Article Text

Abstract
Objective Atrial fibrillation (AF) is common in patients with heart failure (HF), and oral anticoagulants (OAC) are indicated. The aim was to assess prevalence of, predictors of and consequences of OAC non-use.
Methods We included patients with AF, HF and no previous valve replacement from the Swedish Heart Failure Registry. High and low CHA2DS2-VASc and HAS-BLED scores were defined as above/below median. Multivariable logistic regressions were used to assess the associations between baseline characteristics and OAC use and between CHA2DS2-VASc and HAS-BLED scores and OAC use. Multivariable Cox regressions were used to assess associations between CHA2DS2-VASc and HAS-BLED scores, OAC use and two composite outcomes: all-cause death/stroke and all-cause death/major bleeding.
Results Of 21 865 patients, only 12 659 (58%) received OAC. Selected predictors of OAC non-use were treatment with platelet inhibitors, less use of HF treatments, paroxysmal AF, history of bleeding, no previous stroke, planned follow-up in primary care, older age, living alone, lower income and variables associated with more severe HF. For each 1-unit increase in CHA2DS2-VASc and HAS-BLED, the ORs (95% CI) of OAC use were 1.24 (1.21–1.27) and 0.32 (0.30–0.33), and the HRs for death/stroke were 1.08 (1.06–1.10) and for death/major bleeding 1.18 (1.15–1.21), respectively. For high versus low CHA2DS2-VASc and HAS-BLED, the ORs of OAC use were 1.23 (1.15–1.32) and 0.20 (0.19–0.21), and the HRs for death/stroke were 1.25 (1.19–1.30) and for death/major bleeding 1.28 (1.21–1.34), respectively.
Conclusions Patients with AF and concomitant HF do not receive OAC on rational grounds. Bleeding risk inappropriately affects decision-making more than stroke risk.
- medication adherence
- atrial fibrillation
- heart failure
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) is a common comorbidity in patients with heart failure (HF), with prevalence ranging from 21% to 77% and increasing with age and higher left ventricular ejection fraction.1 The onset of AF in patients with pre-existing HF is associated with a two fold increase in mortality, whereas the onset of HF in patients with pre-existing AF is associated with a three fold increased mortality.2
HF is considered to be an independent risk factor for thromboembolic risk in patients with AF3; thus, it is included in the CHA2DS2-VASc score.4 Current European Society of Cardiology guidelines on AF give oral anticoagulant (OAC) therapy IIa B recommendation in AF patients with CHA2DS2-VASc>1. Thus, all AF patients with concomitant HF, accounting for 1 point in CHA2DS2-VASc scoring, should receive OAC.5
Several studies have reported OAC underuse in patients with AF.6 Fear of catastrophic bleeding together with underestimating thrombotic risk might contribute to OAC underuse, in particular in frailer patients such as those with HF, with several concomitant comorbidities and receiving multiple and complex therapies. While use of HF-specific therapy has been well studied,7 the reasons for OAC non-use in AF with HF are less well known.
The aim of this study of patients with AF and concomitant HF was to assess (1) the use of OAC for stroke prevention; (2) clinical predictors of OAC non-use; (3) the role of thrombotic and bleeding risk, evaluated by CHA2DS2-VASc and HAS-BLED scores, respectively, in affecting clinicians’ decision of prescribing OAC and (4) their association with outcomes; and (5) the association between OAC use and outcomes.
Methods
Study protocol and setting
The Swedish Heart Failure Registry (SwedeHF) has been previously described.8 Briefly, it was created in 2000 and spread throughout Sweden in 2003. The only inclusion criterion is clinician-judged HF. Approximately 80 variables are recorded at discharge from hospital or after outpatient clinic visit on a web-based case report form and entered into a database managed by the Uppsala Clinical Research Center, Uppsala, Sweden. In 2014, the coverage of SwedeHF was 53%.
