Article Text

Abstract
Objectives We aimed to analyse outcomes of ticagrelor and clopidogrel stratified by estimated glomerular filtration rate (eGFR) in a large unselected cohort of patients with acute myocardial infarction (MI).
Methods We used follow-up data in MI survivors discharged on ticagrelor or clopidogrel enrolled in the Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies registry. The association between ticagrelor versus clopidogrel and the primary composite outcome of death, MI or stroke and the secondary outcome rehospitalisation with bleeding diagnosis at 1 year, was studied using adjusted Cox proportional hazards models, stratifying after eGFR levels.
Results In total, 45 206 patients with MI discharged on clopidogrel (n=33 472) or ticagrelor (n=11 734) were included. The unadjusted 1-year event rate for the composite endpoint of death, MI or stroke was 7.0%, 18.0% and 48.0% for ticagrelor treatment and 11.0%, 33.0% and 64.0% for clopidogrel treatment in patients with eGFR>60 (n=33 668), eGFR30–60 (n=9803) and eGFR<30 (n=1735), respectively. After adjustment, ticagrelor as compared with clopidogrel was associated with a lower 1-year risk of the composite outcome (eGFR>60: HR 0.87, 95% CI 0.76 to 99, eGFR30–60: 0.82 (0.70 to 0.97), eGFR<30: 0.95 (0.69 to 1.29), P for interaction=0.55) and a higher risk of bleeding (eGFR>60: HR 1.10, 95% CI 0.90 to 1.35, eGFR30–60: 1.13 (0.84 to 1.51), eGFR<30: 1.79 (1.00 to 3.21), P for interaction=0.30) across the eGFR strata.
Conclusions Treatment with ticagrelor as compared with clopidogrel in patients with MI was associated with lower risk for the composite of death, MI or stroke and a higher bleeding risk across all strata of eGFR. Of caution, bleeding events were more abundant in patients with eGFR<30.
- acute myocardial infarction
- coronary artery disease
- acute coronary syndromes
- epidemiology
Statistics from Altmetric.com
Introduction
Chronic kidney disease (CKD) is present in 30%–40% of patients presenting with myocardial infarction (MI),1–4 and is associated with an increased risk of recurrent MI, all-cause and cardiovascular (CV) death, as well as bleeding complications.3 5–7
In the PLATelet inhibition and patient outcomes (PLATO) trial,8 comparing ticagrelor and clopidogrel in patients with acute coronary syndrome, CKD defined as creatinine clearance (CrCl) below 60 mL/min was one of the enrichment criteria for inclusion. Overall, ticagrelor significantly reduced the incidence of the primary endpoint (CV death, non-fatal MI or non-fatal stroke).8 In the subgroup of patients with available serum creatinine on admission (n=15 202), ticagrelor resulted in a greater risk reduction of the primary endpoint in patients with reduced CrCl compared with patients with normal renal function (CrCl>60 mL/min) (HR 0.77, 95% CI 0.65 to 0.90 vs HR 0.90, 95% CI 0.79 to 1.02), but with no significant interaction. Even though CKD was associated with an overall higher bleeding risk in PLATO, patients with CKD treated with ticagrelor did not have a higher relative risk of major bleeds as compared with patients with non-CKD.9 However, the generalisability may be limited as CKD was defined as CrCl<60 mL/min and patients in the lower range of CrCl were few and patients on kidney replacement therapy were excluded. Furthermore, subgroup analyses should also be interpreted with caution since positive drug effects are prone to be over-reported and adverse effects under-reported.10 Postapproval studies in real-world settings therefore provide important complementary data to randomised clinical trials.
We aimed to compare ticagrelor with clopidogrel and their association with outcome stratified by renal function in a national cohort of unselected patients with MI using the Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies (SWEDEHEART) registry.4
Methods
Patient population
All patients with MI in the SWEDEHEART registry were identified. This national registry includes all consecutive patients admitted to a coronary care unit or other specialised facility with symptoms suggestive of MI. The SWEDEHEART registry contains data on more than 100 variables such as baseline characteristics, medication on admission, in-hospital therapies, complications and medication at discharge. Continuous monitoring evaluates the correctness of data entered in the registry with the medical records yearly (agreement is about 96%).4 All consecutive patients older than 18 years diagnosed with non-ST-elevation MI (NSTEMI) or ST-elevation MI (STEMI) who were treated and discharged alive with dual antiplatelet therapy (DAPT) with aspirin and clopidogrel or ticagrelor, between 1 January 2010 and 31 December 2013 were selected. For patients with multiple hospital stays for MI, only the first admission was included. We excluded all patients who were on anticoagulant therapy at discharge (n=6912), patients with missing creatinine measurements (n=4744) and patients revascularised with coronary artery bypass grafting (n=3423) during the index hospitalisation resulting in a study population of 45 206 patients. To evaluate percutaneous coronary intervention (PCI)-related in-hospital bleeding, we included a subset of patients (n=36 392) who were enrolled during the same period for cardiac biomarker-verified acute MI (International Classification of Diseases (ICD) code I21), aged ≥18 years, had PCI during the admission and received DAPT with aspirin and either clopidogrel or ticagrelor prior to or during PCI, excluding previous admissions for MI during the study period and patients on oral anticoagulation.
