Article Text

Abstract
Objective Limited data exist on the association between menopause and atrial fibrillation (AF). We sought to examine the relationship between menopausal age, postmenopausal hormone therapy (PHT) use and incident AF.
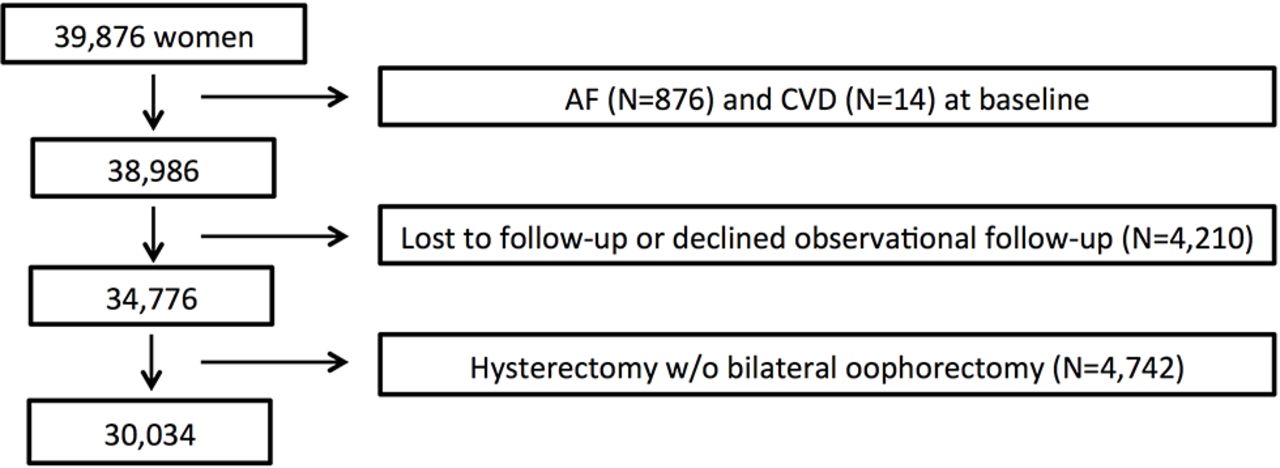
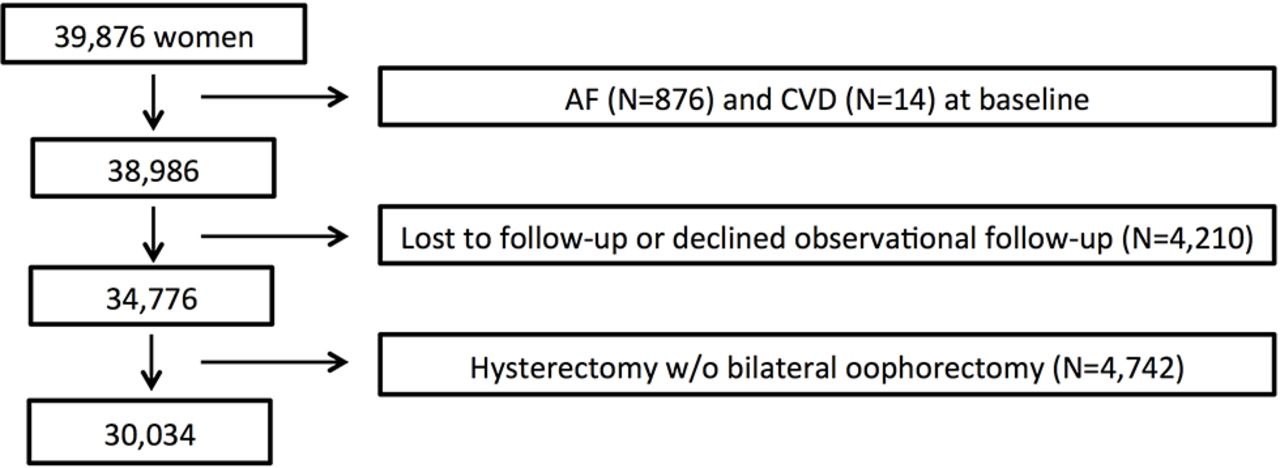
Methods The Women’s Health Study (WHS) enrolled 39 876 female health professionals between 1992 and 1995. We prospectively examined 30 034 women in WHS using Cox proportional-hazard models. Participants were free of cardiovascular disease and AF at baseline and had not undergone hysterectomy without bilateral oophorectomy prior to menopause. Incident AF was confirmed by medical record review.