The Swedish Board of Health and Welfare administers the Population Registry and the Patient Registry. The Population Registry provided date of death. From the Patient Registry, we obtained additional baseline comorbidities and the outcomes stroke/transient ischaemic attack and severe bleeding, defined according to the InternationalClassification of Diseases 10th revision (ICD-10) codes (ICD-10 codes for outcomes reported in the online supplementary materials).
Statistics Sweden maintains socioeconomic data on all Swedish permanent residents and provides additional baseline data. All permanent residents in Sweden have unique personal identification numbers that allows linking of disease-specific health registries and governmental health and statistical registries.
Establishment of the HF registry and this analysis with linking of the above registries were approved by a multisite ethics committee. Individual patient consent was not required, but patients were informed of entry into national registries and allowed to opt out.
In the current study, HF patients with AF, no history of valve intervention and with no missing data for use of OAC, left ventricular ejection fraction or the variables needed for the calculation of CHA2DS2-VASc and HAS-BLED scores were considered. CHA2DS2-VASc and HAS-BLED scores were calculated as reported in the online supplementary materials. The exposure to OAC was analysed at baseline (first registration), without consideration of potential crossover during follow-up.
Statistical analysis
Baseline characteristics
Baseline characteristics of patients receiving versus those not receiving OAC were compared by t-test or Wilcoxon Mann-Whitney to test continuous variables, and by χ2 to test categorical variables. Missing data were managed by multiple imputation using chained equations method (n=10). Variables labelled with * in table 1 together with OAC, dialysis, malignant cancer within the last 3 years and the outcomes have been considered for the imputation procedure. All the analyses except for descriptive statistics were performed on imputed data.
Baseline characteristics
Predictors of OAC use/non-use
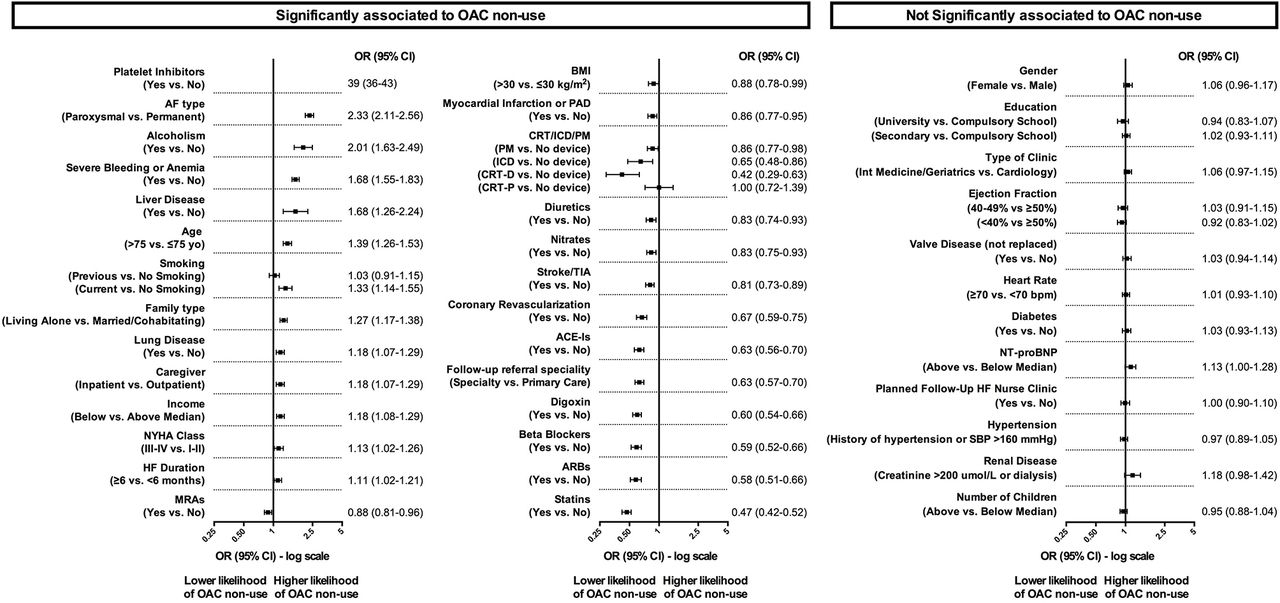
Multivariable logistic regression models were performed including OAC use as dependent variable and CHA2DS2-VASc and HAS-BLED scores together with the variables reported in figure 1 that did not contribute to the calculation of the scores as independent covariates, in order to assess the association between CHA2DS2-VASc and HAS-BLED scores and OAC use. CHA2DS2-VASc and HAS-BLED scores were included as continuous variables in one model in order to investigate the association between 1-unit increase of scores and the likelihood of receiving OAC, and categorised as > versus <median in another model in order to investigate the association between high versus low scores and OAC use. Multivariable regression models were also fitted including OAC non-use as dependent variable and the individual components of CHA2DS2-VASc and HAS-BLED scores together with all the variables reported in figure 1 as covariates, in order to assess the predictors of OAC non-use.