The SWEDEHEART database was merged with data from the National Patient Registry, which includes discharge diagnoses of all hospital stays in Sweden since 1987 and the Swedish Population Registry, providing data on vital status for all Swedish residents. Patients enrolled in national clinical quality registries are informed and can opt out but informed consent is not requested.
We compared the DAPT with either clopidogrel or ticagrelor in addition to aspirin at discharge following the index MI hospitalisation event in an intention-to-treat-like approach. The duration of different DAPT regimens was not available in this study, but current Swedish guidelines recommend 12 months’ duration for most patients.
Outcome definitions
The primary outcome of this study was the composite outcome of time to death, readmission due to stroke or MI at 1 year (see online supplementary material for definitions) for ICD codes. Whichever event occurred first from the time of hospital discharge defined the combined outcome. Secondary outcomes included the individual components of the primary outcome described separately as well as readmission with bleeding (see online supplementary material for definitions). In the case of MI, we applied an initial 28-day grace period during which no events were counted. This approach was taken as index MI events may otherwise be counted as an MI event in patients who are transferred between hospitals and departments during the index admission.11 12 In addition, patients with MI treated with PCI were evaluated for the secondary endpoint of PCI-related in-hospital bleeding. This event was defined by any of the following complications being documented in SWEDEHEART: puncture site haematoma, pseudoaneurysm or bleeding leading to either prolonged compression, blood transfusion, surgery or a drop in haemoglobin.
Supplemental material
Kidney function strata
Estimated glomerular filtration rate (eGFR) was calculated from creatinine measurements on admission recorded in SWEDEHEART and using the Chronic Kidney Disease Epidemiology Collaboration equation.13 Information on ethnicity was not available and not corrected for in the equation. The following categorisation of eGFR was used: eGFR (mL/min/1.73 m2) higher or equal to 60 (eGFR≥ 60), eGFR ≥30 but <60 (eGFR30–60) and eGFR 30 (eGFR<30).
Statistical analysis
Continuous data were expressed by median and IQR and categorical data as numbers and percentages. The Kaplan-Meier method was used to describe unadjusted cumulative survival rates. Cox proportional hazard models were used to evaluate the association between DAPT regimens and outcome after adjusting for prespecified clinical relevant comorbidity and demographic variables. The assumptions of proportional hazards were tested graphically. The association between DAPT with aspirin and ticagrelor or clopidogrel and clinical outcomes were expressed by HRs derived from univariable and multivariable analyses. The multivariable analyses included the covariates ticagrelor treatment, sex, age, history of diabetes, hypertension, MI, congestive heart failure, peripheral vascular disease, ischaemic stroke, chronic obstructive pulmonary disease, cancer within the last 3 years, bleeding, calendar year, Killip class on admission >1, type of MI (STEMI vs NSTEMI), PCI during admission and drugs at discharge including β-blockers, ACE inhibitors or angiotensin receptor blockers and statins. Hospital was used as a random effect. As sensitivity analyses, we also performed the analyses censoring patients according to the intended treatment duration at discharge, analyses restricted to the time period 2012–2013 (excluding the year of 2011 when ticagrelor prescription was low), adjusting for data on stent type (older and newer generation drug-eluting stents vs bare metal stents (see online supplementary material for stent definitions) and after propensity score matching.
Logistic regression was used to study the secondary outcome of in-hospital bleeds related to PCI treatment. Clinically relevant covariates were antiplatelet treatment with ticagrelor, calendar year, sex, age, history of diabetes, hypertension, MI, congestive heart failure, peripheral vascular disease, ischaemic stroke, chronic obstructive pulmonary disease, cancer within the last 3 years, bleeding, Killip class on admission >1, type of MI (STEMI vs NSTEMI), concomitant use of unfractionated heparin, IIb/IIIa inhibitor, radial versus femoral access and use of vascular closure device, drugs at discharge including β-blockers, ACE inhibitors or angiotensin receptor blockers and statins. Hospital was used as a random effect. Significance level was set at P<0.05.