Results At baseline, median age was 53 years (IQR 49–60), median menopausal age was 50 years (IQR 46–52) and 14 415 (48.0%) had prior PHT use. Over a median follow-up of 20.5 years, 1350 AF events occurred. In multivariable analysis, relative hazards for AF were lower among women with younger age at menopause but did not differ significantly from women with the oldest menopausal age (<45: HR 0.82, 95% CI 0.67 to 1.02; 45–49: HR 0.90, 95% CI 0.74 to 1.08; 50–54: HR 0.89, 95% CI 0.75 to 1.06; >54 years: referent). Use of oestrogen-alone PHT, but not oestrogen and progesterone, was independently associated with AF risk (HR 1.22; 95% CI 1.02 to 1.45 vs HR 1.04; 95% CI 0.86 to 1.26). This relationship was not attenuated by intermediary cardiovascular events.
Conclusions In this large prospective study, menopausal age was not significantly related to incident AF, while use of oestrogen monotherapy was associated with increased AF risk. Our findings suggest a pathophysiological link between unopposed oestrogen exposure and AF in women.
Clinical trial registration NCT000000479; Post-results.
- Atrial fibrillation
- Menopause
- Menopausal Age
- Post-menopausal Hormone Therapy
- Epidemiology
- Women
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) is a rapidly growing healthcare problem.1 Although men are at higher risk of AF than women,2 the prevalence of AF is greater in women after age 75.3 4 Women with AF also have poorer outcomes. Female gender is associated with an increased risk of stroke,3 5 including more disabling and fatal strokes, an increased risk of other AF-related complications3 5–8 and cardiovascular mortality.9–12 Given the significant burden and impact of AF in women, a greater understanding of gender-specific risk factors predisposing women to AF is important.
Early menopausal age has been associated with an increased risk of coronary heart disease, stroke and all-cause mortality.13–15 Previous studies have shown that younger menopausal age is associated with incident cardiovascular disease (CVD), and women with bilateral oophorectomy were at particularly high risk.13 14 16 These findings prompted large randomised trials on postmenopausal hormone therapy (PHT) use.17 18 However, in these studies, PHT use was linked to increased CVD risk. In the Women’s Health Initiative (WHI), women randomised to treatment with conjugated oestrogen and progesterone had a greater risk of incident CVD compared with placebo.18
In contrast, the relationship between menopausal age, PHT use and incident AF remains poorly understood. To date, only three prior studies have examined these associations.19–21 In a modest-sized cohort from the Framingham Heart Study (FHS), no significant association was found between age of natural menopause and incident AF.19 In a subanalysis from WHI, largely based on diagnostic codes for Medicare claims, oestrogen-alone PHT was recently reported to be associated with an increased risk of incident AF.20 A similar observation was reported in a retrospective study.21 Given the high prevalence and adverse impact of AF in women, and the incomplete understanding of the relationship between AF and this important aspect of women’s health, we sought to characterise the relationship between menopausal age, PHT use and incident AF in a large cohort of women free of AF and CVD at baseline using data from the Women’s Health Study (WHS). We hypothesised that early menopause and PHT would both be associated with an increased risk of incident AF, mediated by the development of interim CVD.
