Article Text

Abstract
Objectives Differentiation between normal and abnormal features of vascular ageing is crucial, as the latter is associated with adverse outcomes. The normal aortic ageing process is accompanied by gradual luminal dilatation and reduction of vessel compliance. However, the influence of age on longitudinal aortic dimensions and geometry has not been well studied. This study aims to describe the normal evolution of aortic length and shape throughout life.
Methods A total of 210 consecutive patients were prospectively enrolled in this cross-sectional single-centre study. All subjects underwent CT on a third-generation dual-source CT scanner. Morphometric measurements, including measurements of segmental length and tortuosity, were performed on three-dimensional models of the thoracic aorta.
Results The length of the thoracic aorta was significantly related to age (r=0.54) and increased by 59 mm (males) or 66 mm (females) between the ages of 20 and 80 years. Elongation was most pronounced in the proximal descending aorta, which showed an almost 2.5-fold length increase during life. The lengthening of the thoracic aorta was accompanied by a marked change of its geometry: whereas the aortic apex was located between the branch vessels in younger patients, it shifted to a more distalward position in the elderly.
Conclusions The normal ageing process is accompanied by gradual aortic elongation and a notable change of aortic geometry. Part II of this two-part article investigates the hypothesis that excessive elongation could play a role in the occurrence of acute aortic dissection.
- aortic elongation
- vascular aging
- aortic aging
Statistics from Altmetric.com
Introduction
As the Western population grows increasingly older, physicians will more frequently encounter age-related alterations of the vascular system. It is important to distinguish normal from abnormal aspects of vascular ageing, since an accelerated ageing process confers risk for future cardiovascular disease (CVD).1 2 Prominent structural changes of the aorta include thickening of the intimal vessel wall and gradual luminal dilatation.3–7 The increase of aortic diameters has been studied extensively, given the relation of excessive dilatation with severe complications like dissection and rupture.8 In contrast to its circumferential dimensions, the longitudinal dimensions of the aorta and their evolution over time have not been well studied. It is conceivable that the aorta lengthens during life, since a tortuous deformation or even kinking is frequently observed in elderly patients. This theory was investigated by an autopsy study which measured aortic length in post mortem specimens.9 However, in vitro measurements may not represent those in vivo due to postmortem contraction and the loss of autonomous nerve innervation.9 10 Since advanced imaging techniques are required to study the complex three-dimensional (3D) geometry of the aorta, it was not until recently that non-invasive measurements of aortic length became feasible. One imaging study assessed the relation between age and aortic length and concluded that elongation only occurs in the proximal aorta.11 However, this study measured the length of the ascending aorta as the distance between the sinuses of Valsalva and the apex of the aortic arch. Since the morphology of the aortic arch differs between individuals12 and may change with increasing age,13 it is unclear if these findings represent true vessel lengthening. Theoretically, tortuosity and kinking could also result from age-associated changes of thorax configuration (such as spondylosis and increased kyphosis), which may lead to confinement of the aorta in a gradually decreasing intrathoracic volume.14 Using the latest CT scan techniques, the purpose of the current study is to provide an elaborate description of the evolution of longitudinal aortic dimensions and geometry during life.
Materials and methods
Study population
Consecutive adult patients who underwent contrast-enhanced chest CT at the Maastricht University Medical Center between September 2015 and September 2016 were prospectively enrolled in this single-centre cross-sectional study. Patients with suspected or known aortic disease and those who previously underwent cardiothoracic surgery were excluded, as were those with any other condition that might cause distortion of aortic shape (such as previous radiotherapy or pneumothorax). All scans that provided for adequate 3D modelling of the thoracic aorta with automatically detected centerline were studied. Eventually, a total of 210 patients was included. CT examination was performed because of suspicion of pulmonary embolism (50.7%), pneumonia (7.1%), evaluation or follow-up of pulmonary nodules (38.9%) and other (3.3%). Baseline characteristics were drawn from the medical record.
Image acquisition
All CT scans were performed on a third-generation dual-source CT scanner (Somatom Force, Siemens Healthineers, Forchheim, Germany) with 96×0.6 slice collimation at a rotation time of 0.25 s. Indications and protocolling were clustered in vascular (n=111) and oncological (n=99) workflows without dedicated ECG synchronisation of the respective data sets. Tube voltage and tube current were individually and semi-automatically adapted in all examinations (CARE kV, CARE Dose4D, Siemens), depending on patient’s body mass index (BMI). Iopromide (300 mg iodine/mL, Ultravist, Bayer, Berlin, Germany) was used as a contrast medium in all subjects, using an individualised approach (Contrast Dose Management, Certegra, Bayer). Image reconstruction was performed with 1 mm slice thickness and a reconstruction increment of maximal 0.7 mm with soft tissue kernels (Siemens Bv36/Br40), using a raw data-based iterative reconstruction algorithm (ADMIRE, reconstruction strength 3).