Independent predictors of OAC non-use. AF, atrial fibrillation; ARBs, angiotensin receptor blockers; BMI, body mass index; CRT, cardiac resynchronisation therapy; HF, heart failure; ICD, implantable cardiac defibrillator; MRA, mineralocorticoid receptor antagonist; NT-proBNP, N-terminal pro-b-type natriuretic peptide; NYHA, New York Heart Association; OAC, oral anticoagulant; PAD, peripheral artery disease; PM, pacemaker; SBP, systolic blood pressure; TIA, transient ischaemic attack.
Association between CHA2DS2-VASc and HAS-BLED, OAC use and outcomes
Kaplan-Meier curves and adjusted Cox regressions were fitted to evaluate the association between CHA2DS2-VASc score (also adjusted for HAS-BLED and OAC use) and the composite of all-cause death and stroke, and between HAS-BLED score (also adjusted for CHA2DS2-VASc and OAC use) and the composite of all-cause death and major bleeding. CHA2DS2-VASc and HAS-BLED scores were included as continuous variables in one model to investigate the association between 1-unit increase of scores and outcomes, and categorised as > versus <median in another model in order to investigate the association between high versus low scores and outcomes together with the variables reported in figure 1 that did not contribute to the calculation of the scores as covariates. Kaplan-Meier curves and adjusted Cox regression models (adjusted for CHA2DS2-VASc and HAS-BLED and the variables reported in figure 1 that did not contribute to the calculation of the scores) were also performed to investigate the association between OAC use and outcomes in the overall population and according to the different combinations of high/low thrombotic and bleeding risk. The proportional hazards assumption was tested on the basis of Schoenfeld residuals and met.
In all the analyses, continuous variables were categorised as reported in figure 1. Year of registration was included as potential confounder in all the multivariable models.
Statistical analyses were performed by Stata V.14.2 (Stata) or IBM SPSS Statistics V.24.0 (IBM). A P value<0.05 was considered statistically significant.
Results
Patients
Between 11 May 2000 and 31 December 2012, 80 772 registrations were recorded from 51 060 unique patients. Of these, 21 865 were patients with HF and concomitant AF who reported no missing data for OAC use and all the variables needed for the calculation of CHA2DS2-VASc and HAS-BLED scores: 12 659 (58%) patients were receiving OAC therapy and 9206 (42%) were not (online supplementary figure S1).
Baseline characteristics
In the overall population, the mean age was 76±10 years, 37% were women, 26% had HF with preserved (HFpEF), 22% with mid-range and 52% with reduced ejection fraction. Median CHA2DS2-VASc and HAS-BLED scores were 4 and 2, respectively. Median follow-up was 1.95 (IQR: 0.76–3.82). 19.3 per 100 patient-years died/reported a stroke; 18.8 per 100 patient-years died/reported a major bleeding (table 1).
