Article Text

Abstract
Atrial fibrillation (AF) is frequent in patients with rheumatic mitral stenosis (MS). Pressure overload leads to marked structural and electrical remodelling of left atrium. The frequency of persistent AF increases with age and paroxysmal, asymptomatic, AF seems even more frequent. The occurrence of AF worsens the haemodynamic tolerance of MS and markedly increases the risk of thromboembolic events. AF has a negative impact on the natural history of MS and on its outcome after commissurotomy. The respective indications of rhythm and rate control should be adapted to patient characteristics, particularly the consequences of MS, and take into account the high risk of recurrence of AF. Oral anticoagulant therapy is mandatory when AF complicates MS, regardless of its severity and CHA2DS2-VASc score. Non-vitamin K antagonists oral anticoagulants are not recommended in moderate-to-severe MS due to the lack of data. Percutaneous mitral commissurotomy does not appear to prevent the occurrence of AF in MS but should be considered as the first-line therapy when AF is associated with severe symptomatic MS, followed by the discussion of cardioversion or ablation. AF ablation should be considered in patients with mitral disease requiring intervention, but the ideal timing and techniques are difficult to determine due to the lack of appropriate specific randomised trials in patients with MS.
- mitral stenosis
- atrial fibrillation
- transcatheter valve interventions
- valve disease surgery
- atrial arrhythmia ablation procedures
Statistics from Altmetric.com
- mitral stenosis
- atrial fibrillation
- transcatheter valve interventions
- valve disease surgery
- atrial arrhythmia ablation procedures
Atrial fibrillation (AF) is a common complication of rheumatic mitral stenosis (MS) and has an impact on event-free survival, either spontaneously or after intervention on the mitral valve. The prevention and management of AF raise questions with regard to the respective indications for medical therapy, valvular and rhythm interventions.
We review here the presentation, diagnostic features and prognostic impact of AF in patients with rheumatic MS, and the current knowledge on the effects of medical therapy and valvular interventions.
Presentation and epidemiology of rheumatic MS
MS is most commonly caused by rheumatic fever. The main mechanism of stenosis is commissural fusion, associated with leaflet thickening and, possibly, calcification. These anatomical features differentiate rheumatic MS from degenerative MS, in which mitral annular calcification extends to the leaflets and causes stenosis without commissural fusion.
The prevalence of MS depends on the incidence of rheumatic fever, antibiotic use and medical practices in the countries considered. It was estimated at 0.1% in an American population-based study. MS represented 9% of left-sided native valve disease in Europe in 2001, 85% being of rheumatic origin. In children from low-income and middle-income countries, the prevalence of rheumatic heart disease is estimated at 1–10 per 1000 according to clinical screening, and 20–30 per 1000 when using systematic echocardiographic screening. In a South-African study, MS accounted for 25% of valvular diseases in patients aged between 20 and 30 years and for 10%–20% after the age of 30 years.
Pathophysiology of AF in MS
Haemodynamic consequences of MS
The increase in upstream pressure leads to progressive enlargement of the left atrium (LA) with an important individual variability. The geometric pattern of LA enlargement is inhomogeneous, which explains why LA remodelling is better assessed by the evaluation of LA volume rather than M-mode diameter or planimetry.1
Stenosis severity and haemodynamic consequences are major determinants of AF in MS,2 but age is also important. Rates of persistent AF are <20% in series in which mean age is <35 years while they range between 30% and 60% when >45 (table 1, figure 1).3–15 In a Scottish series of percutaneous mitral commissurotomy (PMC), the rate of sinus rhythm (SR) was 79% before the age of 40 years, 41% between 40 and 54 years, 23% between 55 and 69 years and 15% after 70 years.16 The marked increase of AF incidence with age is consistent with the epidemiology of AF without valvular disease.

Relationship between age and the percentage of patients with arial fibrillation (AF) in the series of percutaneous mitral commissurotomy of table 1.
