Article Text

Abstract
Objective Whether revascularisation is superior to medical therapy in older populations presenting with non-ST-elevation acute coronary syndromes (NSTEACS) remains contentious, with inconclusive evidence from randomised trials. We aimed to compare routine invasive therapy with initial medical management in the elderly presenting with NSTEACS.
Methods MEDLINE, EMBASE and Cochrane Controlled Trial Register were searched for studies comparing routine invasive therapy with initial medical management in patients ≥75 years old presenting with NSTEACS. Endpoints included long-term mortality, myocardial infarction (MI), revascularisation, rehospitalisation, stroke and major bleeding reported as ORs.
Results Four randomised trials and three observational studies met inclusion criteria, enrolling a total of 20 540 patients followed up from 6 months to 5 years. Routine invasive therapy reduced mortality (OR 0.67, CI 0.61 to 0.74), MI (OR 0.56, CI 0.45 to 0.70) and stroke (OR 0.53, CI 0.30 to 0.95). Analyses restricted to randomised controlled trials (RCTs) confirmed a reduction in MI (OR 0.51, CI 0.40 to 0.66), revascularisation (OR 0.27, CI 0.13 to 0.56) and a trend to reduced mortality (OR 0.84, CI 0.66 to 1.06) at the expense of major bleeding (OR 2.19, CI 1.12 to 4.28). Differences in major bleeding were unapparent in more recent studies.
Conclusion Routine invasive therapy reduces MI and repeat revascularisation and may reduce mortality at the expense of major bleeding in elderly patients with NSTEACS. Our findings highlight the need for further RCTs to better determine the effect on mortality and contemporary bleeding risk.
- Acute coronary syndromes
- Percutaneous coronary intervention
Statistics from Altmetric.com
Introduction
Coronary artery disease remains the leading cause of death in those aged ≥75 years, with the elderly presenting with acute coronary syndrome (ACS) having an increased risk of mortality, cardiogenic shock, myocardial infarction (MI) and rehospitalisation.1 2 Non-ST-elevation MI (NSTEMI) (73.52% vs 60.46%) is more prevalent than ST elevation MI (26.48% vs 39.54%) in patients >75 years old compared with those aged ≤75 years.2 Moreover, the diagnosis of ACS can be challenging in elderly patients, who frequently present with atypical symptoms.3
The European Society of Cardiology Guidelines suggest that the elderly be considered for invasive therapy with angiography and revascularisation as a class IIa recommendation.4 Similarly, the American Heart Association recommends guideline-based therapy, invasive therapy and revascularisation if appropriate in patients aged >75 years (level A evidence).5 Despite this, older people are less likely to undergo revascularisation, be admitted to a coronary care unit or be admitted under the care of a cardiologist than younger people.2 6
The evidence regarding revascularisation in older populations with non-ST-elevation ACS (NSTEACS) is primarily derived from small randomised controlled trials (RCTs) and observational studies. Furthermore, the two most recent RCTs reported inconsistent results. The After Eighty study found a reduction in MI (17% vs 30%, p=0.0003) and need for urgent revascularisation (2% vs 11%, p=0.0001) in the routine invasive therapy group compared with those medically managed, but no difference in mortality (25% vs 27%, p=0.53) at 18-month follow-up.7 In contrast, the Italian Elderly ACS study found no differences between routine invasive therapy and initial medical management (MI 7.1% vs 10.7%, p=0.27; mortality 12.3% vs 13.8%, p=0.65) at 1 year.8 The routine provision of invasive therapy thus continues to be controversial. We therefore performed a meta-analysis of available randomised and non-randomised studies to evaluate whether routine invasive therapy was superior to initial medical management in those aged ≥75 years presenting with NSTEACS.
Aims and methods
Study design and selected trials
Meta-analyses pooling together RCT and registry data have been recognised as a way of corroborating findings from RCTs and increasing the precision of conclusions, particularly when randomised data are limited.9 Using the Cochrane Collaboration guidelines,10 electronic searches of MEDLINE (1996–present), EMBASE (1996–present) and the Cochrane Central Register of Controlled Trials (most recent edition) were performed in December 2015 (online supplementary appendix 1).