No multiple imputation was performed as complete cases constituted 96.5%. Statistical analyses were performed using R (R V.3.3 with package coxme V.2.2–5).
Results
Patient population and dual antiplatelet treatment regimens
A total of 45 206 patients with MI from 1 January 2010 to 31 December 2013 were included in the study population (ticagrelor: 11 734 patients (26.0%) and clopidogrel: 33 472 patients (74.0%)). The median and the IQR of the intended treatment duration at discharge was 365 days (186–365) for clopidogrel and 365 days (365–365) for ticagrelor. The overall ticagrelor use increased during the study period in all eGFR groups, from the first calendar year to the last: from 0% to 59.8%, 60.8% and 39.5% in patients with eGFR>60, eGFR30–60 and eGFR<30, respectively (online supplementary efigure 1).
Supplemental material
Background characteristics and in-hospital treatments
In all eGFR groups, ticagrelor-treated patients were younger, more likely to be male, more often diagnosed with STEMI and less likely to have suffered previous MI than clopidogrel-treated patients (table 1).
Baseline characteristics for ticagrelor-treated and clopidogrel-treated patients stratified by estimated glomerular filtration rate (eGFR)
The rate of prior hospital admissions with bleeding episodes was similar between ticagrelor-treated and clopidogrel-treated patients. Ticagrelor-treated patients were more likely to have undergone PCI for their index MI than clopidogrel-treated patients (table 2).
In-hospital course and treatment for ticagrelor-treated and clopidogrel-treated patients stratified by estimated glomerular filtration rate (eGFR)
Composite outcome of death, readmission for MI or stroke at 12 months
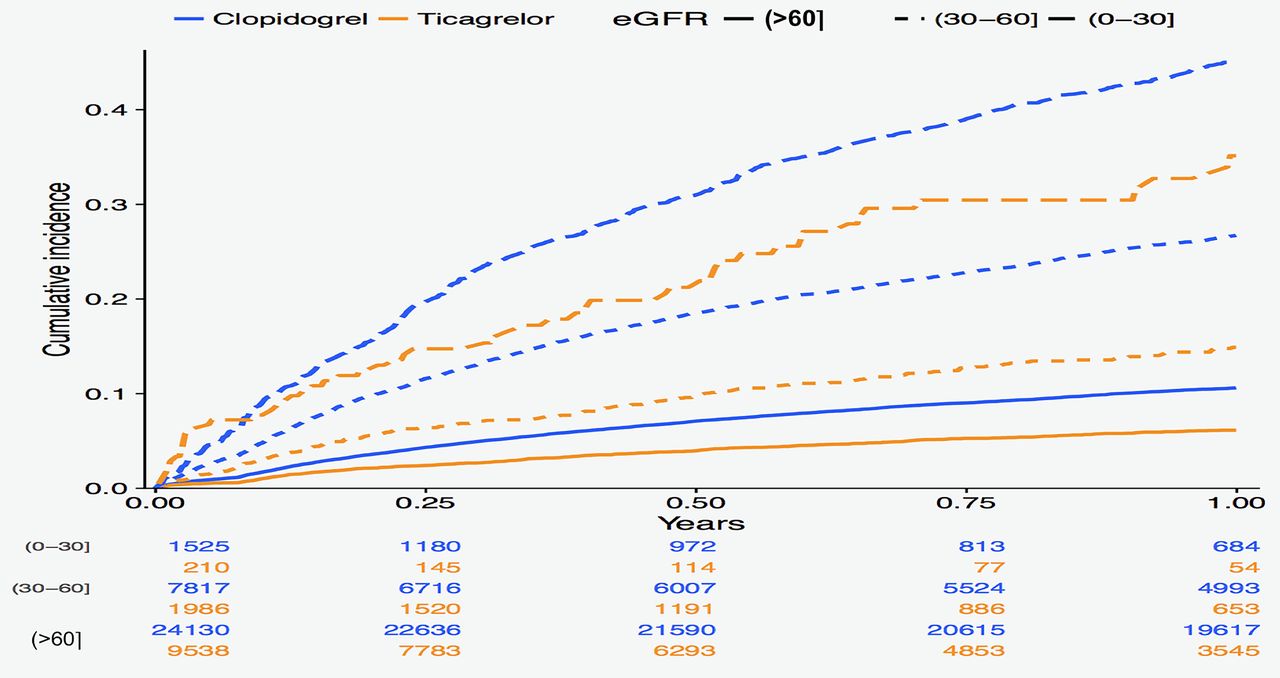
The incidence rate of the combined outcome of death, readmission for MI or stroke at 12 months was higher in patients with CKD (eGFR30–60 and eGFR<30) than in those with normal renal function (eGFR>60) (figure 1, table 3a).

