Article Text

Abstract
Objective To describe the long-term outcomes, treatment pathways and risk factors for patients diagnosed with hypoplastic left heart syndrome (HLHS) in England and Wales.
Methods The UK’s national audit database captures every procedure undertaken for congenital heart disease and updated life status for resident patients in England and Wales. Patients with HLHS born between 2000 and 2015 were identified using codes from the International Paediatric and Congenital Cardiac Code.
Results There were 976 patients with HLHS. Of these, 9.6% had a prepathway intervention, 89.5% underwent a traditional pathway of staged palliation and 6.4% of infants underwent a hybrid pathway. Patients undergoing prepathway procedures or the hybrid pathway were more complex, exhibiting higher rates of prematurity and acquired comorbidity. Prepathway intervention was associated with the highest in-hospital mortality (34.0%).
44.6% of patients had an off-pathway procedure after their primary procedure, most frequently stenting or dilation of residual or recoarctation and most commonly occurring between stage 1 and stage 2.
The survival rate at 1 year and 5 years was 60.7% (95% CI 57.5 to 63.7) and 56.3% (95% CI 53.0 to 59.5), respectively. Patients with an antenatal diagnosis (multivariable HR (MHR) 1.63 (95% CI 1.12 to 2.38)), low weight (<2.5 kg) (MHR 1.49 (95% CI 1.05 to 2.11)) or the presence of an acquired comorbidity (MHR 2.04 (95% CI 1.30 to 3.19)) were less likely to survive.
Conclusion Treatment pathways among patients with HLHS are complex and variable. It is essential that the long-term outcomes of conditions like HLHS that require serial interventions are studied to provide a fuller picture and to inform quality assurance and improvement.
- quality and outcomes of care
- Fontan physiology
- complex congenital heart disease
- congenital heart disease surgery
Statistics from Altmetric.com
- quality and outcomes of care
- Fontan physiology
- complex congenital heart disease
- congenital heart disease surgery
Introduction
Hypoplastic left heart syndrome (HLHS) represents one of the most complex and high-risk forms of congenital heart disease (CHD), and treatment options have evolved dramatically in the last 30 years.1
The possible treatment pathways that patients with HLHS can undergo in the UK are summarised in figure 1. Treatment generally begins soon after birth, and completion of the stage 3 Fontan operation usually takes place before primary school age. A recently introduced alternative to the traditional surgical pathway is the combined surgical and interventional cardiology pathway referred to as the hybrid procedure.2 A minority for whom these pathways fail are diverted to transplantation.
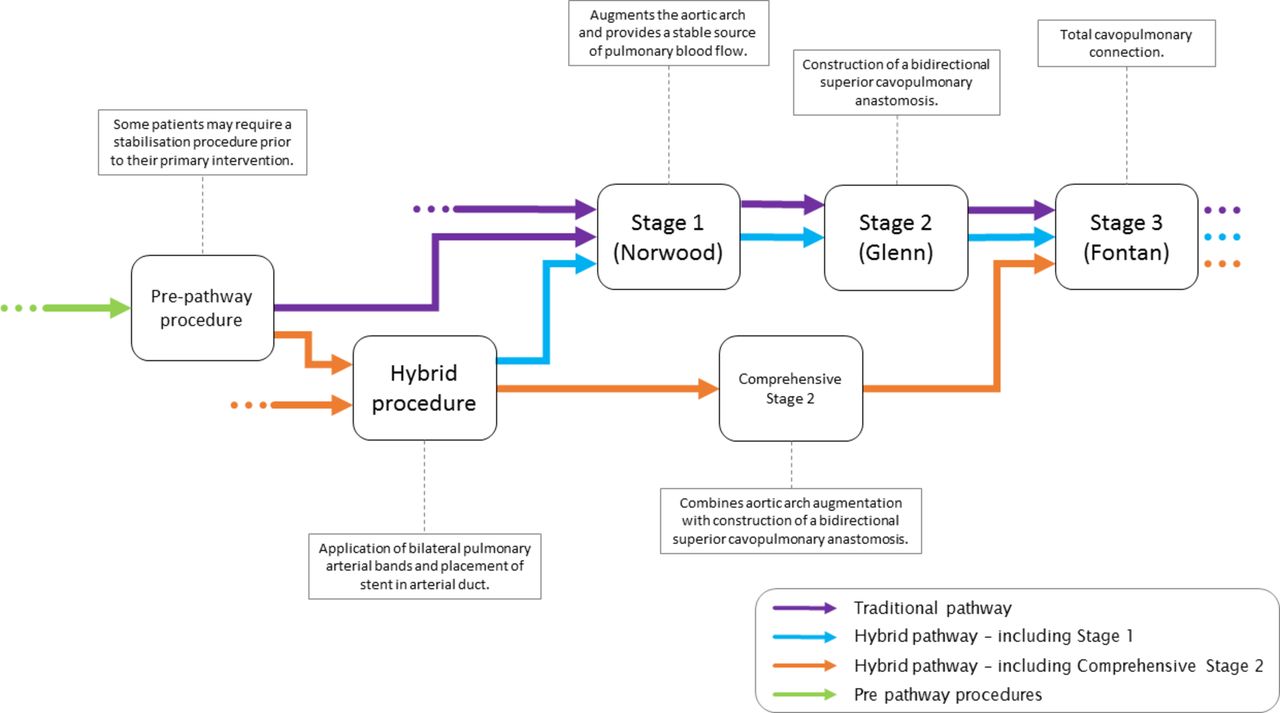
The possible treatment pathways for patients born with hypoplastic left heart syndrome (HLHS) in the UK.