Trials with the following characteristics were included: (1) RCTs, either restricted to populations aged ≥75 years or reporting outcomes for this patient subgroup, or observational studies where outcomes were presented in the form of adjusted ORs using multivariable regression and/or propensity matching techniques; (2) patients presenting with NSTEACS; (3) comparison of a routine in-hospital invasive strategy (coronary angiography and/or percutaneous coronary intervention or coronary artery bypass grafting during index admission) to selective invasive or medical management during index admission; (4) data available for ≥6-month follow-up and (5) English language. Two reviewers (SRG and DB) independently performed study selection, quality assessment and data extraction. Disagreements were resolved by discussion and adjudication by a third reviewer (HL).
Data extraction included information regarding study type, participants, methods, interventions and outcome measures. Endpoints were all cause death, MI (non-fatal), repeat revascularisation, rehospitalisation, ischaemic stroke and bleeding (major) at in-hospital or final follow-up. A quality assessment of each trial was performed by two authors (SRG and DB). RCTs were assessed using the Cochrane Collaboration risk of bias tool,11 while observational trials was assessed using the Newcastle-Ottawa Scale.12
Statistical analysis
OR with 95% CIs were calculated and when appropriate, effect sizes were pooled (log-transformed ORs) using the inverse variance method. A two-tailed p-value risk of 5% was used for hypothesis testing. Heterogeneity was estimated using the I2 statistic. A fixed effects analysis was used unless there was significant heterogeneity (I²>70%), in which case a random effects analysis model was used.13 We used meta-regression analyses to further explore heterogeneity of treatment effects, stratifying by (1) median age and (2) proportion actually receiving revascularisation in the invasive group. Sensitivity analyses were performed, restricted to (1) RCTs, (2) trials only including older patients ≥80 years old, (3) trials that only recruited patients from the year 2003 onwards. Publication bias was assessed using Funnel plots and Egger’s test. Statistical analysis was performed using Review Manager (RevMan) 5.3 software.14
Results
Of 1252 articles identified, 94 articles were reviewed in full. Seven met inclusion criteria, four RCTs and three observational studies, enrolling a total of 20 540 patients with follow-up ranging from 6 months to 5 years (figure 1). Of the RCTs that reported revascularisation rates, 54.4% (284/522) in the routine invasive therapy were revascularised during the index admission compared with 15.4% (81/526) of those initially medically managed. Two RCTs did not report the breakdown of revascularisation rates during initial admission for the subgroup ≥75 years.15 16

Flow chart of study selection methodology.
Study characteristics
The After Eighty trial was a Norwegian open-label multicentre RCT conducted in 2010–2014 that compared routine invasive therapy (angiography with appropriate revascularisation within 72 hours of presentation) with medical management, in patients with NSTEACS ≥80 years. Of these, 93% had troponin elevation (table 1).7
Characteristics of included studies
The Italian Elderly ACS multicentre RCT8 randomly allocated patients ≥75 years old with NSTEACS in 2008–2010 to early invasive therapy within 72 hours of presentation or an initially medical approach. Troponin elevation was reported in 61% of patients.
The FIR trial was a pooled meta-analysis of individual patient data from three multicentre RCTs (FRISC II, ICTUS and RITA-3) comparing routine invasive therapy with initial medical therapy in a NSTEACS population at 5-year follow-up.16 Our analysis included only the subgroup aged ≥75 years old. The FRISC II trial was conducted in Scandinavian hospitals in 1996–1998, the ICTUS trial was performed in the Netherlands in 2001–2003, while RITA-3 was conducted in the United Kingdom from 1997 to 2001. Patients in the routine invasive group underwent angiography within 48 hours in the ICTUS trial, 72 hours in the RITA-3 trial and 7 days in the FRISC II trial, with subsequent revascularisation when appropriate.