{kind=link}
Cumulative incidence rates for the combined outcomes (death, myocardial infarction or stroke) and numbers at risk stratified on estimated glomerular filtration rate (eGFR) groups in mL/min/1.73 m2.
Even rate and the association between use of ticagrelor as compared with clopidogrel and outcomes stratified by estimated glomerular filtration rate (eGFR)
In the adjusted analyses, ticagrelor as compared with clopidogrel was consistently associated with a significantly lower risk of the combined outcome without significant interaction for subgroups based on eGFR (P for interaction 0.55). In the two upper eGFR strata, eGFR>60 and eGFR30–60, the HRs were 0.87 (95% CI 0.76 to 0.99) and 0.82 (0.70 to 0.97), respectively (figure 1 and table 3a)(figure 2, table 3a). In the group of patients with eGFR<30, the CIs were wide and crossed the line of unity (HR 0.95, (95% CI 0.69 to 1.29)).
- Download figure
- Open in new tab
- Download powerpoint
Forest plot illustrating the adjusted HR (adj HR) and the adjusted OR (*) for different outcomes stratified on estimated glomerular filtration rate (eGFR) groups (mL/min/1,73m2). MI, myocardial infraction.
Separate outcomes of death, readmission for MI or stroke
With lower eGFR strata the rates of death, readmission for MI and stroke were higher (figure 2,3, table 3a)(figure 3, table 3a). The point estimates indicated a lower risk with ticagrelor as compared with clopidogrel in all eGFR strata except in patients with eGFR<30 where all CIs were wide and crossed the line of unity (figure 2). For the secondary outcomes, there were no significant interaction except for renal function and ticagrelor regarding death (P=0.04). Different subtypes of stroke outcomes (haemorrhagic stroke and ischaemic stroke) stratified on eGFR are presented in the (online supplementary table 1).
- Download figure
- Open in new tab
- Download powerpoint
Cumulative incidence rates for the different secondary outcomes and number at risk stratified on estimated glomerular filtration rate (eGFR) groups in mL/min/1.73 m2. MI, readmission with myocardial infarction, bleed, readmission with bleeding.
Bleeding
Ticagrelor was consistently associated with a higher risk of hospitalisation with bleeding and PCI-related bleeds in the different eGFR strata as compared with clopidogrel without a significant interaction between eGFR strata and treatment (figures 2 and 3 and table 3b).
Sensitivity analyses
For the primary outcome, we also performed sensitivity analyses with propensity score matching (see online supplementary table 2a–c), analyses censoring patients according to the intended DAPT duration at discharge (see online supplementary table 3a–c), analyses adjusting for information on coronary stent types (see online supplementary table 4a–c) as well as analyses restricted to the years 2012–2013 (see online supplementary content supplementary table 4d). These analyses resulted in similar results regarding the primary outcome (see online supplementary figures 1 and 2).
Association between use of ticagrelor as compared with clopidogrel and bleeding outcomes stratified by estimated glomerular filtration rate (eGFR)
Discussion
In this large real life, observational study of prospectively enrolled patients with MI treated with ticagrelor or clopidogrel in combination with aspirin, we showed that ticagrelor was associated with a lower risk of death and readmission for MI or stroke, which was consistent across eGFR subgroups. In patients with advanced kidney dysfunction (eGFR<30), we did not observe a significant association between ticagrelor and the primary outcome. However, these patients were few and CIs wide, indicating a low power to detect potential differences between treatment groups, and there was no sign of interaction between kidney function and treatment regarding the primary outcome.
There was a higher risk of in-hospital and out-of-hospital bleeding events in the ticagrelor-treated group. After adjustment, the estimated risk of in-hospital bleeding was 41%–53% higher, regardless of kidney function. Regarding subsequent readmission with bleeding the estimated risk of ticagrelor was statistically significant and appeared higher in patients with eGFR<30, compared with those with eGFR>60 and eGFR30–60. Still, the CIs were wide a there was no significant interaction.