Numerous reports document the early surgical outcomes following the stage 1 operation for HLHS,3 4 recognised as among the most technically challenging in paediatric cardiac surgery.5 Interstage deaths between discharge following stage 1 or hybrid procedure and the stage 2 procedure have been a focus of quality assurance efforts.6 7
Studies capturing staged interventions and longer term HLHS outcomes that go beyond single-centre experience are rare but include the prospective multicentre Single Ventricle Reconstruction (SVR) trial which reported in 2016 that of 549 neonates enrolled in the first stage of the trial, 327 (60%) transplant-free survivors between the ages 2 and 4 years subsequently underwent a Fontan-type procedure.8 A propensity score matching paired study of 338 patients over 21 institutions in North America reported survival at 6 years after Norwood stage 1 of 70% and 55% for patients undergoing right ventricle to pulmonary artery conduit and modified Blalock-Taussig shunt, respectively, with 52% having transitioned to stage 3.9 A registry study of patients with a Fontan-type circulation from Australia and New Zealand published in 2014, which contained only 88/1006 with a HLHS diagnosis,10 suggested HLHS had the poorest outcome. A systematic review of long-term outcomes for CHD contained minimal information specific to HLHS in the current era.11
Given the paucity of long-term data for patients with HLHS at population level, we explored this within the mandatory procedure-based registry for the UK, the National Congenital Heart Disease Audit (NCHDA), operational since 2000 and part of the UK National Institute of Cardiovascular Outcomes Research,12 in which all patients with HLHS who have undergone a procedure are represented. In a previous research letter, we published a summary of outcomes for HLHS based on this NCHDA data.13 We now aim to describe the case mix and interventional pathways in more detail and to evaluate risk factors for longer term survival in HLHS.
Methods
Approvals
The study was approved by the NCHDA Research Committee and the National Health Service (NHS) Healthcare Quality Improvement Partnership (Study number 14CONG03). Further ethics committee approval and patient consent were waived.
Data sources and population
The source data for the study consisted of all records of interventional catheter and cardiac surgical procedures in the NCHDA relating to English and Welsh patients between 1 April 2000 and 31 March 2015. Data submission to the NCHDA is mandatory and subject to external data validation. Each procedure record in the NCHDA contains several diagnostic and procedure codes based on the International Paediatric and Congenital Cardiac Code (IPCCC),14 and further demographic and procedure information. NCHDA procedure data quality is excellent as this has historically been the focus. Data quality for non-procedural information has improved and has been high since 2006,15 partly due to greater scrutiny, with centre-specific outcomes published online from 2007.