Frequency of permanent atrial fibrillation (AF) in series of percutaneous mitral commissurotomy. Series are ranked by increasing mean age
Inflammation and structural remodelling
Disease-specific inflammation such as that seen in Aschoff bodies may play a role during acute episodes of carditis and during chronic phases. However, a recent histological study found that Aschoff bodies are uncommon and not statistically associated with AF at the time of surgery. Myocyte hypertrophy and glycogen deposition were predictive factors of SR while the presence of myocytolysis was a significant predictor of AF. Interstitial fibrosis was present in >90% of patients irrespective of rhythm presentation. Beyond histological factors, LA enlargement is associated with the presence of AF. Kim et al followed (median 72 months) 293 patients with rheumatic valve disease in SR at the time of evaluation and 20.5% of patients developed AF (3.5% per year). After univariate analysis, age, cholesterol level, LA diameter and mitral valve area <1.5 cm² were associated with AF occurrence.
Fibrosis is a hallmark of structural remodelling and AF is associated with more extended fibrosis in patients with different types of mitral diseases. In a small series of LA appendage samples obtained during mitral valve replacement, patients with persistent AF were older and had larger LA when compared with patients in SR. They also had a higher degree of fibrosis. In patients with AF, MS was associated with a higher degree of fibrosis despite younger age and less dilated LA when compared with mitral regurgitation.
Non-invasive imaging assessment of atrial fibrosis also suggests an association of the degree of fibrosis and the occurrence of AF during follow-up in patients with MS.
Since LA size and fibrosis are clearly associated with lower odds of maintaining SR by intervention,important difficulties in maintaining SR should be expected (figure 2).
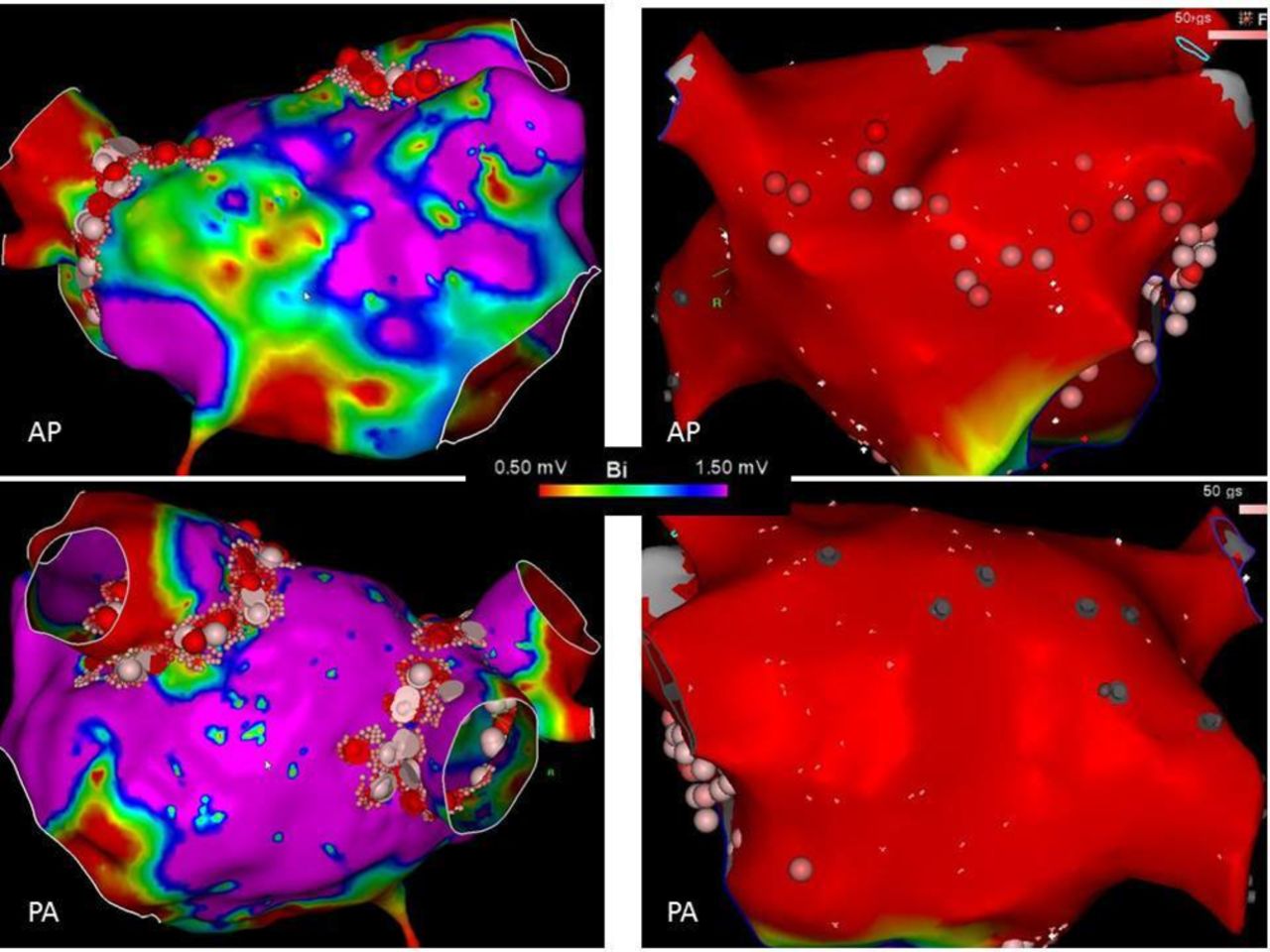
Left atrial bipolar voltage map in two patients without (left side) and with (right side) MS referred for AF ablation. Purple colour reflect normal voltage (>1.5 mV) and red colour low voltage (<0.5 mV). The atrium shown on the right side of the figure is from a patient with a mechanical mitral valve and a long history of persistent AF. The whole atrium shows endocardial voltage below 0.5 mV indicating severe and extensive myocardial disease. AP, anterior view; PA, posterior view.
Pulmonary veins, electrical remodelling and stretch
Despite the probable leading role of fibrosis, non-structural factors should not be overlooked.
The role of pulmonary vein (PV) foci in AF initiation and maintenance has been clearly demonstrated by the Bordeaux group. Accordingly, PV isolation is a cornerstone of AF ablation procedures.17 Conversely, PV firing has been seldom described in AF in patients with MS.18 Paroxysmal AF might be recorded in patients with MS,19 but in these patients, AF is more often persistent, a condition considered as being less dependent on PV foci.