Methods
Study population: WHS
The detailed rationale and design of WHS have been described previously.12 22 23 Briefly, WHS was initiated as a randomised controlled trial of low-dose aspirin and/or vitamin E versus placebo for the primary prevention of CVD and cancer in women. Between 1992 and 1995, the study enrolled 39 876 female health professionals aged ≥45 who were free of CVD, cancer or any major illness. On completion of the randomised trial in March 2004, subjects were invited to participate in continued observational follow-up, which is ongoing. The present study consisted of 30 034 women from the WHS. We excluded subjects with a history of AF (n=876) or CVD (n=14) at baseline and women who were either lost to follow-up during the randomised trial period or declined observational follow-up in 2004 (n=4210) since incident AF could not be adjudicated (figure 1). Among those who declined follow-up, only 129 self-reported AF events occurred. Women who underwent hysterectomy without bilateral oophorectomy were excluded from analysis if their surgery occurred before AF onset (n=4742), because age of menopause could not be reliably determined. All participants completed questionnaires on demographics, medical history, CVD risk factors and lifestyle habits at enrolment. Follow-up questionnaires were used to update demographic, lifestyle and CVD risk factors (see online supplementary table 1) and to determine the development of relevant health outcomes. All participants provided written informed consent, and the study was approved by Brigham and Women’s Hospital institutional review board.
{kind=link}
Schematic depicting the study population within the Women’s Health Study. AF, atrial fibrillation; CVD, cardiovascular disease.
Ascertainment of incident AF
Ascertainment of incident AF in WHS has been described previously.12 Briefly, at enrolment, 48 months and annually thereafter, participants reported whether they had been newly diagnosed with AF. Participants who self-reported incident AF after randomisation were contacted and asked for consent to review both inpatient and outpatient medical records. Confirmation of AF required the presence of electrocardiographic evidence or a medical report clearly indicating a history of AF. The earliest date on the medical record was used as the date of AF onset. Medical records could be obtained in approximately 80% of self-reported cases, and of these, 86% were ultimately confirmed to have AF by an endpoint committee of cardiologists. To maximise specificity, only AF cases validated by medical record review were used in this analysis. Person-time was calculated from the time of return of the baseline questionnaire to the date of incident AF, death, loss to follow-up or 31 December 2014, whichever came first.
Assessment of exposure: menopausal status and PHT
Women were asked to report their menopausal status and age at menopause at baseline and at 12, 36, 60, 96 and 126 months. Participants were also asked to indicate the cause of menopause (natural, surgical or radiation/chemotherapy-induced). Participants who reported surgical menopause were asked to indicate whether they had hysterectomy with or without oophorectomy. Data on the type and pattern of PHT use were collected at baseline and at 12, 36, 60, 96, 126, 150, 174 and 210 months. At each time point, women were asked to report their current status of PHT use (never, past use or current use). Those reporting female hormone use since the previous questionnaire were asked to indicate the regimen they had been on the longest from a list of PHT formulations, which included oral Premarin, oral Prempro, oral Estrace/Ogen, oral Premphase and patch oestrogen as well as non-PHT formulations, which included vaginal oestrogen and progesterone or ‘other’ if none of the above applied. Based on these selections, subjects were classified as being on oestrogen, oestrogen and progesterone or other PHT. Women who reported only using non-PHT regimens (ie, vaginal oestrogen) were considered unexposed. Actual PHT start and stop dates were not provided by participants.
Statistical analysis
Age of menopause was determined based on women’s responses on study questionnaires and was categorised into four groups (<45, 45–49, 50–54, >54 years (referent)) based on studies of other CVD endpoints.14 PHT use was examined both in aggregate (never, past or current) and by hormone types (oestrogen alone, oestrogen and progesterone or other). Cox proportional-hazard models using time-in-study as the time scale were used to estimate associations between menopausal age, PHT and incident AF. Initial models were adjusted for multiple prespecified covariates assessed at baseline as categorised in table 1, and time-dependent covariates (including primary exposures) were updated at various time points during follow-up as outlined in online supplementary table 1. Subsequent models were additionally adjusted for surgical/chemotherapy-induced menopause and CVD events during follow-up to assess their potential intermediary role. CVD events included myocardial infarction, stroke, percutaneous coronary intervention and surgical revascularisation. Similar to AF, CVD events were identified by self-report and confirmed by an independent committee of cardiologists through medical record review.