Case ascertainment, inclusion and exclusion criteria
Patients with HLHS, defined as those with a small left ventricle, left-sided valvar stenosis or atresia, normally related great arteries and no common atrioventricular junction,16 were identified based on IPCCC codes appearing in their records in the NCHDA and their survival ascertained according to the processes detailed in online supplementary appendix 1. Since patients who do not receive any surgical or interventional cardiology procedures are not captured in the NCHDA, these patients do not feature in the analyses.
Classification and timing of procedures
The allowed timings for the components of HLHS treatment pathway were a primary procedure (stage 1 Norwood or hybrid) within 3 months of birth, a stage 2 or comprehensive stage 2 by 1.5 years of age and a stage 3 by 8.5 years of age. These age limits were deliberately broad to include patients with unusual procedural histories.
In addition to identifying procedures inconsistent with HLHS within the case ascertainment process outlined in online supplementary appendix 1, procedures were classified as:
Prepathway procedures such as stabilisation procedures for neonatal HLHS including bilateral pulmonary artery banding17 and enlargement of a restrictive atrial septum18 or the aortic valve or arch in neonates with hypoplastic left ventricle where subsequent events indicate biventricular strategy was unsuccessful.19
Off-pathway procedures that may be required in patients with HLHS, including surgeries and interventional catheterisations.20
Ambiguous procedures for which there was insufficient information.
The NCHDA does not consistently collect all diagnostic catheters, mechanical support procedures and non-cardiovascular operations so such procedure types were not considered in the analyses.
Demographic data and risk factors
Other data available included: gender, ethnicity (NCHDA contains the categories White, Black, Asian, Other or Unknown), socioeconomic status (Index of Multiple Deprivations 2010)21 for English patients, antenatal diagnosis (yes, no, unknown), comorbidities22 and prematurity (birth at gestation less than 37 weeks).
The following additional factors were derived from records corresponding to prepathway and primary procedures: acquired comorbidities,22 increased severity of illness (preprocedural mechanical ventilation, shock or severe acidosis)22 and low weight (less than 2.5 kg).3
Descriptive analysis
From each patient history, a graphical timeline was constructed of the procedures undergone from birth to death or censoring. An array of these timelines was then produced for patients on a traditional and hybrid pathway separately, with timelines arranged from top to bottom in decreasing order of time to death or censoring.
Statistical methods
Given that the data quality in NCHDA is recognised to be poor for non-procedural factors prior to 2006, which coincides with when the hybrid pathway was introduced in the UK,2 23 patients treated before 2006 were analysed as a separate subgroup (‘the early era’). For patients treated between 2006 and 2015 (‘the recent era’), those following a traditional pathway were analysed separately from those following a hybrid pathway. Variables for which data quality was poor are not presented for the early era.
Unadjusted bivariate comparisons of demographics in the recent era between patients embarking on the traditional pathway and on a hybrid pathway were performed using Fisher’s exact test.
The median and IQRs of age at procedure and length of stay in hospital at different stages of treatment were calculated. Competing risks analysis, with interstage death and completing the next stage of treatment as the competing risks, was used to explore differences in the timing of operations and in interstage mortality between eras and between traditional and hybrid pathways.
The frequency and type of off-pathway procedures were determined and compared using negative binomial regression.
Survival analysis was carried out using the Kaplan-Meier approach, with death representing failure. As the primary study objective was to ascertain long-term condition-based outcomes, we do not treat heart transplantation as an end point in our survival analysis.
Univariable and multivariable Cox proportional hazard regression was carried out on demographic and other patient factors for the recent era patients from England. Welsh patients were excluded as deprivation data were not available. Patients were considered ‘at-risk’ from the time of their initial procedure until death or censoring. Patients with missing data on the risk factors were excluded. We carried out sensitivity analysis comparing the univariable Cox model results for two extreme cases of all patients with missing data for a particular risk factor being allocated as having or not having the risk factor in question.
Data were analysed using the Stata statistical software package (Stata Statistical Software: Release 13. College Station, StataCorp, Texas, USA).