Electrical remodelling (ie, slow conduction and shortened refractory periods) has been shown to be induced by AF and serves as a functional substrate for AF. Electrophysiological evaluation was performed in a small series of patients with MS before commissurotomy and compared with patients referred for left-side accessory pathway ablation.20 MS was associated with a decrease in conduction velocity but an increase in effective refractory periods in both atria.20 In addition, MS was associated with lower atrial voltage and more frequent electrical scar again in both atria.20 The study could not determine whether electrical remodelling preceded or followed structural remodelling. However, the conjunction of both types of remodelling was associated with an increased AF inducibility.20
Atrial stretch induced by pressure overload is another player in AF mechanisms. Evaluation before and after PMC has shown that LA pressure is correlated with AF inducibility.21 The atrial stretch seems to affect both conduction velocity and refractory periods. Different studies found a consistent decrease in conduction times following commissurotomy.21 22 The effect of commissurotomy on the atrial refractory periods is less clear.21 These electrophysiological effects of commissurotomy were mainly observed in patients in SR but not in patients with AF.21
These data suggest that at least part of the electrical remodelling might be related to pressure overload-induced atrial stretch. This is a potential reversible remodelling factor if addressed before the occurrence of extensive structural remodelling.
Diagnosis
Diagnosis of MS
Auscultation reveals a loud first heart sound and an opening snap in early diastole followed by a holodiastolic rumbling murmur. The diagnosis of MS is based on echocardiography. MS is considered significant when valve area is <1.5 cm², preferably according to planimetry which is the reference measurement, but requires expertise. Doppler pressure half-time is influenced by confounding factors, in particular in patients with AF. Mean gradient is not reliable to assess MS severity because it depends on heart rate and flow. It should be averaged in five cycles in AF. Evaluation of anatomy is important to assess aetiology and the suitability of PMC.1
Diagnosis of AF
Most series of MS consider persistent AF, as diagnosed on baseline ECG. Little is known with regard to the frequency of paroxysmal AF in MS. In 63 patients with MS in SR (mean age 49 years), 24 hours Holter ECG showed that 56% had paroxysmal supraventricular arrhythmias (including atrial tachycardia in 40% and AF in 22%) with a mean duration of 5 s, which were asymptomatic in 95%.23 Factors associated with paroxysmal supraventricular arrhythmias were age, LA diameter and valve calcification. A series of 179 patients with MS in SR (mean age 32 years) found 27% of transient AF (duration <30 s) according to Holter monitoring.19 In both studies, paroxysmal AF was associated with an increased risk of thromboembolic events.