Patients not receiving versus those receiving OAC were more likely to be female, older, inpatients, registered in and referred to non-specialty care, to have HFpEF, to report clinical characteristics linked to a more severe HF, to have more paroxysmal versus permanent AF, history of both stroke and severe bleeding and comorbidities. Furthermore, they received less HF treatments but more diuretics and antiplatelet therapy. Finally, they were more likely to live alone and to report characteristics linked to a lower socioeconomic status.
Association between single characteristics and OAC non-use
Differences in table 1 are unadjusted. Adjusted ORs for OAC non-use are shown in descending order of magnitude in figure 1, and included prior bleeding, absence of prior stroke, treatment with platelet inhibitors, paroxysmal versus permanent AF, age and comorbidities, variables related to a more severe HF (higher New York Heart Association (NYHA) class and longer HF duration), socioeconomic factors and non-use of cardiovascular medications.
Association between CHA2DS2-VASc and HAS-BLED scores and OAC use
After adjustments for potential confounders, a 1-unit increase in CHA2DS2-VASc and HAS-BLED was associated with OR=1.24 and 0.32 for OAC use, respectively (figure 2A). When scores were dichotomised at medians, the ORs for OAC use were 1.23 and 0.20 in high versus low CHA2DS2-VASc and HAS-BLED, respectively (figure 2B). Additionally, as compared with low CHA2DS2-VASc/high HAS-BLED, the OR for OAC use was 1.76 in high CHA2DS2-VASc/high HAS-BLED, 6.90 in low CHA2DS2-VASc/low HAS-BLED and 7.18 in high CHA2DS2-VASc/low HAS-BLED (figure 3A).

Likelihood of oral anticoagulant (OAC) use and prognosis according to 1-unit increase in high versus low CHA2DS2-VASc and HAS-BLED scores. OR for OAC use (A) per 1-unit increase in CHA2DS2-VASc and HAS-BLED scores and (B) in patients with high versus low CHA2DS2-VASc and HAS-BLED scores. HRs for all-cause death/stroke and all-cause death/major bleeding (C) per 1-unit increase in CHA2DS2-VASc and HAS-BLED scores and (D) in patients with high versus low CHA2DS2-VASc and HAS-BLED scores, respectively. *High and low CHA2DS2-VASc and HAS-BLED scores are defined according to the median values (low≤median, high>median).

Likelihood of oral anticoagulant (OAC) use (A) and outcomes (B) according to the different combinations of CHA2DS2-VASc and HAS-BLED scores. High and low CHA2DS2-VASc and HAS-BLED scores are defined according to the median values (low≤median, high>median).
Association between CHA2DS2-VASc and HAS-BLED and outcomes
After adjustments, 1-unit increase in CHA2DS2-VASc was associated with HR=1.08; whereas for all-cause mortality, 1-unit increase in HAS-BLED was associated with HR=1.18 (figure 2C). When scores were dichotomised at medians, high versus low CHA2DS2-VASc had an HR=1.25 for all-cause mortality/stroke and high versus low HAS-BLED had HR=1.28 for all-cause mortality/major bleeding (figure 2D). Additionally, as compared with low CHA2DS2-VASc/high HAS-BLED, the risk of all-cause mortality/stroke was reduced in low CHA2DS2-VASc/low HAS-BLED (HR=0.74), increased in high CHA2DS2-VASc/high HAS-BLED (HR=1.16) and similar in high CHA2DS2-VASc/low HAS-BLED (HR=0.97), whereas the risk of all-cause mortality/major bleeding was reduced in low CHA2DS2-VASc/low HAS-BLED (HR=0.71) and high CHA2DS2-VASc/low HAS-BLED (HR=0.92), but increased in high CHA2DS2-VASc/high HAS-BLED (HR=1.10) (figure 3B).