Results
The data set
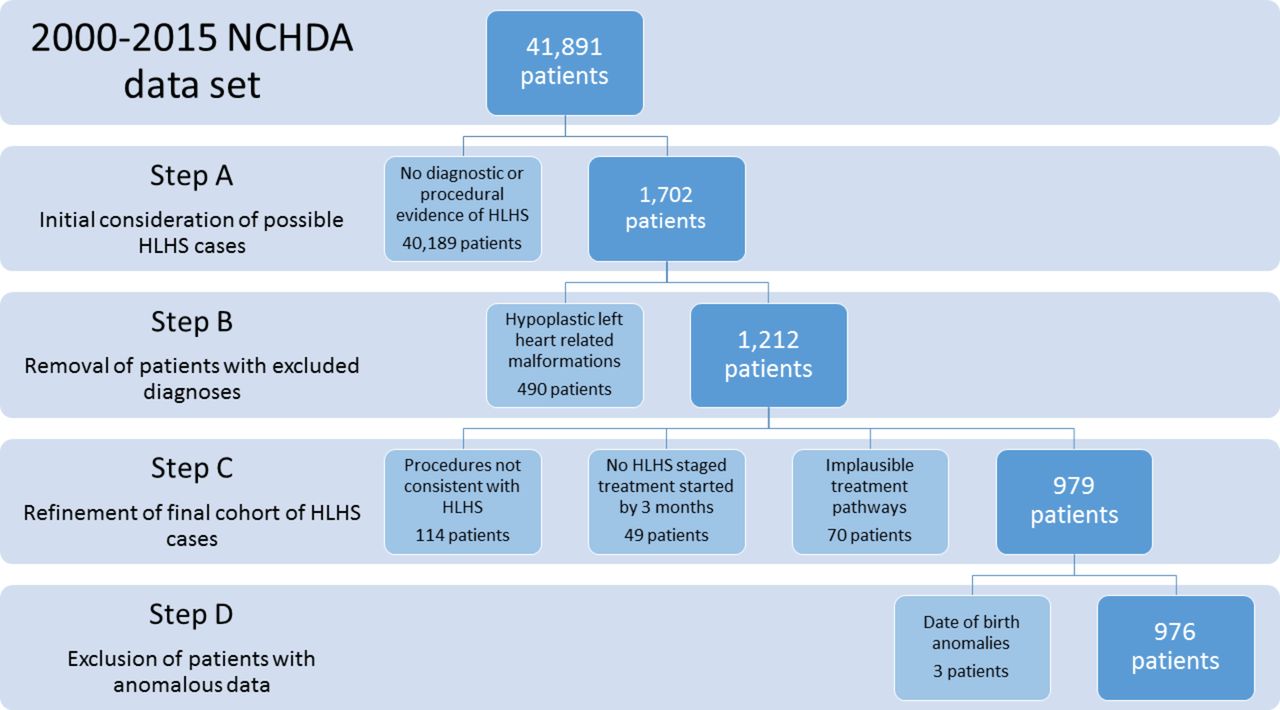
The exclusions that were made from the data set are summarised in figure 2, and resulted in a cohort of 976 patients with HLHS for analysis.

Exclusions made during the case ascertainment process. HLHS, hypoplastic left heart syndrome; NCHDA, National Congenital Heart Disease Audit.
Demographics and time eras
There were 296 patients commencing treatment in the early era, including 14 patients undergoing prepathway interventions, eight of whom survived to stage 1.
In the recent era, 584 patients started a traditional pathway and 62 patients a hybrid pathway. A total of 80 recent era patients underwent prepathway interventions, 46 of whom continued to primary procedure (45 embarking on the traditional pathway and 1 embarking on the hybrid pathway). The 34 patients who did not reach their primary procedure are included with the dominant traditional pathway cohort for analysis purposes.
Patient characteristics are summarised in table 1.
Characteristics of patients with HLHS commencing interventions in the early era and for patients commencing the traditional and hybrid pathways in the recent era
The patients following a hybrid pathway were more complex than those following a traditional pathway, with a higher incidence of patients with congenital comorbidities, prematurity or low weight or acquired comorbidities prior to or at their primary procedure.
Interventional treatment pathways
Figure 3 shows the array of timelines of treatment for traditional and hybrid pathway patients. One notable feature is the variability in the ages at which stage 3 procedures were undertaken.