Baseline participant characteristics by menopausal status
Baseline participant characteristics by baseline postmenopausal hormone therapy use
In the age of menopause analysis, baseline age was adjusted for in the final model given the expected collinearity with age of menopause and to be consistent with prior literature.19 For the PHT analyses, pattern of PHT use was modelled as three binary, time-dependent covariates (never, prior use and current use), and type of PHT was modelled as four binary, time-dependent covariates (none, oestrogen, oestrogen and progesterone and other). If a woman reported a change in hormone therapy use, the date of questionnaire return was considered the date of change for analysis purposes. Tests of linear trends across categories of age at menopause were obtained by assigning the median value to each category and modelling this as an ordinal variable in separate Cox models. Since surgical menopause and PHT use may be important confounders or modifiers of the effect of menopausal age on AF, prespecified stratified analyses were performed. Missing values corresponded to <1% for all baseline covariates (table 1) and previous reported values were carried forward to replace missing data during follow-up, which permitted >99% of the data to be analysed as complete cases. The proportional hazards assumption was tested by assessing the interaction between age of menopause or PHT use and the logarithm of time, and no violation was identified. Two tailed p values<0.05 were considered significant. SAS V.9.3 was used for all statistical analysis (SAS Institute).
Results
Participant characteristics
Patient characteristics according to baseline menopausal status and PHT use are summarised in tables 1A and 1B, respectively. Median baseline age of the postmenopausal women was 53 (IQR 49–60) years and median age at menopause was 50 (IQR 46–52) years. Age of menopause was significantly correlated with baseline age (Spearman correlation=0.27, p<0.0001), a relationship that was not significantly attenuated following adjustment for surgical/chPre-reemotherapy-induced menopause (adjusted correlation=0.25, p<0.0001). Participants with earlier menopause were younger, taller and had a lower prevalence of hypertension, but more frequently had history of hypercholesterolaemia, surgical/chemotherapy-induced menopause, smoking and PHT use. Compared with never users, women on PHT at baseline were older, had earlier menopause, lower BMIs, higher prevalence of hypertension and hypercholesterolaemia and were more likely to exercise, consume alcohol and have surgical/chemotherapy-induced menopause.
Age at menopause and incident AF
During a median follow-up of 20.5 years (range: 1 day–21.6 years), 1350 incident AF cases occurred among 30 034 women. Multivariable adjusted HRs and 95% CIs for incident AF according to age of menopause categories are summarised in table 2. There was no significant trend across categories of age at menopause in any of the multivariable models. As compared with women who reported onset of menopause after age 54, women reporting an earlier age of menopause had marginally significant lower HRs for incident AF after controlling for relevant covariates (table 2, Model 3; <45: HR 0.80, 95% CI 0.65 to 0.99; 45–49: HR 0.83, 95% CI 0.69 to 1.00; 50–54 years: HR 0.83, 95% CI 0.69 to 0.98). These relationships were significantly attenuated after adjustment for baseline age leaving only a trend towards a lower risk among the women with menopausal age <45 (table 2, Model 4; HR 0.82, 95% CI 0.67 to 1.02, p=0.07). The association between age of menopause and AF did not significantly differ according to type of menopause (table 3; p interaction=0.45) or by history of PHT use (see online supplemental table 2; p for interaction=0.77). However, fully adjusted stratified analyses did demonstrate a trend towards an inverse association between age of menopause and AF among women with surgical/chemotherapy-induced menopause (table 3, Model 4, p trend=0.06), whereas no such association was observed in women with natural menopause.
Multivariable adjusted HR and 95% CI of incident AF according to age of menopause categories
Multivariable adjusted HR and 95% CI for incident AF according to age of menopause categories, stratified by type of menopause
PHT use and AF
Details on the use of conjugated oestrogen and medroxyprogesterone during the study period are summarised in online supplementary table 3. There was a sharp decline in their use around 120 months of follow-up, approximately when the results from the WHI hormone trials17 18 were made available, after which a total of 856 (64%) incident AF cases occurred. The relationship between PHT use and incident AF is summarised in table 4. In age-adjusted analyses, no significant relationship between PHT use and incident AF was identified. However, following full covariate adjustment, current PHT use was associated with a marginally increased hazard of AF (HR 1.18, 95% CI 1.00 to 1.40, p=0.046). When type of PHT used was examined in multivariable adjusted models (table 5), use of oestrogen-alone, but not combined oestrogen and progesterone, was significantly associated with AF risk (HR 1.21, 95% CI 1.02 to 1.45, p=0.032 and HR 1.04, 95% CI 0.86 to 1.26, p=0.7, respectively). Further adjustment for CVD events during follow-up did not attenuate this relationship (oestrogen-alone: HR 1.22, 95% CI 1.02 to 1.45, p=0.028).