Image evaluation
Image evaluation was performed by a single observer with 5 years experience in cardiovascular imaging. A 3D reconstruction of the thoracic aorta with fitted centerline was created automatically using dedicated software (Syngo.via, Siemens). The aorta was then manually divided by the observer into multiple anatomical segments following current guidelines (figure 1A).15–17 The ascending aorta was defined as the part of the aorta between the sinotubular junction (STJ) and the origin of the brachiocephalic trunk. The aortic arch was measured as the distance from the brachiocephalic trunk to the left subclavian artery. The descending aorta was defined as the segment between the left subclavian artery and the diaphragm and subdivided into two parts: a proximal part (from the left subclavian artery to the level of the bifurcation of the pulmonary trunk) and a distal part (from the level of the pulmonary trunk bifurcation to the diaphragm). The length of each segment was measured as the centerline distance between two points. Segment tortuosity was calculated as the ratio of the centerline path length to the direct linear distance between centerline endpoints (figure 1B). The position of the aortic apex (ie, the most cranial position of the centerline) determined the morphology of the aorta. Type I was defined as an aorta in which the apex was located between the branch vessels (ie, in the segment defined as the aortic arch), while in type II aorta the apex was identified at a position distally of the left subclavian artery (figure 1).

The two distinct aortic types. In type I aorta (A), the apex can be appreciated between the branch vessels (as depicted by the grey dot). Type II aorta (B) is characterised by a more distal position of the apex, in the segment defined as the proximal descending aorta. Part A shows the four individual segments in which the thoracic aorta was divided. Part B shows the measurement methods for segment length and tortuosity: the black line marks the centreline length of the ascending aorta, while the dotted line marks the direct linear distance between the sinotubular junction (STJ) and the brachiocephalic trunk. Segment tortuosity was calculated as the ratio between the centreline and the linear line between these anatomical landmarks.
Statistical analysis
Statistical analyses were performed using commercially available software (IBM SPSS Statistics, V.24, Armonk, New York, USA). The distribution of continuous variables was assessed for normality by the Shapiro-Wilk test and assessed visually by inspection of histograms and standardised normal probability (P-P) plots. Continuous baseline characteristics are presented as mean±SD or as median and IQR in the presence of skewness. Categorical variables are expressed as frequency and percentages. Differences between genders were assessed using the independent samples t-test (or Mann-Whitney U test, if deemed appropriate) and Χ2 test for categorical variables. Linear regression tested the relationship between age and aortic length. Model assumptions on normality, linearity and homoscedasticity for multiple regression analysis were checked and variance stabilising measures, such as log transformation and bootstrapping were applied. Check for (curvi)linearity was performed by introducing linear and quadratic terms for the quantitative predictor of age (in years minus the average, to prevent collinearity between the linear and quadratic term).18 Logistic regression analysis was performed to obtain predictors for the two distinct aortic types; P<0.05 was considered to be statistically significant.
Results
Study population
Subject characteristics are summarised in table 1. The study sample comprised more females than males (61% vs 39%, respectively). The median age of the total study sample was 62 years (IQR 52–72, range 23–92) and did not differ between genders. Men were significantly taller and heavier than women and, consequently, had a larger body surface area (BSA). BMI was comparable between genders. Sixty-eight patients were free of any cardiovascular risk factor. The others were marked as smoker (n=82) and/or suffered from hypertension (n=69), hypercholesterolaemia (n=29) or diabetes (n=19). Of the hypertensive subjects, 62 (91%) were treated with antihypertensive medication.