The present study extends the findings of our previous real-life analysis by demonstrating that the balance between lower risk of ischaemia and higher risk of bleeding is beneficial, also in the large subgroup of patients with moderate CKD.14 Our findings support the notion that the proven benefit of ticagrelor shown in PLATO can be applied in a real-world setting.8 9
In PLATO, the benefit of ticagrelor was even more pronounced with a larger absolute risk reduction in patients with CKD (CrCl <60 mL/min) compared with patients with normal renal function (CrCl >60 mL/min).8 9 The relative risk reduction of ticagrelor as compared with clopidogrel for the primary endpoint (CV death, non-fatal MI or non-fatal stroke) was 23% in patients with CKD (HR 0.77; 95% CI 0.65 to 0.90) compared with 10% in patients with normal renal function (0.90; 95% CI 0.79 to 1.02), but this interaction was not statistically significant. Similarly, when ticagrelor was tested against placebo in aspirin-treated patients with stable coronary artery disease, 1–3 years after a MI, in the Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin-Thrombolysis in Myocardial Infarction 54 (PEGASUS-TIMI 54) trial,15 the absolute risk reduction of ticagrelor was larger in patients with CKD than in patients with non-CKD, but there was no difference in relative risk reduction. Several other studies comparing different intensity and duration of antiplatelet therapy have not shown any major differences in the relative treatment effect between patients with and without CKD.16–20 The increased risk of bleeding regardless of kidney function found in the present study, is well in line with results from the PLATO8 and PEGASUS15 trials, although the absolute risks cannot be directly compared due to different definitions of bleeding.
Since CKD is an independent predictor of both thrombotic and bleeding complications, antiplatelet treatment may be challenging in clinical practice. Abnormal platelet interaction, decreased platelet reactivity and increased bleeding risk have been described in patients on kidney replacement therapy,21 but higher platelet reactivity and reduced clopidogrel-induced antiplatelet effects are associated findings in patients with moderate CKD.22–24 However, results from pharmacodynamic studies regarding CKD and the associations of platelet reactivity have not been consistent, in particular when adjusting for comorbidities that are more prevalent in patients with CKD.22 25–27
Conflicting results exist regarding impaired efficacy of clopidogrel on platelet reactivity observed in CKD and the association with adverse outcomes in this group, which has been attributed to confounding, lack of power and heterogeneous definitions of platelet reactivity.25 26 28 29 Also, studies examining the effect of ticagrelor on platelet inhibition in patients with CKD have come to different conclusions.27 30 31 Besides P2Y12-pathway blockage, ticagrelor treatment increases inhibition of adenosine reuptake by erythrocytes and it has been postulated that this effect may improve myocardial reperfusion which may play an important role in patients with CKD.9 32 Our study supports, however, that the overall effect of ticagrelor on clinical events is similar regardless of CKD stage, although our results regarding patients with eGFR<30 do not allow definite conclusions.
The present study has several strengths. By enrolling a large majority of patients in the entire country of Sweden for a defined time period, we were able to include a very large sample with unselected and highly representative patients treated with DAPT in the clinical routine. Compared with PLATO,8 patients were significantly older (median age in patients with eGFR<60 was 80 vs 74 years in PLATO) and with a higher proportion of comorbidities, such as previous heart failure (11.8% vs 5.6%), MI (24.7% vs 20.5%) and stroke (10.3% vs 3.9%). The rate of subsequent cardiac events was also higher, which was most obvious in the clopidogrel-treated group with CKD. The high validity of the SWEDEHEART registry and Swedish inpatient registry is also a strength as well as the fact that virtually none of our patients were lost to follow-up.33
Despite a large sample of a large proportion of patients with moderately reduced GFR (eGFR30–60), the number of patients with eGFR<30 was still small resulting in estimates with wide CIs. For most outcomes, there were no significant interaction between eGFR and ticagrelor treatment, which suggest that the effect of ticagrelor is similar regardless of kidney function. But it should be noted that there was a borderline significant interaction (P=0.04) between eGFR and ticagrelor when considering the secondary outcome of death alone. While a borderline statistically significant interaction test of a secondary outcome variable should be interpreted with great caution, the results may suggest that the balance between reducing ischaemia and increasing bleeding events may be different in the real world in patients with more advanced kidney disease. This, together with a higher risk of readmission because of bleeding in patients with eGFR<30, indicates that more studies are needed in patients with more advanced kidney disease, especially in those on kidney replacement therapy who were excluded from PLATO.8
This study has limitations. Due to the nature of the observational study design residual confounding is a well-known potential source of bias and cannot be excluded even after careful multivariable adjustments. We defined our study population based on treatment at discharge (intention to treat). It is possible that patient’s medications were changed or discontinued after hospital discharge which may have led to some misclassification. eGFR groups were based on a single creatinine level available in SWEDEHEART and spuriously high or low values could potentially lead to misclassification of patients. However, the low numbers of missing creatinine values at baseline (<5%) adds strength to this study. Information about exact dosage of other medications was not available and we did not take into account differences in DAPT duration. While data on admissions with prior kidney replacement therapy were available, we were unable to discern whether patients were receiving kidney replacement therapy or not at time of inclusion. Under-reporting of data is also a potential limitation to our study as well as registry studies in general. In particular, bleeding events following PCI in our study were obtained from the SWEDEHEART registry where any under-reporting of bleeding complications would have led to a type II error.