Treatment and outcome timeline for traditional pathway patients (n=914) and hybrid pathway patients (n=62). Each dark blue line represents a patient, with different markers for the interventions and events during their treatment. Hybrid; stage 1; stage 2 (or comprehensive stage 2) and stage 3 are shown with pink, orange, purple and green, respectively. Heart transplants undertaken are shown in yellow, and any off-pathway procedures are shown in blue. A patient’s ‘known lifespan’ line ends either at censoring alive or death, with deaths shown in red. As there are many traditional pathway patients than hybrid pathway patients, each individual patient timeline cannot be discerned for traditional pathway patients.
Table 2 gives the frequencies of prepathway and pathway procedures, summaries of the age and weight at which the procedure occurred; the hospital length of stay, in-hospital mortality and interstage mortality. The highest in-hospital mortality rates followed the prepathway procedures for both eras, followed by the mortality rates linked to stage 1 surgery in the early era and then hybrid procedures in the recent era. Statistically significant differences between eras are highlighted in table 2.
Frequencies, timings, weights, in-hospital and interstage outcomes for staged treatment of HLHS
Prepathway procedures
Prepathway procedures, which had the highest mortality, were undertaken in 94 more complex patients who had a higher incidence of acquired comorbidity (P=0.021), severity of illness indicator (P<0.001) and prematurity (P=0.043) in the recent era. Components of prepathway procedures included: 58 to create or enlarge the interatrial communication (surgery or catheter), 40 to place bilateral pulmonary arterial bands, 4 surgeries to relieve obstructed pulmonary veins and 15 other miscellaneous or incompletely coded procedures. There were also 21 operations to relieve obstruction to the aortic arch, 15 transcatheter balloon dilations of the aortic valve and 4 neoaortic valvoplasty procedures representing neonates where an initial (failed) attempt had been made to create a biventricular circulation.
Off-pathway procedures
The frequencies of each off-pathway procedure type are included in online supplementary appendix 2, the most common being revision of the arterial shunt or right ventricle to pulmonary artery valveless conduit (Sano) and stenting or dilation of residual or recoarctation. 