The TACTICS-TIMI 18 trial was an international multicentre RCT in 1997–1999 that compared early invasive therapy in NSTEACS with initial medical therapy.15 Those in the routine invasive treatment strategy underwent angiography 4–48 hours post randomisation, with revascularisation when appropriate.
Three observational studies were included. The Global Registry for Acute Coronary Events (GRACE) compared patients aged ≥80 years with NSTEACS recruited in 1999–2002 undergoing revascularisation (PCI or CABG) during initial hospitalisation with those managed medically.17 Of these, 82% had troponin elevation. Outcomes were adjusted using multivariable analyses. The Acute Coronary Syndromes (ACOS) Registry was a prospective, multicentre observational study conducted in Germany in 2000–2002 in patients aged ≥75 years with NSTEMI comparing patients who underwent angiography with those medically managed. Outcomes adjusted for confounding factors in propensity score analyses.18 The Polish Registry of Acute Coronary Syndromes (PL-ACS) enrolled patients in a nationwide, prospective study of consecutively hospitalised patients aged ≥80 years with NSTEMI in 2003–2009.19 The study reported outcomes for propensity matched subgroups.
Study quality
The RCTs were of high quality as assessed by the Cochrane Collaboration risk of bias tool (online supplementary appendix 2).11 A main limitation was the lack of blinding due to the invasive nature of the intervention. A limited proportion (10.9%–48.5%) of eligible elderly patients were recruited in the most recent two RCTs due to strict inclusion criteria or patient refusal.7 8 The TACTICS-TIMI 18 subanalysis did not report baseline characteristics for the elderly subgroup or perform adjustment of OR to minimise potential confounders.15 FIR had only a small elderly subgroup and also did not report baseline between-group differences in the older subgroup.
Similarly, the observational trials were of acceptable quality as assessed using the Newcastle-Ottawa Scale (score ≥7) (online supplementary appendix 3).12 Limitations include attrition bias in the ACOS Registry (~20% loss of follow-up) and short (6 month) follow-up in GRACE.
There was no significant publication bias as assessed by funnel plot confirmed on Egger’s regression testing (p=0.09), although inspection of the plot suggested an over-representation of studies showing less benefit with invasive therapy (online supplementary appendix 4).
Baseline clinical characteristics
Patients who underwent routine invasive therapy were more likely to be male and have a history of hypertension, hypercholesterolaemia and previous revascularisation (table 2, online supplementary appendix 5). They were less likely to have a history of chronic kidney disease.
Baseline clinical characteristics of total cohort*
Outcomes
Mortality
In-hospital mortality
Three trials reported in-hospital mortality. Invasive therapy reduced in-hospital mortality compared with initial medical therapy (OR 0.65, CI 0.53 to 0.79, p<0.0001, I²=38%) (figure 2A). As only one RCT reported this outcome, with a small number of events (in-hospital mortality with routine invasive therapy compared with initial medical therapy, eight vs five patients, p=0.36),8 the result was primarily due to observational studies. Of the two studies that recruited participants after 2003, in-hospital mortality was lower with invasive therapy (OR 0.67, CI 0.54 to 0.84, p<0.0005, I²=61%) (online supplementary appendix 6).

Mortality.
Mortality at follow-up
Seven studies reported incident mortality at follow-up as OR (figure 2B). Pooling these studies confirmed a significant reduction in mortality following routine invasive therapy with no interstudy heterogeneity (OR 0.67, CI 0.61 to 0.74, p<0.00001, I²=0%). Analyses restricted to the three studies with patient recruitment after 2003 showed a benefit with routine invasive therapy (OR 0.67, CI 0.60 to 0.75, p<0.00001, I²=24%) (online supplementary appendix 7). Sensitivity analyses restricted to RCTs showed an attenuation of benefit with a trend to reduction in mortality with invasive therapy (OR 0.84, CI 0.66 to 1.06, p=0.15, I²=0%) (figure 2C). Meta-regression analysis of studies according to mean age of each study population also demonstrated a trend to reduced effect with increasing age, but there was insufficient power due to the limited number of studies (online supplementary appendix 8). Similarly, meta-regression analysis of studies according to revascularisation rate of each study demonstrated a trend to increasing reduction in mortality with increased difference in the rate of revascularisation between routine invasive and initial medical therapy arms (p=0.30) (online supplementary appendix 9), but was underpowered to detect significant differences.