Complications of AF in MS
AF impairs the haemodynamic tolerance of MS due to the loss of LA contraction and the shortening of diastole, which leads to a decrease in cardiac output and an increase in mean gradient.
The other complication of AF in MS is thromboembolism. In a retrospective study, the risk of thromboembolic events reaches 5.7% per year for severe MS in patients with AF without anticoagulant therapy (figure 3).24 Thromboembolic events are favoured by blood stasis in the LA, which is reflected by the frequency of LA spontaneous contrast in patients with MS in AF.

Annual rate of new thromboembolic events in 300 patients with mitral stenosis (MS) according to rhythm, the severity of MS and anticoagulation. AF, atrial fibrillation. Data from Horstkotte et al.24
Impact of AF on the outcome of MS
In patients undergoing PMC, AF is associated with other features of advanced heart disease, in particular older age, more severe symptoms, smaller mitral valve area and more severe impairment of valve anatomy,25 26 all of which contribute to decreased event-free survival. Multivariate analysis is therefore mandatory to approach the impact of AF per se on outcome.
The relationship between AF and the natural history of MS is illustrated by a series of 271 patients with medically treated MS (mean age 42 years, 57% in AF). Ten-year and 20-year survival rates were 25% and 0% in patients with AF, respectively, whereas the corresponding figures were 46% and 29% in SR. Mortality was associated with older age and heart failure, but it is unclear whether AF or other patient characteristics was the cause of increased mortality.
The largest amount of data comes from series of PMC. In multivariate analysis, AF is not associated with the quality of immediate results. AF at the time of PMC is associated with a decrease in survival without surgery or repeat PMC and with few or no symptoms (New York Heart Association class I–II) in multivariate analyses on series reporting 19–20 years follow-up.4 14 The same findings were observed after closed-heart commissurotomy.
Medical therapies of AF and its complications
Antiarrhythmic therapy
In rheumatic MS, most patients in persistent AF before PMC fail to revert to SR in the absence of an aggressive antiarrhythmic strategy.27–29 Furthermore, only a few of the patients who do revert remain in SR at follow-up.27 Therefore, combining PMC with an antiarrhythmic strategy seems to offer the best opportunity for rhythm control. This has previously been attempted, in non-randomised studies, with favourable results. Duration of AF, LA size and age are the principal determinants of successful cardioversion and maintenance of SR.28 29 There are no data on the potential usefulness of early antiarrhythmic strategy for paroxysmal AF.
Cardioversion of AF with amiodarone
In most of the published studies, the antiarrhythmic drug used before DC cardioversion (DCCV) in an attempt to restore SR is amiodarone. A major limitation of these studies is that they are open and observational. The rate of conversion under amiodarone alone is relatively low, between 24% and 39%.28 30
Maintenance of SR on amiodarone
Studies of DCCV combined with amiodarone therapy in patients with MS reported a successfully restored SR and maintenance in 49%–81% of patients at a mean follow-up of 18–31 months after PMC,29 31 a success rate apparently surpassing that achieved by catheter-based radiofrequency ablation in this particular group of patients.32 33
DCCV should not be performed too early after the beginning of amiodarone therapy to avoid early relapses. One month of amiodarone administration, with or without initial loading dose, seems appropriate.
The first randomised but apparently open study of a rate versus rhythm control (under amiodarone) strategy immediately following PMC was published in 2006.34 The authors reported an impressive rate of success with a rhythm control strategy with amiodarone (96% of the patients were in SR at 1 year) with concomitant improvements in symptom status, exercise capacity and quality of life. It should be underlined that it was a highly selected population (LA diameter ≤45 mm and AF duration ≤12 months) and that earlier and more recent studies including higher risk patients were not as successful with rhythm control.30 The authors conclude that rhythm control should therefore be considered as the preferred initial therapy for this group of patients but that the optimal strategy to treat AF after PMC, that is, in the long-term, should be individualised, due to the potential side effects of amiodarone in young patients (mean age 37 years).