44.6% had a subsequent off-pathway procedure following their primary procedure; rates are shown in table 3. Table 3 shows the rates of off-pathway procedures split for the early, recent era traditional and hybrid pathway patients, and by stage of treatment. The rates were generally higher for the recent era cohort, particularly hybrid patients. Negative binomial regression showed that the increase in the rate of off-pathway procedures between the early and recent eras was statistically significant between stages 1 and 2 (P<0.001), most notably driven by interventional catheterisations in the hybrid cohort, and poststage 3 (P=0.030).
The rate of off-pathway procedures occurring at different stages of the treatment pathway for HLHS by era
Survival analysis
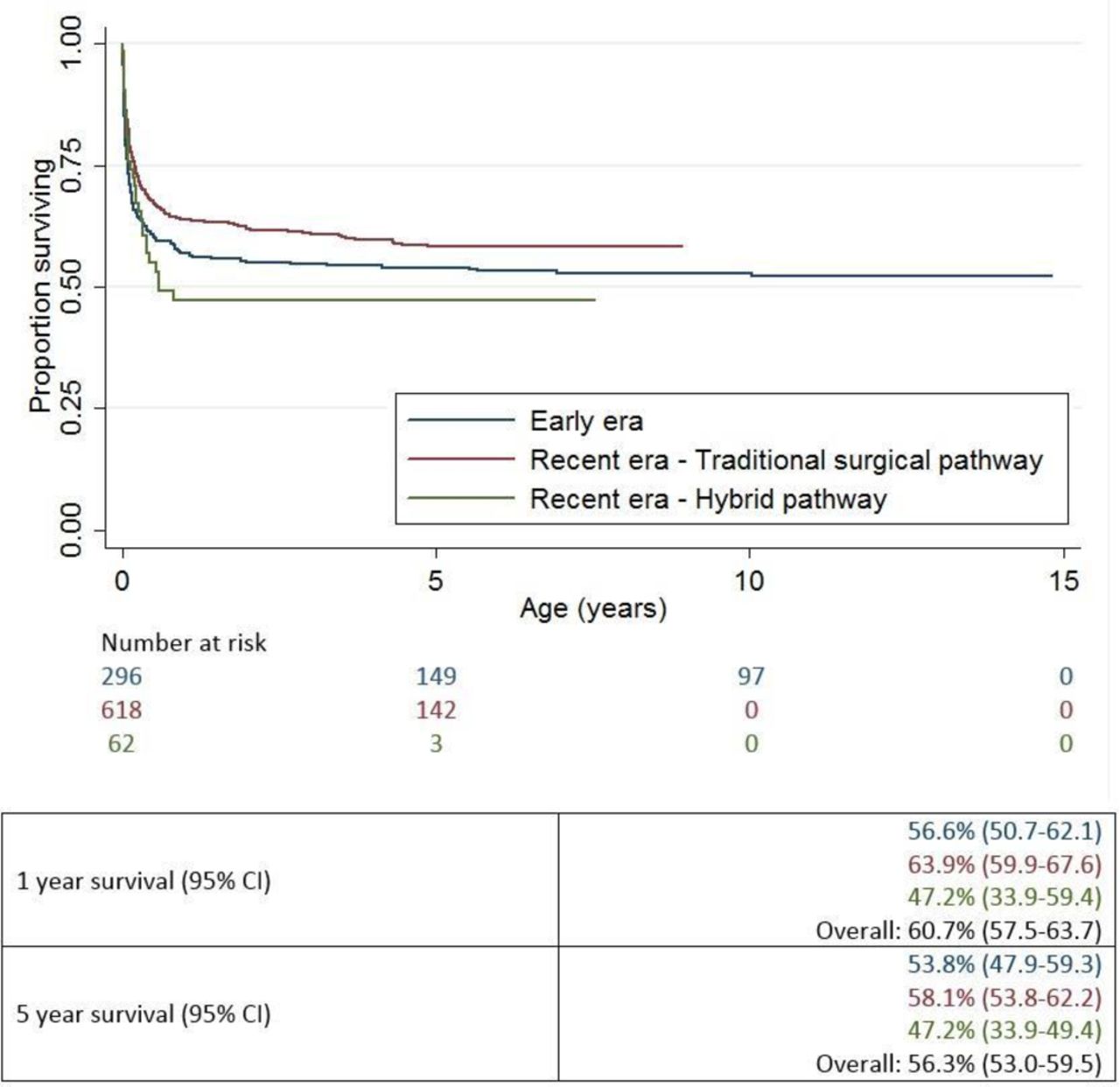
Figure 4 shows Kaplan-Meier survival curves by era and by pathway for the recent era, inclusive of prepathway deaths in the traditional cohort. The 1-year and 5-year survival in the early era was 56.6% (95% CI 50.7% to 62.1%) and 53.8% (95% CI 47.9% to 59.3%), respectively. For the recent era, the 1-year and 5-year survival rates were 63.9% (95% CI 59.9% to 67.6%) and 58.1% (95% CI 53.8% to 62.2%) for the traditional patients versus 47.2% (95% CI 33.9% to 59.4%) and 47.2% (95% CI 33.9% to 49.4%) for the hybrid patients. A cox proportional hazards model, presented in table 4, showed that patients with antenatal diagnosis, a low weight or acquired comorbidity prior to primary intervention were all less likely to survive. The Cox model showed no evidence that the proportional hazards assumption had been violated (P=0.869). For traditional pathway patients in the recent era, whether the stage 1 procedure was performed before or after 1 month of age did not have an effect on subsequent survival (P=0.875).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival plot and 1-year and 5-year actuarial survival displaying separately: patients commencing treatment in the early era (n=296), in the recent era on the traditional surgical pathway (n=618) and the hybrid pathway (n=62).
Univariable and multivariable HRs for recent era patients (n=599)
Sensitivity analysis
If all patients with missing ethnicity data were assumed to be non-white, non-white patients had a significantly increased HR (P=0.021) compared with white patients, and if all patients’ missing data on antenatal diagnosis were assumed to have not had an antenatal diagnosis, antenatal diagnosis ceased to significantly increase the HR (P=0.124). Other comparisons of patients with missing data for ethnicity, sex and antenatal diagnosis did not change the univariable results shown in table 2.