Myocardial infarction
Data were available from two trials (one RCT) for in-hospital outcomes and five trials for longer term follow-up. In-hospital MI was reduced with invasive therapy compared with initial medical management (OR 0.43, CI 0.30 to 0.61, p<0.00001, I2=0%) (figure 3A).

Myocardial infarction.
Routine invasive therapy significantly reduced MI at follow-up (OR 0.56, CI 0.45 to 0.70, p<0.00001, I²=18%) (figure 3B). MI was also reduced by invasive therapy in analyses restricted to RCTs (OR 0.51, CI 0.40 to 0.66, p<0.00001, I²=0%) (figure 3C). Similarly, subgroup analyses of trials that enrolled people only ≥80 years old also demonstrated the superiority of routine invasive therapy (OR 0.60, CI 0.43 to 0.84, p=0.002, I²=60%) (online supplementary appendix 10).
Revascularisation
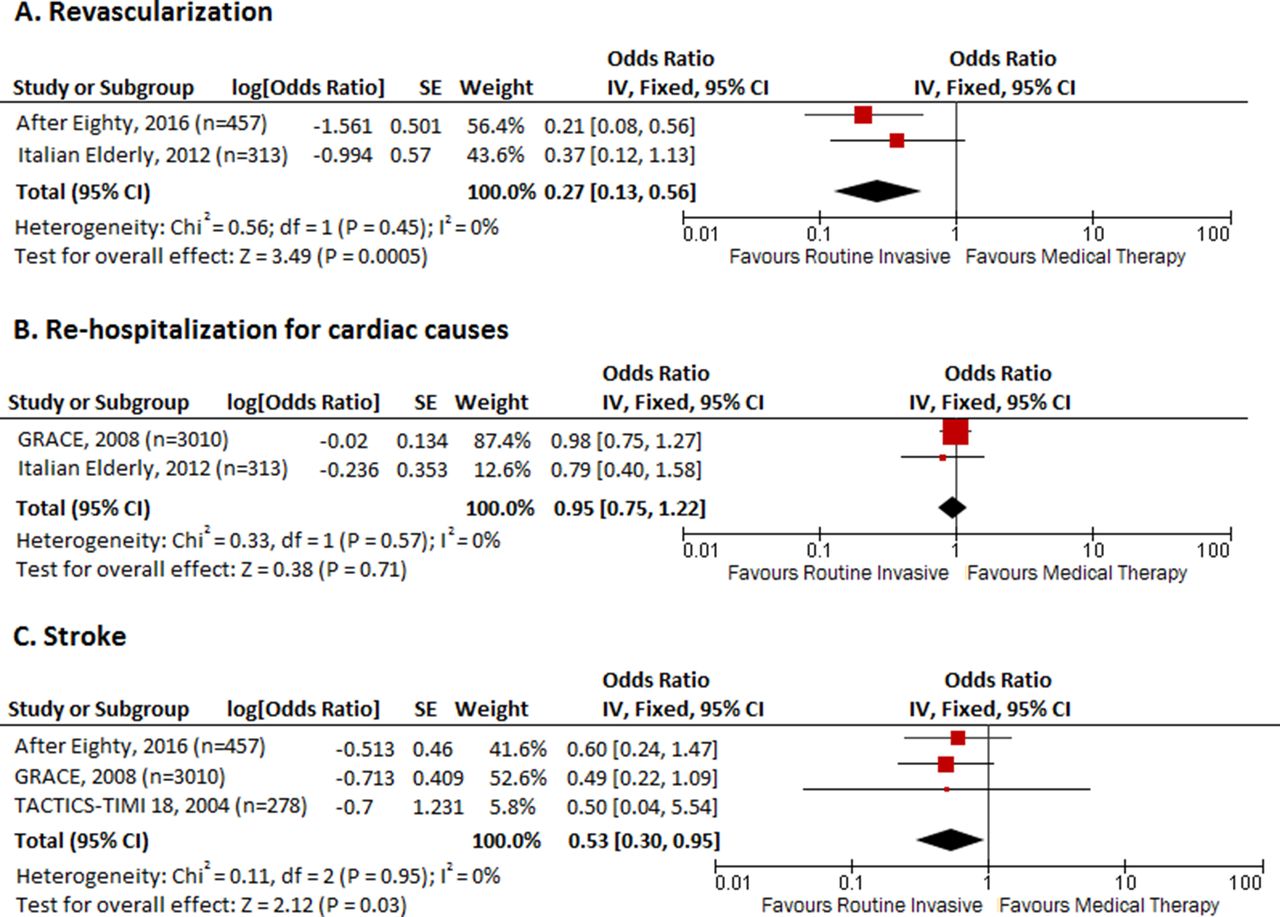
Two studies, both of which were RCTs, reported this outcome. Routine invasive therapy reduced need for revascularisation at 12–18 months compared with those medically managed (OR 0.27, CI 0.13 to 0.56, p=0.0005, I²=0%) (figure 4A).
