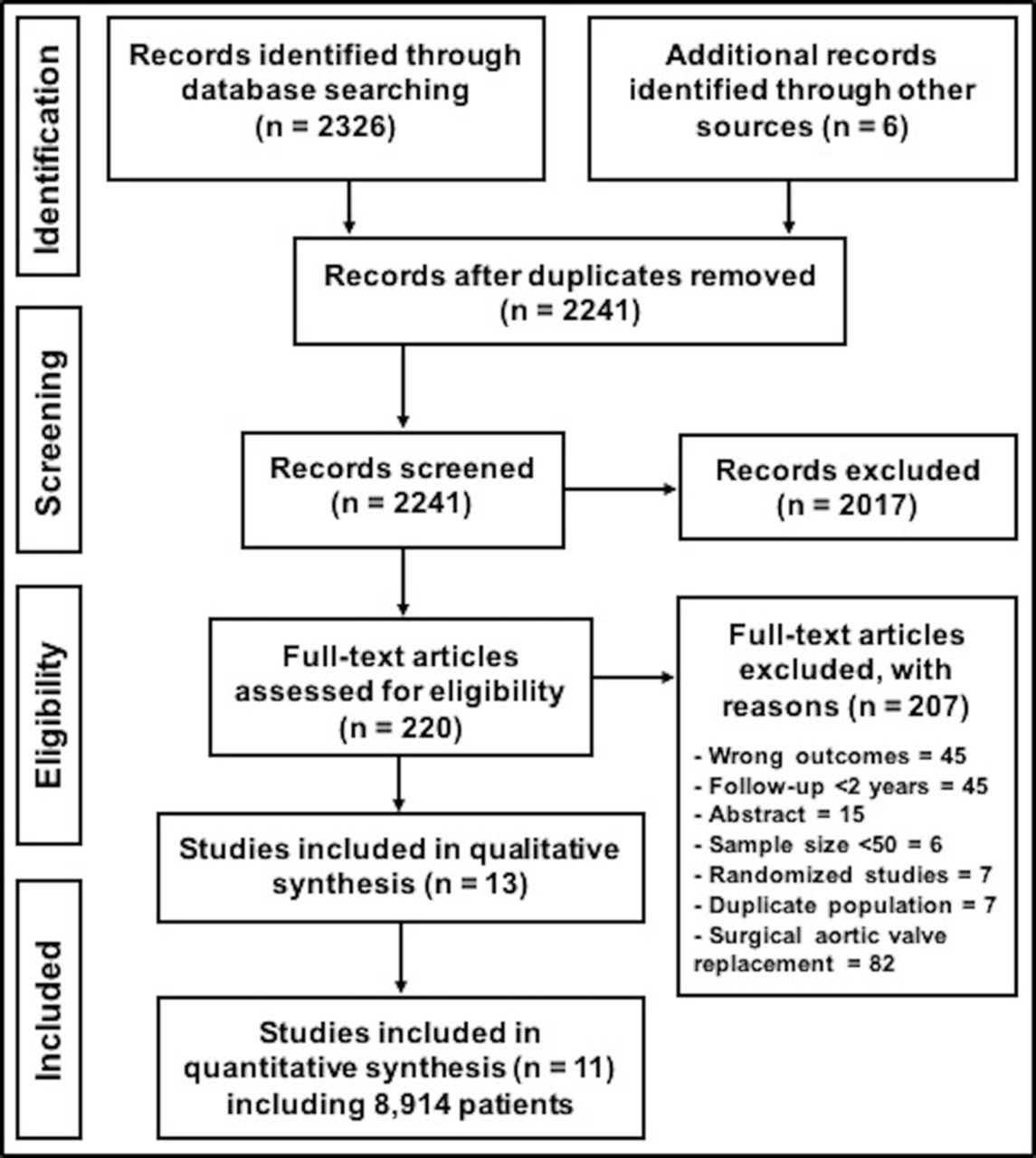
Figure 1 presents the study flow diagram following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) format.12 The 13 eligible studies13–25 reported on 8914 patients enrolled between 2004–2015. Studies reported an approximately equal distribution of male and female patients with severe aortic stenosis undergoing TAVI with mean age ranging from 79 to 83 years (see online supplementary material).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Risk of bias in individual studies
All but one of the included studies proved overall low risk of bias (supplementary material).13–23 25 We found one study to be at moderate risk of bias due to moderate risk of bias under study attrition and outcome ascertainment.24
Structural valve deterioration
Thirteen studies reported the absolute number of patients suffering SVD that ranged from 0 to 47 (frequency of 0% to 5.6%) over median follow-up times ranging from 1.6 to 5.0 years (table 1). Seven studies19–22 24–26 reported no cases of SVD; the six studies13–15 17 18 27 with SVD cases reported SVD in 3.1% to 5.6% of their population. The incidence rate ranged between 0 and 134 per 10 000 patient years.