Discussion
This longitudinal analysis on procedure-based registry data offers a unique insight into the journey faced by patients with a complex disease like HLHS in terms of interventions and mortality across anticipated staged and unanticipated prepathway or off-pathway interventions during infancy and childhood. The variations to the standard treatment pathway for HLHS, and the outcomes, are made available to inform counselling of families, particularly considering that the vast majority of cases are currently prenatally diagnosed. This provides a more valid perspective than reliance on data from procedure-based data sets.
The variation in treatment is shown by the 9.6% of patients who had a prepathway procedure. Such prepathway interventions are required for the highest risk neonates17 and over a third did not survive to a primary procedure. The use of the hybrid procedure was infrequent at 6.4% (in 2015, North American Centres represented within the Society of Thoracic Surgeons Congenital Heart Surgery Database reported that 13% of primary procedures for HLHS were hybrids)24 and reserved for the smallest and most complex patients, who had poorer outcomes. Among patients in the whole cohort, only 1.8% underwent a transplant, this occurring at various stages in the treatment pathway, but notably, because of low donor organ availability in the UK, no patient had transplantation as their primary intervention, an approach reported from North America.25
Although in-hospital mortality following the stage 1 operation improved in the recent era and the age at which stage 2 was undertaken fell (this has previously been reported in UK26 and USA data7), mortality rates across later stages in the journey were unchanged. As has been reported in other cohorts,27 there was significant interstage mortality between stages 1 and 2. Previous focus on this interstage period has enabled the evaluation of therapeutic interventions to reduce mortality, including additional surveillance of patients in home monitoring programmes.6 Furthermore, non-randomised studies of digoxin use between stages 1 and 2 indicate this is linked to reduced mortality.28 Our study data identified further interstage deaths between stages 2 and 3, a less well-explored phase of the patient journey for HLHS. This interstage mortality and the variability in age at stage 3 suggest that these phases may be future targets for quality improvement. In this regard, we note that the median stage 3 age in the recent era was 4 years compared with 2.8 years reported in the SVR trial.8
Previous population-based studies of HLHS have predominantly reported outcomes at 1 year of age,29 or are focused on even shorter time periods,25 whereas our study includes a median follow-up time in survivors of 5 years and 2 months. Our survival analyses suggested that although among patients on the traditional pathway there was improved survival in the later era, this was accompanied by the evolution of complex cohort of hybrid patients with poorer outcomes. One explanation to note for the modest progress in overall survival across the HLHS population is the reported trend in the UK towards acceptance of more complex candidates for surgery.26
The high rate of antenatal diagnosis for HLHS in this study (81% in the recent era) indicates excellent performance of obstetric sonographers screening for this disease. Although it is unsurprising that patients who were smaller and sicker at primary intervention had poorer outcome, some readers may be surprised that those with antenatal diagnosis also did worse, even after adjustment for size and comorbidities. This supports a previously stated hypothesis that antenatally diagnosed patients are more likely to display higher risk disease subtypes,30 which in HLHS specifically includes worse forms of HLHS anatomy that are not consistently collected within NCHDA (eg, tricuspid valve regurgitation). The small but significant relationship between non-white ethnicity and poorer outcomes, and the complex relationship between deprivation and outcomes require further work to fully explore the interactions between socioeconomic factors and survival for patients with HLHS.
How do these outcomes compare with other data?
The overall in-hospital mortality rates reported for our study cohort (stage 1, 22.7%; stage 2, 3.6%; stage 3, 1.2%) compare well with other studies.3 10 20 31 Considering survival rates for HLHS beyond 1 year, outcomes of our study cohort cannot be directly compared with the results of the Wilder et al’s study9 of outcomes for neonates undergoing stage 1 Norwood from 21 North American institutions between 2005 and 2014, because of the large number of exclusions in that study. Among 692 consecutive neonates meeting the diagnostic criteria for inclusion, 454 underwent a traditional pathway but reported outcomes are only available for the 339 included in the propensity- matched paired analysis. The SVR trial included 549 patients with HLHS who underwent a Norwood-type operation at 15 North American sites between 2005 and 2008 and excluded patients with major congenital or acquired abnormalities likely to affect survival.3 The SVR trial reported 32.2% of patients were deceased at 3 years (and 20 survivors transplanted).20 After removal of the patients undergoing only prepathway intervention, the 3-year mortality in the recent era cohort of traditional pathway patients in our study was very similar at 36.0%, noting that in contrast to SVR our cohort did include patients with additional congenital anomalies and moreover was population based.