Rehospitalisation for cardiac causes
Data were available from two studies. There was no difference in rehospitalisation for cardiac causes at 6 or 12 months postdischarge between those undergoing routine invasive management compared with initial medical therapy (OR 0.95, CI 0.75 to 1.22, p=0.71, I²=0%) (figure 4B). One RCT reported this outcome, which found no difference between the groups (10.4% vs 13.2%) at 1 year.8
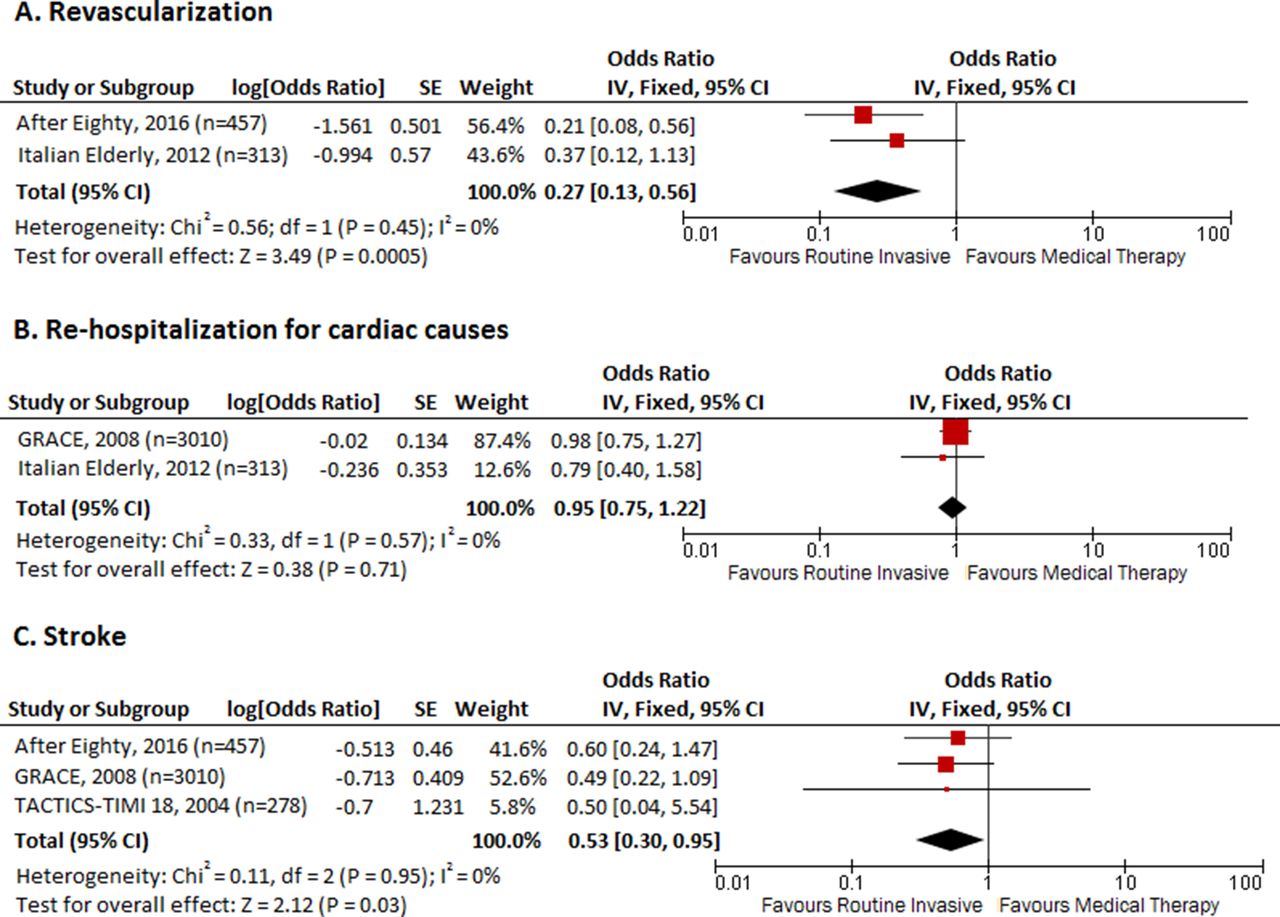
Follow-up revascularisation, rehospitalisation and stroke.
Stroke
Data were available from three trials (two RCTs) for follow-up at 6–18 months. Routine invasive therapy reduced stroke (OR 0.53, CI 0.30 to 0.95, p=0.03, I²=0%) (figure 4C). The superiority of routine invasive therapy persisted in trials enrolling patients ≥80 years old (OR 0.54, 0.29–0.97, p=0.04, I²=0%) (online supplementary appendix 11). Subgroup analyses restricted to RCTs revealed a trend to reduced stroke with routine invasive therapy (OR 0.59, CI 0.25 to 1.36, p=0.21, I²=0%) (online supplementary appendix 12).
Major bleeding
In-hospital major bleeding was reported in two studies and found to be increased in patients undergoing invasive management (OR 2.37, CI 1.53 to 3.68, p=0.0001, I²=30%) (figure 5A).

Major bleeding.
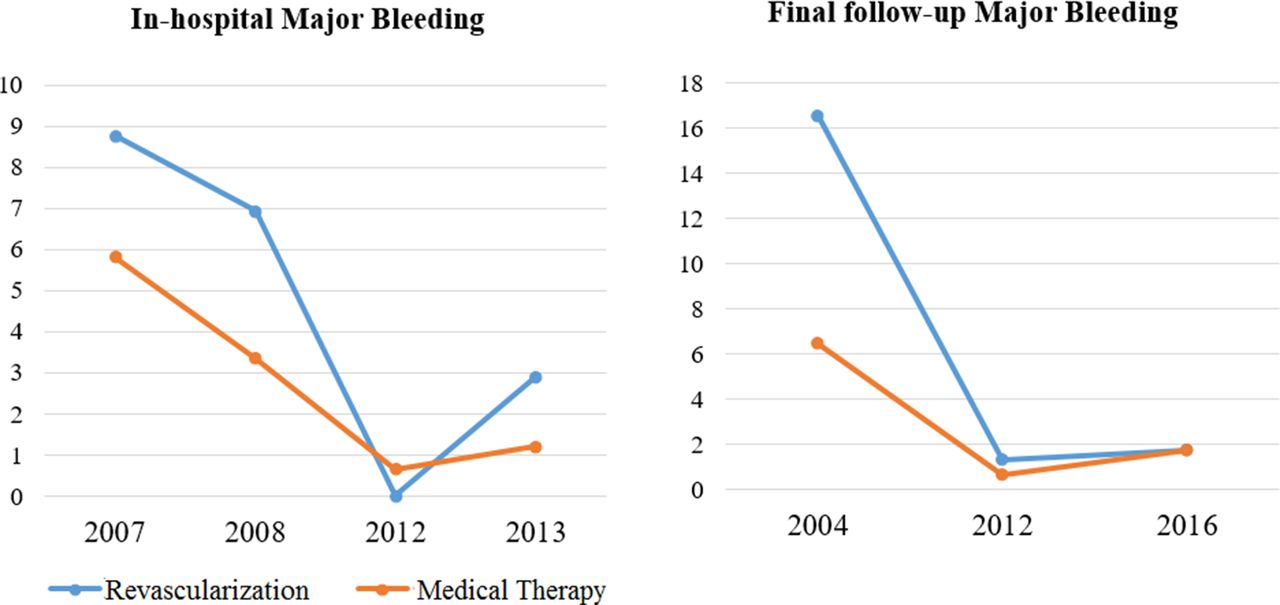
Major bleeding at longer-term follow-up was reported in four studies. Routine invasive management was associated with increased major bleeding (OR 2.38, CI 1.64 to 3.45, p<0.00001, I²=0%) at final follow-up (figure 5B). This was confirmed on sensitivity analysis restricted to RCTs (OR 2.19, CI 1.12 to 4.28, p=0.02, I²=0%) and to studies that recruited participants only after 2003 (OR 2.27, CI 1.49 to 3.44, p=0.0001, I²=0%) (online supplementary