A recent randomised study demonstrated a significant benefit with amiodarone compared with placebo in the maintenance of SR: 77.5% vs 34.1% (P<0.001), respectively at 3 months following DCCV and 55% vs 17.1% (P=0.001), respectively at 12-month follow-up when amiodarone was continued.35 Patients who were restored and maintained in SR had a better quality of both physical and mental health during the 3-month and 12-month follow-up as assessed by SF8 quality of life survey. Patients in this study had duration of AF varying from 3 months to more than 2 years, and no selection was done regarding the LA size.
One small randomised study evaluated the efficacy of early DCCV along with intravenous loading dose followed by low-dose short duration (100 mg/day during 6 weeks) amiodarone after successful PMC.36 At the end of a short follow-up period (range 6–9 months), 13/15 (87%) patients remained in SR, while 2 patients (13%) had reverted to AF, one at 2 weeks and one at 4 months. The authors underline the fact that such a therapeutic strategy may be important in low-income and middle-income countries where patients may not have the facility for repeated or prolonged hospitalisation.
Alternative medical strategies
Amiodarone is the preferred antiarrhythmic agent because it has been reported to be more effective than sotalol or class I agents for maintenance of SR in AF and is particularly effective in AF in patients with rheumatic disease after mitral valve surgery or PMC.29 31 37
Randomised trials in patients with AF have not demonstrated any outcome advantage of rhythm control strategies, but most of the patients had a non-valvular AF in these studies that are therefore not relevant in this population of patients with MS. Moreover, most of the patients with MS included in the studies dealing with AF are much younger,34 35compared with those studied in the large AF trials, underlying the fact that comparisons between these studies are hazardous.
Most of the studies reporting the efficacy of amiodarone have a short follow-up (6–12 months). Evidence of the safety of amiodarone at long-term follow-up in the MS population is needed, before this strategy can be universally advocated. Dronedarone may also be tested in such populations, in the countries where this drug is available. Class IC agents are likely to be safe in this situation (young patients, low likelihood of coronary artery disease and normal left ventricular function) and need to be tested.
A rate control strategy may also be acceptable in patients with MS who have recurrent AF after failure of initial rhythm control therapy under amiodarone or if amiodarone is contraindicated or not accepted. Heart rate control is a class IIa recommendation in the American Heart Association/ American College of Cardiology (AHA/ACC) Valvular Heart Disease guidelines.38 No recommendation is made in these guidelines and in the updated guidelines published in 2017 regarding antiarrhythmic therapy.39 40 There is no recommendation on this subject in the 2016 European Society of Cardiology (ESC) guidelines for the management of AF.17
Anticoagulant therapy
The efficacy of anticoagulant therapy has been assessed only in retrospective studies (figure 3).24 The high thromboembolic risk justifies immediate anticoagulation using heparin when AF is diagnosed in patient with MS. Prompt rate control is also needed. According to AHA/ACC and ESC/European Association for Cardio-Thoracic Surgery guidelines, permanent or paroxysmal AF is a class I indication for anticoagulation using vitamin K antagonists in rheumatic MS, regardless of stenosis severity and CHA2DS2-VASc score (table 2).39 40 Target International Normalised Ratio (INR) is 2.0–3.0. Aspirin alone is not an alternative. Non-vitamin K antagonists oral anticoagulants (NOACs) are now considered in guidelines for patients who develop AF on aortic valve diseases or mitral regurgitation, due to subgroup analyses of randomised trials. However, NOACs remain contraindicated in patients with MS, since they were excluded from all trials.39 40
Recommendations of European and American guidelines on valvular heart disease concerning the management of MS and AF
Interventional therapies
Interventions of the mitral valve and occurrence of AF
There are no randomised or even comparative studies enabling the effect of mitral intervention on the subsequent occurrence of AF to be assessed. In a series of 181 patients in SR (mean age 48 years) treated by PMC, 20% experienced AF during a mean follow-up of 34 months.41 The occurrence of AF was associated in multivariate analysis with older age and LA enlargement, but not with initial success of PMC. These results suggest that successful PMC does not prevent the occurrence of AF in MS.