In conclusion, ticagrelor was associated with a lower risk of death or rehospitalisation for MI or stroke than clopidogrel in patients with and without CKD, which supports previously shown benefits in the PLATO. Of caution, bleeding events were more abundant in patients with eGFR<30 and there was a borderline interaction between ticagrelor and renal function regarding death, which may indicate that the balance between ischaemia and risk of bleeding may differ in patients with advanced renal failure, warranting further studies in this specific subgroup.
Key messages
What is already known on this subject?
Data from clinical trials demonstrate that ticagrelor as compared with clopidogrel is beneficial regarding ischaemic risk reduction in patients with myocardial infarction (MI) with normal and moderately reduced renal function.
What might this study add?
This study expands on previous findings by providing postapproval real-world data of unselected patients with MI as well as including patients with severely reduced renal function. Treatment with ticagrelor as compared with clopidogrel, was associated with lower risk for the composite of death, MI or stroke (estimated glomerular filtration rate, eGFR>60: HR 0.87 (95% CI 0.76 to 0.99), eGFR30–60: 0.82 (95% CI 0.70 to 0.97), eGFR<30: 0.95 (95% CI 0.69 to 1.29) and a higher risk of bleeding (eGFR>60: HR 1.10 (95% CI 0.90 to 1.35), eGFR30–60: 1.13 (95% CI 0.84 to 1.51), eGFR<30: 1.79 (95% CI 1.00 to 3.21) across the eGFR strata. The balance between ischaemia and risk of bleeding may differ in patients with advanced renal failure, warranting further studies in this specific subgroup.
How might this impact on clinical practice?
This may influence the choice of dual antiplatelet treatment in patients with severely reduced renal function.
Acknowledgments
We are grateful to all SWEDEHEART coworkers who make the SWEDEHEART registry possible.
References
Footnotes
Contributors RE, TJ, AS, HR, SKJ and KS contributed to the design of the article. AS and HR performed data collection and HR conducted statistical analyses. ME, TJ, SKJ, CV, BL, KS, JS, J-JC, AS and RE were responsible for the interpretation of data as well as drafting and critical revision of the article. All authors approved the final version of the article to be published/submitted.
Funding This work was supported by a grant from the Swedish Foundation for Strategic Research. This work was also supported by the Swedish Heart and Lung Foundation and the Stockholm County Council (ALF project).
Competing interests CV received institutional research grants from AstraZeneca and The Medicines Company, lecture and advisory board fees from AstraZeneca, The Medicines Company and Boehringer Ingelheim, lecture fees from Bristol Myers Squibb, Pfizer and CSL Behring, and is on Clinical Endpoint Committees for Pfizer, Bristol Myers Squibb, Philips and AstraZeneca. KS received lecture fees from AstraZeneca, Aspen and St Jude. BL received institutional research grants from AstraZeneca. ME received payment for lectures for Amgen. J-JC received institutional research grants from AstraZeneca. JS received speaker honoraria from Amgen, Baxter, Astellas Pharma, AstraZeneca, MSD and Hospira. SKJ received institutional research Grant, honoraria and consultant/advisory board fee from AstraZeneca; institutional research grant and consultant/advisory board fee from Medtronic; institutional research grants and honoraria from The Medicines Company; consultant/advisory board fees from Janssen, Bayer. TJ: consulting and lecture fees from AstraZeneca, MSD and Aspen.
Patient consent Not required.
Ethics approval Regional Ethics Committee in Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.