appendix 13). However, when the studies were stratified by year of publication, both the overall rate of bleeding and the differences between routine invasive and initially medically managed groups were attenuated (figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Major bleeding rates by year of trial publication (%).
Discussion
The management of NSTEACS in elderly populations poses the challenges of difficult diagnosis, altered physiology, competing comorbidities, frailty and increased vulnerability to adverse outcomes. Although international guidelines recommend consideration of routine invasive therapy, the strongest independent negative predictor of the use of cardiac catheterisation has been demonstrated to be age ≥75 years.20
Our analyses demonstrate a clear reduction in MI (OR 0.56, CI 0.45 to 0.70) and revascularisation (0.27, CI 0.13 to 0.56) at follow-up in elderly patients undergoing invasive therapy. While there was a strong reduction in mortality in the pooled analysis (OR 0.67, CI 0.61 to 0.74), this was attenuated in subgroup analyses of RCTs (OR 0.84, CI 0.66 to 1.04). There are a number of reasons for this discrepancy. First, RCTs use a ‘strategy’ of routine invasive vs selective invasive whereas observational studies compare patients receiving invasive therapy with those that did not. Second, despite restricting our analyses to high-quality observational studies that adjusted for the impact of known confounders, it is almost certain that residual selection bias remained, potentially exaggerating the effect of invasive therapy on mortality. This includes a survivorship bias, whereby patients needed to survive long enough to be offered invasive management. The absence of excess in-hospital mortality