Association between OAC and outcomes
In the overall population, OAC was associated with a significant reduction in risk of all-cause mortality/stroke (HR=0.74) and also of all-cause mortality/major bleeding (HR=0.78) (figure 4A). In particular, OAC was associated with a significant lower risk of all-cause mortality/stroke and all-cause mortality/major bleeding in low CHA2DS2-VASc/low HAS-BLED (HR=0.66 and 0.70, respectively), in high CHA2DS2-VASc/low HAS-BLED (HR=0.75 and 0.78) and in high CHA2DS2-VASc/high HAS-BLED (HR=0.77 and 0.84), but not in low CHA2DS2-VASc/high HAS-BLED (HR=0.95 and 0.97) (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between oral anticoagulant use (OAC) and risk of all-cause death/stroke and all-cause death/major bleeding in the overall population (A) and according to the different combinations of CHA2DS2-VASc and HAS-BLED scores (B). Solid lines=OAC use yes; dash lines=OAC use no. High and low CHA2DS2-VASc and HAS-BLED scores are defined according to the median values (low≤median, high>median).
Discussion
In the large and unselective nationwide SwedeHF, we made numerous concerning observations: (1) only 58% of patients with HF and AF received OAC; (2) non-use was associated with numerous factors that increase the risk for stroke, such as higher age, frailty, severity of HF and comorbidity; with paroxysmal versus permanent AF; with inappropriate use of platelet inhibitors in lieu of OAC; with lower socioeconomic class and lower use of specialty care and other cardiovascular medications; (3) non-use was also associated with lower CHA2DS2-VASc and higher HAS-BLED as expected, but (4) HAS-BLED reduced the use much more than CHA2DS2-VASc increased the use; and (5) non-use was associated with poor outcomes.
Underuse of OAC in patients with AF and concomitant HF
OAC therapy has been demonstrated to reduce the risk of stroke in patients with AF and is recommended by AF guidelines in those with AF and CHA2DS2-VASc>1,5 that is, all patients with HF. However, several studies report OAC underuse in patients with AF and, in particular, in those with AF and concomitant HF.9 10 Among over 40 million US patients with AF, only 45.6% received OAC, almost 6 million had AF with concomitant HF and 50.2% of them received OAC.11 Among 108 791 Danish patients with a first AF event, 43.5% of them received OAC, whereas OAC use was even more limited (37.5%) in patients with concomitant HF.12 In the Euro Heart Survey on AF, the rates for OAC use were 52% in the overall AF population and 41% in patients with AF and concomitant HF.13
In our analysis, 58% of patients with AF and concomitant HF received OAC. The higher OAC use in our study compared with other national cohorts may be explained by the high quality of anticoagulation management in Sweden, with dedicated clinics achieving time in therapeutic range for warfarin even higher than in randomised clinical trials.14 But the low use in our and other studies demands a more targeted assessment of the reasons for non-use and whether these reasons may be mitigated. Previous studies have observed expected risk factors for underuse, such as higher age, which may represent age itself or be a marker for frailty.15 16 Prior to our study, there were limited data from multivariable analyses providing independent factors for underuse.15 16
Patients' characteristics independently associated with OAC underuse
HF is an independent predictor of stroke in patients with AF,3 but it is also often associated with conditions determining higher bleeding risk (higher age, renal, liver disease).17 Additionally, AF patients with concomitant HF using warfarin have been shown to spend less time in therapeutic range compared with those with AF alone, suggesting more difficult anticoagulation management.18 19 The fear for OAC use in frailer patients was confirmed in our analysis, with lower use with more severe HF (higher NYHA class, N-terminal pro-b-type natriuretic peptide levels, longer HF duration), lower body mass index and inpatient versus outpatient. These observations may be explained by (1) inappropriately considering HF per se as a risk factor for bleeding, with more severe HF associated with higher risk of bleeding, and (2) the assumption that sicker patients with HF are expected to die because of HF before having the chance to develop stroke secondary to AF; thus, exposing these patients to OAC may increase the risk of bleeding without preventing any stroke event. We also reported older age being considered as an independent predictor of OAC non-use although stroke risk is much higher in elderly than in the general population. Thus, again, the high prevalence of concomitant comorbidities and, thus, the frailty status, together with polypharmacy may make physicians less confident to initiate OAC, even though it is even more effective in these patients.20