Risk of incident atrial fibrillation by pattern of postmenopausal hormone use
Risk of incident atrial fibrillation by type postmenopausal hormone therapy
Discussion
In this large, prospective study examining the relationship between menopausal age, PHT use and the risk of incident AF, we have identified several important findings. First, age of menopause was not significantly associated with incident AF after controlling for age in multivariable models, although a trend towards a modest decrease in risk remained among women with menopause at <45 years. There was also a weak trend towards an inverse association between age of menopause and AF among the subgroup of women with surgical and/or chemotherapy-induced menopause. Second, compared with never users, current PHT use was independently associated with increased risk of AF. Furthermore, oestrogen monotherapy was associated with increased AF risk, while combined oestrogen and progesterone use was not. Finally, cardiovascular events during follow-up were not important intermediaries in the relationship between PHT use and AF.
To our knowledge, only one other study has evaluated the relationship between menopausal age and AF. In a cohort of 1809 postmenopausal women (mean age 71 years) in the FHS, age of natural menopause was not associated with incident AF events (n=273) over 10 years of follow-up.19 We add to this prior literature by examining the association between age of menopause and AF in a larger, younger and broader cohort of postmenopausal women over a longer follow-up period during which a greater number of AF events accrued. We included women with surgical and/or chemotherapy-induced menopause and also controlled for PHT use and baseline age in the analysis. Despite these differences in study design and power, our results were similarly null, except for the possible modest decrease in AF risk noted in women who underwent menopause at a very early age, usually as the result of surgery or chemotherapy.
Our findings regarding the association between PHT and AF confirm and extend findings from WHI.20 In a substudy of the trial, Perez et al linked participants to Medicare claims data and found that women randomised to oestrogen-alone PHT were at increased risk for AF (HR 1.17, 95% CI 1.00 to 1.36) compared with placebo. Despite significant methodological differences in exposure and outcome assessment, the findings between our two studies are remarkably similar lending strength to the validity of the finding. Interestingly, in both studies, AF risk did not extend to women on oestrogen and progesterone, suggesting that the effect of oestrogen may be mitigated by concurrent progesterone use. PHT regimens used by participants in the present study reflect the general practice patterns in USA over the past 20 years. While there have been substantial changes in the formulations and doses used, particularly after the release of the main results from the WHI hormone trials, the majority of AF cases in our study occurred after WHI, when study subjects were on more contemporary PHT regimens.
The mechanisms behind our observed associations are currently unknown. Adjustment for interim CVD events during follow-up did not significantly change the effect estimates, suggesting that CVD is not a significant intermediary in the causal pathway. This finding is also in keeping with prior literature as there was no apparent association between oestrogen-alone PHT and CVD risk in WHI.17 18 We postulate that our observations may relate to pattern of oestrogen exposure. Oestrogen can affect cardiac ion channel dynamics,24 and postmenopausal women have different repolarisation kinetics and atrial electrophysiological properties compared with their premenopausal counterparts.25–28 Use of oestrogen-alone PHT has been associated with QT-interval prolongation, while no change in the QT-interval was observed in women on oestrogen and progesterone PHT.25 Presumably, these changes in ventricular repolarisation also reflect atrial repolarisation, possibly leading to AF via increased atrial early afterdepolarisations.29 PHT use has also been linked to increased inflammation, which is an important purported mechanism in AF pathogenesis.30 Based on our findings, the pattern of oestrogen exposure (opposed vs unopposed) and pattern of oestrogen decline (abrupt vs natural) may be important components of the underlying mechanism.