Baseline demographic and population characteristics
The pooled estimate of SVD incidence rate was 28.08 per 10 000 patient years (95% CI 2.46 to 73.44, moderate quality evidence, rated down for inconsistency) (table 2, figure 2). Results were consistent in three studies with non-VARC-2 definitions for SVD compared to eight studies that used VARC-2 (supplementary material), and seven studies with median length of follow-up ≥4 years versus four studies with <4 years (supplementary material). An increasing proportion of patients on self-expandable valves showed an association with an increasing incidence of SVD (7.6 more cases of SVD per 10 000 more patients on self-expandable valves, 95% CI 0.4 to 14.8; p=0.039) (supplemental material 4). Two studies that reported no anticoagulation therapy at discharge in the majority of patients showed a higher incidence rate of SVD (126.50 per 10 000 patient years, 95% CI 96.74 to 160.09) compared with studies that did not report on the use of anticoagulation (13.51 per 10 000 patient years, 95% CI 0.16 to 39.85) (association p=0.01; figure 3). In a multivariable meta-regression including the aforementioned significant predictors, only the proportion of patients on self-expandable valves showed an independent association with an incidence of SVD (6.4 more cases of SVD per 10 000 more patients on self-expandable valves, 95% CI 0.4 to 12.4; p=0.0366).

Overall pooled estimate of structural valve deterioration incidence rate.

{kind=link}
{kind=link}
{kind=link}
Subgroup analysis on use of anticoagulation.
Quality of evidence
Five studies (33 events) reported on the cause of SVD, and commonly found valve restenosis (19 events, 58%), followed by regurgitation (13 events, 39%) and mixed (one event, 3%). Seven studies reporting 25 events observed three (12%) patients to require valve re-intervention with transcatheter aortic valve-in-valve implantation. Of these, two patients experienced severe symptomatic restenosis14 and one patient experienced aortic regurgitation.18
Publication bias
Visual inspection of the funnel plot showed no relationship between incidence rates and study standard error (supplementary material).
DISCUSSION
We found that few patients experienced SVD during the 5-year period after TAVI; indeed, the majority of studies reported no SVD at all. The pooled incidence rate was 28 per 10 000 patient years; in those that did experience SVD, 12% underwent valve re-intervention. We rated the quality of evidence as moderate due to inconsistency (one study reported an incidence of SVD of 134 per 10 000 patient-years, which if true would mean a rate close to 7% at 5 years).
Strengths
We defined explicit eligibility criteria, conducted a comprehensive search, reviewed eligibility and risk of bias of individual studies in duplicate using an established rating system, and pooled results to generate a risk of SVD per 100 patient years. A final strength is that we applied the GRADE approach to rate overall quality of evidence9 which, for SVD, proved moderate due to inconsistency (table 2).
Limitations
A major limitation of our review is the limited follow-up duration of all included studies. Moreover, only a small number of patients reached the longest median follow-up time of 5 years. Patient-level data were unavailable for this analysis, precluding a more robust analysis for any differences in baseline clinical and periprocedural data that may have affected the outcome.
Our analysis assumes a constant rate of SVD over time, an assumption that, although it is possibly true over 5 years, is unlikely to be true over longer periods of time. In SAVR, rates of deterioration increase substantially at 10 years, and even more at 15 years.28 A pattern of increased hazard of SVD over time is likely to also occur with TAVI.
Investigators based the diagnosis of SVD largely on increased mean trans-prosthetic gradient (suggesting valve restenosis), with only 12% of patients requiring valve re-intervention for TAV failure. Some patients may, however, not have undergone valve re-intervention because they were too frail, or had died before the intervention was possible. Others may have had functional limitations with dyspnoea or fatigue and still not have undergone valve re-intervention. Thus, the proportion of patients with SVD who suffered important adverse consequences remains uncertain.
All studies used Doppler echocardiography to define SVD. Not all studies, however, used the VARC-2 definitions7 and there was inconsistency not only in thresholds for defining SVD but also in the timeframe between the TAVI procedure and echocardiographic assessments.