Our study suggests that the misconception of aspirin for stroke prevention in AF being safer than OAC in elderly, and more generally in frailer patients as those with HF, still drives physicians’ practice. However, this practice is not supported by data since in this setting OAC has been demonstrated to be (1) substantially more efficacious than antiplatelet agents in reducing stroke risk (by approximately 40%), (2) associated with an absolute risk reduction of stroke that is greater than the absolute risk increase in major bleeding risk21 22 and (3) report similar yearly major bleeding rates as compared with antiplatelet agents in high risk subgroups.22 Thus, there is no evidence supporting aspirin use, as reflected by the IIIA recommendation (harm) for antiplatelet monotherapy in stroke prevention.5 Another misconception suggested by ours and other studies is that OAC is less needed in patients with paroxysmal versus permanent AF. Although there is contrasting evidence, with stroke/mortality risk being higher23 24 or equivalent25 in permanent versus paroxysmal AF, annual stroke rates in paroxysmal AF (2.2%) are high enough to recommend OAC for prevention in these patients.24
Finally, socioeconomical factors such as lower income and living alone, and organisational factors such as non-specialist care, were independently associated with OAC non-use, suggesting that tailored patient information and equal access to specialist care could improve OAC use.
Underestimating thromboembolic and overestimating bleeding risk
OAC underuse may be related to an erroneous estimation of bleeding risk. Indeed, it has been recently shown that bleeding risk scores overemphasising modifiable risk factors perform suboptimally compared with HAS-BLED and, thus, may lead to OAC withholding based on only a temporary increased bleeding risk.26 On the other hand, OAC underuse in patients with AF may be related to an underestimation of its benefits (ie, reduction of stroke risk) and an overestimation of its complications risk (ie, bleeding). Indeed, in a survey in Canada, physicians estimated the relative risk reduction for stroke to be 53% whereas in randomised clinical trials it has been shown to be 68%, and perceived a 10% absolute risk of major bleeding in patients with AF receiving OAC whereas the true estimate has been shown to be 1%.27 Other studies showed that physicians were less likely to prescribe OAC for 1 year after that one of their patients experienced a major bleeding episode under OAC therapy and felt responsible for that, whereas those who had one of their patients suffering from a stroke due to lack of OAC therapy felt less responsible for this outcome and did not change their OAC prescription strategy.28 29
We confirmed underestimation of thrombotic risk and overestimation of bleeding risk as major determinants of OAC undertreatment. High versus low or 1-unit increase in CHA2DS2-VASc and HAS-BLED scores predicted comparable increased risk of all-cause mortality/stroke and all-cause mortality/major bleeding, respectively. However, they had a substantially different weight in driving the OAC use decision-making. Indeed, the likelihood of receiving OAC was 1.2–1.3 fold increased in high versus low or for 1-unit increase in CHA2DS2-VASc, but fivefold decreased in high versus low or for 1-unit increase in HAS-BLED. Additionally, in patients with low HAS-BLED, the likelihood of OAC use was independent from CHA2DS2-VASc and, overall, sevenfold higher than in those with low CHA2DS2-VASc and high HAS-BLED, whereas in those with high CHA2DS2-VASc and high HAS-BLED the risk was only doubled. Finally, OAC were successful in reducing all-cause mortality/stroke risk without any increase in risk of all-cause mortality/major bleeding risk regardless of thrombotic/bleeding risk, suggesting that the reduction in mortality due to stroke induced by OAC was greater than the increase in bleeding risk or bleeding-related mortality.