in these patients (early hazard) suggests that some residual bias indeed persisted. Additionally, the trend to an increased mortality benefit with increased differences in revascularisation rates on meta-regression analysis further supports an exaggerated mortality benefit in the observational studies. Interestingly, although there was no demonstrable publication bias, visual inspection of the funnel plot does suggest a bias towards publication of studies demonstrating less mortality benefit, rather than the exaggerated benefit assumed in observational studies. Despite the challenges of combining RCT and observational data, the consistent mortality benefit at follow-up across all studies, together with the lack of inter-study heterogeneity supports our approach and suggests that the mortality reduction is likely to be a true finding. One important question remaining is the magnitude of the benefit, from 33% when all studies were pooled to 16% when restricted to RCTs. This can only be answered through further randomised studies in these populations.
Our sensitivity analysis restricted to studies enrolling patients ≥80 years old confirmed the benefits observed in the broader elderly cohort. One important finding from the After Eighty trial was the attenuation of benefit as patients aged, with no reduction in composite outcome in those >90 years (HR of 0.47 in those ≤90 years old vs HR 1.21 in those >90 years). However, the trial could not make definitive conclusions due to small numbers aged ≥90 years (n=34). Our metaregression analysis of the interaction between age and the benefit of an invasive strategy supported this observation, with a non-significant trend to reduced effect with increasing mean age of study participants.