The strengths of our study include the large sample size, long follow-up duration and the adjudication of AF and CVD events. Our study adds to an important body of literature examining the relationship between menopausal age, PHT and AF risk. Women with AF remain at an increased risk of stroke and AF-related complications compared with their male counterparts, and a greater understanding of the relationship between hormonal factors and AF risk may lead to novel preventive, risk-modifying, and management strategies in women. Given that three separate studies20 21 have found a modestly elevated AF risk associated with oestrogen-only PHT, this risk may need to be disclosed when initiating and following women on oestrogen-alone PHT.
Several limitations need to be considered. First, the study population was comprised entirely female health professionals, the majority of whom were of European descent; thus, these results may not be generalisable to study populations with less access to healthcare or to women of other races or ethnicities. Second, age of menopause, surgical menopause and PHT use were self-reported and may be subject to misclassification; however, there is literature to support that data in this context are reproducible.14 If present, such misclassification would likely be non-differential and would have biased our results towards the null. Third, PHT start and stop dates were not provided by participants and may have led to misclassification of the exposure, which if differential, may have biased the results away from the null. However, it is unlikely that reporting of PHT use would have differed between women with and without AF. Fourth, AF cases were ascertained by self-report, and as with any AF ascertainment method, there may be biases as to which cases are more likely to be detected by this method. Further, due to the episodic and sometimes asymptomatic nature of AF, some AF episodes may not have been detected. These factors, if non-differential, again would have likely biased our results towards the null. Finally, given the observational nature of WHS and the divergence between observational studies and randomised controlled trials with respect to the relationship between PHT and CVD,17 18 we cannot exclude the possibility that uncontrolled confounding could have contributed to the findings we observed.
Conclusion
In this large prospective study of initially healthy women, we found that oestrogen monotherapy in the setting of PHT use was associated with an increase in incident AF risk, while women with younger age at menopause had relatively lower hazards for AF, a finding which was no longer significant after accounting for baseline age. Our findings suggest a possible pathophysiological link between pattern of oestrogen exposure and AF in women. Future studies to evaluate the underlying mechanisms behind these relationships are warranted.
Key questions
What is already known on this subject?
Younger menopausal age and oestrogen and progesterone postmenopausal hormone therapy (PHT) have been associated with an increased risk of incident coronary heart disease. Although coronary heart disease is strongly associated with incident atrial fibrillation (AF), limited data exist regarding the relationship between age of menopause, PHT use and incident AF.
What might this study add?
We examined the association between menopausal age, PHT use and incident AF among a cohort of 30 034 women free of cardiovascular disease and AF at baseline within the Women’s Health Study. We found that menopausal age was not associated with incident AF after adjustment for relevant covariates, including age and use of PHT. In addition, consistent with a prior study performed in the Women’s Health Initiative, we found that oestrogen-alone PHT, but not oestrogen and progesterone combination therapy, was associated with AF risk. The observed relationship between oestrogen monotherapy and incident AF was not mediated by interim cardiovascular events.
How might this impact on clinical practice?
These data suggest that the pattern of oestrogen exposure may be associated with AF risk in women. In combination with results from prior studies, women treated with oestrogen-alone PHT may be at a modest increased risk for developing AF and education surrounding this potential risk may be provided to women beginning oestrogen-alone PHT.
References
Footnotes
Contributors JAW is the first and corresponding author. He was involved in study design and conception, data analysis and interpretation, drafting and revising of the manuscript, and final approval. He is the guarantor. CMA is the senior author and was involved in study design and conception, data analysis and interpretation, manuscript revision and final approval. KMR and DC were involved in study design, data interpretation, manuscript revision and final approval. RKS was involved in data interpretation, manuscript revision and final approval. MVM was involved in data analysis, manuscript revision and final approval.
Funding This study was supported by grant HL-093613 from the NHLBI to CMA. The WHS was supported by grants HL-043851, HL-080467 and HL-099355 from the NHLBI and grant CA-047988 from the National Cancer Institute. JAW is supported by a Canadian Institutes of Health Research Fellowship award and the Arthur J.E. Child Cardiology Fellowship. DC was supported by a grant of the Swiss National Science Foundation (PP00P3_133681 and PP00P3_159322).
Competing interests None declared.
Ethics approval Brigham and Women’s Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.