Ablation
The ablation of targeted atrial tissue has emerged as an effective rhythm management strategy in patients with AF.17 Still, the indication of AF ablation in patients with MS is not addressed in recent AF management guidelines.17
In small non-randomised series, percutaneous AF ablation was performed at the time of mitral commissurotomy and SR was maintained in 60%–80% of patients after a few years of follow-up.42 43 It is unknown whether these results reflect highly selected patients and predictive factors of procedure success/failure have not been described. In our experience (unpublished data), percutaneous AF ablation performed years after PMC or mitral valve replacement, proved to be long, difficult, even though sometimes associated with important clinical improvement, but was often disappointing because of frequent early and midterm recurrences. Controlled studies evaluating the efficacy and clinical impact of percutaneous AF ablation at different stages of MS are warranted.
The concept of AF ablation was born in the operating room and different techniques have been evaluated during mitral valve surgery (either for MS or regurgitation) in randomised studies.44–46 In the most recent one, 260 patients with persistent or long-standing persistent AF requiring mitral valve surgery were randomised to undergo surgical AF ablation in addition to valve surgery or valve surgery alone.46 Ablation was associated with higher rates of SR at 6 and 12 months (63.2% vs 29.4% in the control group, P<0.001), and a non-significant trend towards a decreased 1-year mortality (HR 0.76; 95% CI 0.32 to 1.84) but at the cost of more pacemaker implantations (21.5 vs 8.1 per 100 patient-years, P=0.01).46 The impact of surgical ablation technique on success rates and the risk of pacemaker implantation have been the subject of intense discussions and comments.
In its 2017 Guidelines, the Society of Thoracic Surgeons stated: ‘Surgical ablation for AF can be performed without additional risk of operative mortality or major morbidity, and is recommended at the time of concomitant mitral operations to restore SR (class I, level A)’.47 The levels of recommendations shown in table 2 are different.
Some studies suggest that SR restoration could be associated with inability to recover atrial contractility and a lack of quality of life improvement.48
In addition, preoperative LA area as well as surgery for MS have been shown to be predictors of AF recurrence.49 Recurrences could also take the form of organised atrial tachycardia/flutters related to incomplete ‘electrical’ conduction block after surgical ablation. Hybrid ablation using a percutaneous catheter ablation might then represent a good solution to restore SR in such patients.
Pacemaker implantation and atrioventricular junction ablation can be considered when ventricular rate cannot be controlled by intensive rate control and failure of rhythm control strategies.17 This general recommendation seems reasonable in patients with MS. Such a decision should be balanced with the low risk of sudden death associated with AV node ablation as well as the dramatic consequences of device infection of patients with mechanical valves.
Finally, the effect of LA reduction on restoration and maintenance of SR is being evaluated in patients undergoing mitral valve replacement.50
Conclusion and clinical implications
The frequency and impact of AF in patients with MS justifies a particular awareness and the first implication is the indication for vitamin K antagonists therapy. Specific studies on NOACs are necessary to determine if they can be used in patients in whom INR monitoring is suboptimal. Indications for medical and interventional antiarrhythmic therapies are difficult to codify since there are few data concerning MS, despite the particularities of anatomic and electric LA remodelling. There is little doubt that AF ablation is more effective than antiarrhythmic drugs in maintaining SR in patients with mitral disease requiring intervention, but they should not be considered without the treatment of MS. However, uncertainties remain on the ideal timing and techniques of intervention. A practical approach is proposed in figure 4, but randomised studies properly powered to demonstrate any clinical benefit of AF ablation are still needed.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proposed approach for atrial fibrillation (AF) ablation in patients with mitral stenosis (MS). PMC, percutaneous mitral commissurotomy.
Supplementary file 1
References
Footnotes
Contributors BI, AL and FE drafted different parts of the manuscript. All of them revised and approved the final draft.
Competing interests BI received Speaker’s fee from Edwards Lifesciences.
Provenance and peer review Commissioned; externally peer reviewed.