Study limitations
Our observational study is subject to selection bias. Although all the analyses were performed adjusting for extensive variables, we cannot rule out potential unmeasured confounders. There were some deviations from the original definition of CHA2DS2-VASc/HAS-BLED, with non-steroidal anti-inflammatory drugs and normalised international ratio not available. However, time in therapeutic range in Sweden is high; thus, we are confident in excluding a major effect of ‘labile normalised international range’ on bleeding risk estimate in our cohort.14 Our definition of major bleeding did not include intracranial haemorrhage; however, since haemorrhage-related mortality is very high, it is reasonable that the composite all-cause mortality/bleeding included most of these events. Additionally, treatment for any individual may be entirely appropriate and conducted in accordance with all known evidence. We considered OAC use in the pre-novel OAC era. Overall, OAC use in patients with AF in Sweden has improved after the introduction of NOAC;30 thus, OAC underuse might be somehow mitigated today as compared with the past. However, guidelines on the estimation of thrombotic and bleeding risk in patients with AF have not changed; thus, our considerations on the reasons for OAC underuse may still apply today. National patient registry has complete follow-up; however, we cannot rule out few losses to follow-up among those who permanently moved abroad. Finally, generalisability of our findings to other countries depends on similarities in healthcare system and management of AF.
Conclusions
Patients with AF and concomitant HF do not receive OAC on rational grounds. Bleeding risk inappropriately affects decision-making more than stroke risk.
Key messages
What is already known on this subject?
Several studies have reported oral anticoagulant (OAC) underuse in patients with atrial fibrillation (AF). In particular, there are concerning signals for OAC underuse in patients with AF and concomitant heart failure (HF), who all have recommendation to receive OAC (CHA2DS2-VASc>1) according to the current guidelines, but the reasons for that have not been investigated.
What might this study add?
We confirmed OAC underuse in patients with AF and concomitant HF. We reported frailty status, underestimation of thrombotic risk and overestimation of bleeding risk as major determinants of OAC underuse, suggesting a generalised fear of OACs in frailer patients despite their greater stroke risk.
How might this impact on clinical practice?
Our study may lead physicians to a more conscious use of OAC in frailer patients as those with HF, and scientific community to the definition of clear guidelines able to facilitate the OAC decision-making in frailer populations in which the stroke/bleeding risk evaluation may be not easy in the daily clinical practice.
Acknowledgments
Preliminary data from the current study have been presented at the Heart Failure Congress 2017 in Paris and at the European Society of Cardiology Congress 2017 in Barcelona.
References
Footnotes
Contributors GS contributed to the conception and design of the research, analysis and interpretation of data, drafting and revising the manuscript. LHL contributed to the conception and design of the research, drafting and revising the manuscript, obtaining funding and supervising work. US, LF and UD performed a critical revision of the manuscript for important intellectual content.
Funding This study was supported in part by grants to LHL’s institution from the Swedish Research Council [grants 2013-23897-104604-23 and 523-2014-2336], the Swedish Heart Lung Foundation [grants 20120321 and 20150557], the Stockholm County Council [grant 20110120].
Competing interests GS: none related to this manuscript. Research grant from MSD Italy and Swedish Heart- Lung Foundation. US: none related to this manuscript. US was supported by grants from the Swedish Society of Medicine, Karolinska Institutet Foundations and Funds, the Mats Kleberg Foundation (grant number 2016-00015), the Swedish Heart-Lung Foundation (grant numbers 20160522 and 20160525), the Swedish Heart and Lung Association (grant number E101/16), Regional ALF agreement between Stockholm County Council and Karolinska Institutet (grant number 20160329), Åke Wiberg Foundation (grant number M16-0081) and Magnus Bergvall Foundation (grant number 2016-01396) LF: none related to this manuscript. Research grants and consultancy fees from Bayer, BMS, Pfizer and Sanofi. UD: none related to this manuscript. Research grant to the author’s institution from AstraZeneca and honoraria/consultancies to author’s institution from Novartis and AstraZeneca. LHL: there are no conflicts of interest related to the work submitted. Outside the work submitted, there are the following potential conflicts of interest: research grants to author’s institution, speaker’s and/or consulting fees: AstraZeneca, Novartis, Bayer, Vifor Pharma, Relypsa, Boston Scientific, StJude, Medtronic, HeartWare.
Ethics approval Regionala erikprövningsnämnden i Linköping.
Provenance and peer review Not commissioned; externally peer reviewed.