The increase in the rate of off-pathway interventions between the early and recent eras in our study suggests that the approach to interstage interventions has become more proactive. Increased patient complexity due to improved early survival and an emerging complex hybrid population could contribute to this. Nonetheless, the rate of off-pathway procedures is lower than the rate reported in the 3-year follow-up of the SVR trial in which 164.3 cardiac surgeries and 43.1 catheter interventions per 100 patient-years from Norwood to 3 years are documented,20 although the cohorts and time periods considered are not directly comparable.
Study limitations
As with any registry-based study, the retrospective analysis of an observational data set holds inherent limitations and is limited by data quality. Of particular note, there are two variants of the stage 1 procedure (the classic Norwood where pulmonary blood flow is either provided by a Blalock-Taussig shunt or a right ventricle to pulmonary artery valveless conduit (Japanese (or Sano) modification)).3 20 27 Previous studies have shown significant differences in outcomes for patients undergoing the two variants.3 9 Regrettably within the NCHDA, the vast majority of stage 1 surgeries (86.0%) do not include sufficient information to determine which of these two types of operation was performed. We took an inclusive approach within this registry-based study and included all patients where the diagnosis was HLHS, irrespective of reasonable variations in the timing of procedures or where unusual additional procedures were undertaken; since this represented our best assessment of the true picture of events for patients with HLHS. As stated, only patients who underwent at least one procedure are captured within the source data.
Summary and future directions
Based on review of published HLHS outcomes, we note that current outcomes for intervened HLHS in England and Wales are well up to international standards. The analyses of ‘longer-term outcomes based on diagnosis’ for patients with complex CHD are inherently complicated, given the range and complexity of possible treatment pathways that a patient follows, and the difficulty in determining a pure population.
Nonetheless, it is essential to take the analyses of outcomes, in particular for higher risk conditions, such as HLHS, that require serial interventions, in this direction in order to provide a fuller picture and to inform quality assurance and improvement efforts.
Key messages
What is already known on this subject?
Hypoplastic left heart syndrome (HLHS) represents one of the most complex and high-risk forms of congenital heart disease.
Treatment options have evolved dramatically in the last 30 years.
Data reporting longer term outcomes reflecting current practice are scarce.
What might this study add?
We have undertaken the first analysis of UK national audit data on procedures to report longer term patient-based outcomes for HLHS.
Interventional treatment pathways followed for HLHS are complex and highly variable.
56.3% of patients survived to age 5 years and nearly half of patients had an additional unplanned intervention.
How might this impact on clinical practice?
The information presented on longer term outcomes may in future be used to inform families during decision-making for their child.
It is essential that the long-term outcomes of conditions like HLHS that require serial interventions are used for audit to provide a fuller picture and to inform quality assurance and improvement.
Acknowledgments
The authors thank the data managers and audit leads at the UK centres that contribute to the national audit data for their hard work in this regard, and finally the authors thank the data management team at NICOR for their major contribution to the NCHDA and providing the data for this study.
In particular, the authors dedicate this paper to David Cunningham, who nurtured the NCHDA database since its beginning as senior data manager at NICOR and who sadly passed away in December 2017.
References
Footnotes
Contributors KLB conceived the study. KLB, CP and MU designed and led the study. LR carried out the data analysis and wrote the first draft of the paper. RCF, IDS, MM, VT and CB provided clinical input and advice. All authors read and commented on the manuscript.
Funding This project was funded by the Great Ormond Street Children’s Charity (v1248). MU was in part supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care North Thames at Bart’s Health NHS Trust. KLB, IDS, MM and VT were supported by the NIHR Research Biomedical Research Center at Great Ormond Street Hospital for Children NHS Foundation Trust and University College London.
Competing interests KLB and RCF sit on the steering committee of NCHDA.
Ethics approval The study was approved by the NCHDA Research Committee and the National Health Service (NHS) Healthcare Quality Improvement Partnership (study number 14CONG03).
Provenance and peer review Not commissioned; externally peer reviewed.