Our review suggests that patients treated with the self-expanding versus balloon-expanding TAVI may potentially experience a higher incidence of SVD. Multivariate meta-regression showed this to be an independent association. This subgroup hypothesis has, however, only low credibility.29 It is based on a between-study comparison, the hypothesis was post-hoc, and the effect was not consistent across all studies in the subgroup of self-expandable valves. Finally, the biological rationale is at best questionable. Prior findings have suggested that balloon valve deployment results in a traumatic effect on the implant leaflets,30 an event that does not occur with self-expanding valves. However, the potential structural damage on crimped leaflets30 and its impact on valve durability is speculative.
Our review also raises the possibility that the lack of long-term anticoagulation may have increased the apparent incidence of SVD. One might postulate a biologic rationale for the effect; a lack of anticoagulation might increase the risk of thrombus reducing TAV-leaflet motion due to leaflet thickening, causing an increase in trans-prosthetic gradient, and thus overestimate the true incidence of SVD.31–33 This hypothesis is consistent with previous reports17 32 33; nevertheless, this postulated effect is again of low credibility. The subgroup analysis is based on a between-study comparison in which only two studies14 17 reported on anticoagulation status at hospital discharge; the frequency of anticoagulation in the other nine studies remains uncertain. The subgroup hypothesis was generated post-hoc, the direction of effect specified post-hoc, the effect was not independent in multivariable meta-regression, and results varied widely in the subgroup of studies not reporting on anticoagulation status.
Previous literature reported a 23 mm TAV valve-in-valve procedure, and greater body mass index (BMI) as risk factors for higher rates of SVD after TAVI.17 The smaller TAV size and high BMI increase the likelihood for prosthesis-patient mismatch, a well-recognised predictor for SVD after SAVR,34 35 and are also associated with poor outcomes in high-risk patients undergoing TAVI.36 Limitations in reporting of population characteristics prevented us from exploring these subgroup hypotheses.
Comparison with other studies
Unpublished data not eligible for inclusion in our study, presented by Dvir and colleagues,37 reported 35 out of 378 patients (9.26%) developed SVD during a median follow-up of 51 months following TAVI (IQR 22–75 months). This greater incidence of SVD is likely due to two factors. First, a larger percentage (64%) of patients, in comparison to eligible studies, received first generation balloon-expandable TAV without anti-calcification properties. Second, some patients were followed for as long as 10 years, suggesting that the rate of SVD is greater in years 6 to 10 than in the first 5 years following TAVI.
Our review found the pooled incidence rate for SVD to be 28 per 10 000 patient-years. Therefore, at 2 years, approximately 0.6% of patients may experience SVD. This is consistent with evidence from re-intervention (1.0%) rates at 2 years after TAVI in the systematic review of randomised trials.2
Conclusion
For patients undergoing TAVI, evidence warranting moderate confidence indicates that SVD occurs infrequently within the first 5 years post-implant. The incidence of SVD beyond 5 years—a period with likely greater hazard of SVD—remains unknown. As reflected in a recent BMJ Rapid Recommendation of TAVI versus SAVR2—which recommended TAVI for older patients (strong recommendation over 85 years of age, weak 75 to 85) and SAVR for younger patients (weak recommendation 65 to 75 years of age, strong under 65)—the older the valve recipient, the more reassuring are our findings, but the younger the recipient, the less reassuring they become.
Key questions
What is already known about this subject?
In patients undergoing transcatheter aortic valve implantation (TAVI), structural valve deterioration is an infrequent event within the first 2 years post-implantation. The durability of TAVI beyond the first 2 years post-implantation is, however, essentially unknown.
What does this study add?
A systematic review of the available evidence demonstrates that during post-TAVI follow-up of up to 5 years, SVD is probably an infrequent event, with a pooled incidence rate of 28 per 10 000 patient years (95% CI 2 to 73 per 10 000 patient years). There remains no published data beyond 5 years of follow-up.
How might this impact on clinical practice?
For patients considering TAVI who are concerned primarily with valve function over the 5 years post-implantation (eg, those over age 85) our data are reassuring. Existing evidence does not address concerns of younger patients whose choice between TAVI and surgical aortic valve replacement may be critically dependent on TAVI long-term valve durability.
References
Footnotes
Contributors FF, GG, POV conceived the study idea. FF, GG coordinated the systematic review. FF wrote the first draft of the manuscript. FF, RAS designed the search strategy. FF, SB screened abstracts and full texts. FF, SB, RB acquired the data and judged risk of bias in the studies. FF, SS performed the data analysis. All authors interpreted the data analysis and critically revised the manuscript. FF had full access to all of the data in the study, and takes responsibility for the integrity of the data and the accuracy of the data analysis. FF is the guarantor.
Competing interests None declared.
Patient consent No patients were involved in production of this manuscript.
Provenance and peer review Not commissioned; externally peer reviewed.