Routine invasive therapy is associated with increased major bleeding at long-term follow-up. Major bleeding is correlated with increased mortality, particularly in older populations with NSTEMI (adjusted OR 1.22 per 10 year age increase, CI 1.10 to 1.35, p=0.002).21 However, bleeding rates have been declining, with recent RCTs demonstrating no excess in major bleeding with invasive therapy.7 8 This may reflect the increased use of radial access, which was the dominant access route in the Italian Elderly ACS and After Eighty trials (radial access 71% and 90%, respectively). Furthermore, in contrast to earlier studies, the recent After Eighty RCT did not use glycoprotein IIb/IIIa inhibitors, a therapy well known to be associated with excess bleeding in older populations.22
Notably, there was no increase in stroke, but an apparent reduction in those who underwent routine invasive therapy at follow-up. Interpretation of this finding should be cautious, because a stroke occurring soon after admission with ACS would very likely preclude angiography and be ‘attributed to’ the medical approach in observational studies and would be a contraindication to randomisation in the RCTs. However, this finding was consistent across the pooled results, with a trend observed in the sensitivity analysis confined to RCTs. Perhaps, this reflects reduced cardioembolic strokes arising from reduction in recurrent infarcts.
These results suggest that we may overestimate risks associated with revascularisation in the elderly and preclude people from otherwise beneficial therapy. Indeed, there have been significant advances in interventional technologies, with increasing evidence that PCI is feasible in elderly patients with complicated anatomy, including left main stenting and complex lesions.23 Furthermore, drug eluting stents have been associated with a reduction in MI and target vessel revascularisation in the elderly, with no difference in major bleeding despite more prolonged dual antiplatelet use.24 Such advances have improved outcomes and the safety profile of revascularisation, allowing consideration of such therapies in older, often frailer populations.
There were a number of limitations to our analysis. Although observational studies were included—which do not provide the same robust evidence as RCTs—they provide relevance to real-world practice. Elderly patients are under-represented in RCTs, with included participants tending to be younger and having lower rates of traditional cardiovascular risk factors, less comorbidities and better haemodynamic status than community populations. Furthermore, there was heterogeneity between trials with regard to study designs, inclusion criteria, length of follow-up, revascularisation rates and PCI technique. We could not ascertain whether the conservatively managed patients in the observational studies were less likely to undergo functional studies or were less symptomatic which could contribute to a selection bias. While medical therapy reflected standard practice at the time of each trial’s publication, there were differences in therapy. Despite these limitations, this study is the largest aggregated meta-analysis of invasive therapy compared with initial medical therapy in older populations.
Conclusion
Routine invasive therapy reduces MI and repeat revascularisation in elderly patients presenting with NSTEACS and may reduce mortality at the expense of increased bleeding. Our findings suggest that age alone should not preclude patients from routine invasive therapy. Further randomised trials in progress should further consolidate the magnitude of mortality benefit, balanced against more contemporary assessment of bleeding in this population.
Key messages
What is already known on this subject?
While coronary artery disease remains the leading cause of death in those aged ≥75 years, older populations are more likely to experience significant disparities in care. Routine invasive therapy in elderly patients with NSTEACS remains contentious, with inconclusive evidence from randomised trials.
What might this study add?
This meta-analysis demonstrates that routine invasive therapy reduces MI, stroke and repeat revascularisation in elderly patients presenting with NSTEACS and may reduce mortality at the expense of an increase in major bleeding.
How might this impact on clinical practice?
Our findings suggest that age alone should not preclude patients from routine invasive therapy. Further randomised trials in progress should further consolidate the magnitude of mortality benefit, balanced against more contemporary assessment of bleeding in this population.
References
Footnotes
Contributors All authors contributed to the paper. SRG and DBB were involved in the planning, literature review, data analysis and writing of the manuscript. LK was involved in the writing of the manuscript. MD was involved in the data analysis. HCL was involved in the planning, literature review and writing of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with ’BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.