Baseline characteristics of the study population
Aortic length
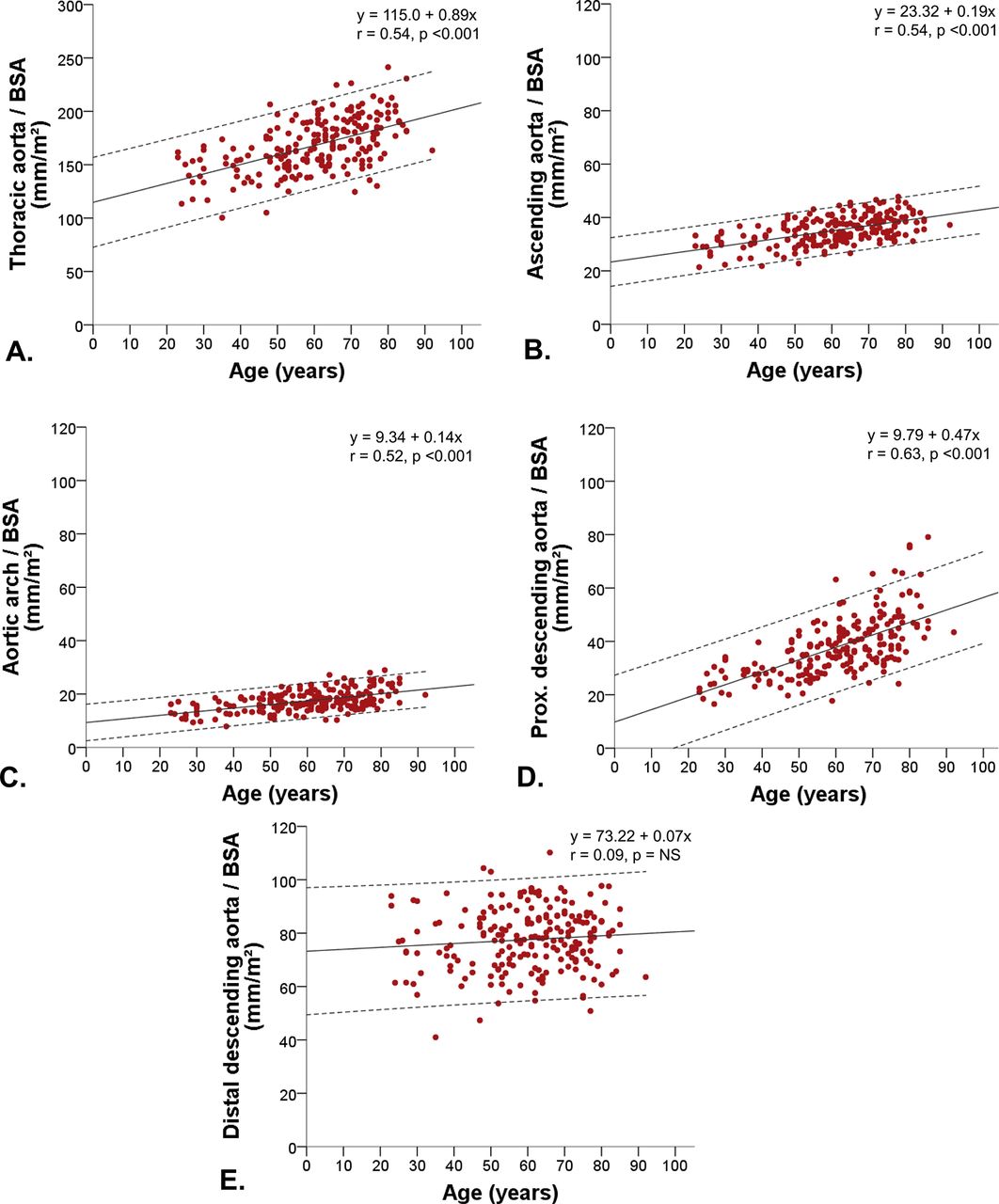
The entire thoracic aorta and all individual segments were, on average, significantly longer in men than in women. However, after adjustment for BSA, none of these differences persisted, indicating the influence of body proportions on aortic length. The BSA-indexed length of the entire thoracic aorta was positively related to age (r=0.54, P<0.001), as were the individual lengths of the ascending aorta (r=0.55, P<0.001) and the aortic arch (r=0.52, P<0.001, figure 2A–C). The length of the descending aorta was also correlated with age (r=0.45, P<0.001). However, this was solely driven by notable lengthening of its proximal part (r=0.63, P<0.001, figure 2D). No relation was found between the length of the distal descending aorta and age (r=0.09, P=0.178, figure 2E). Between the ages of 20 and 80 years, the total length of the thoracic aorta increased by a mean of 59 mm (males) and 66 mm (females), reflecting a relative lifelong growth of approximately 125%. The extent of elongation differed markedly between individual segments: the length of the ascending aorta increased by 142%, compared with 169% (aortic arch) and 247% (proximal descending aorta).
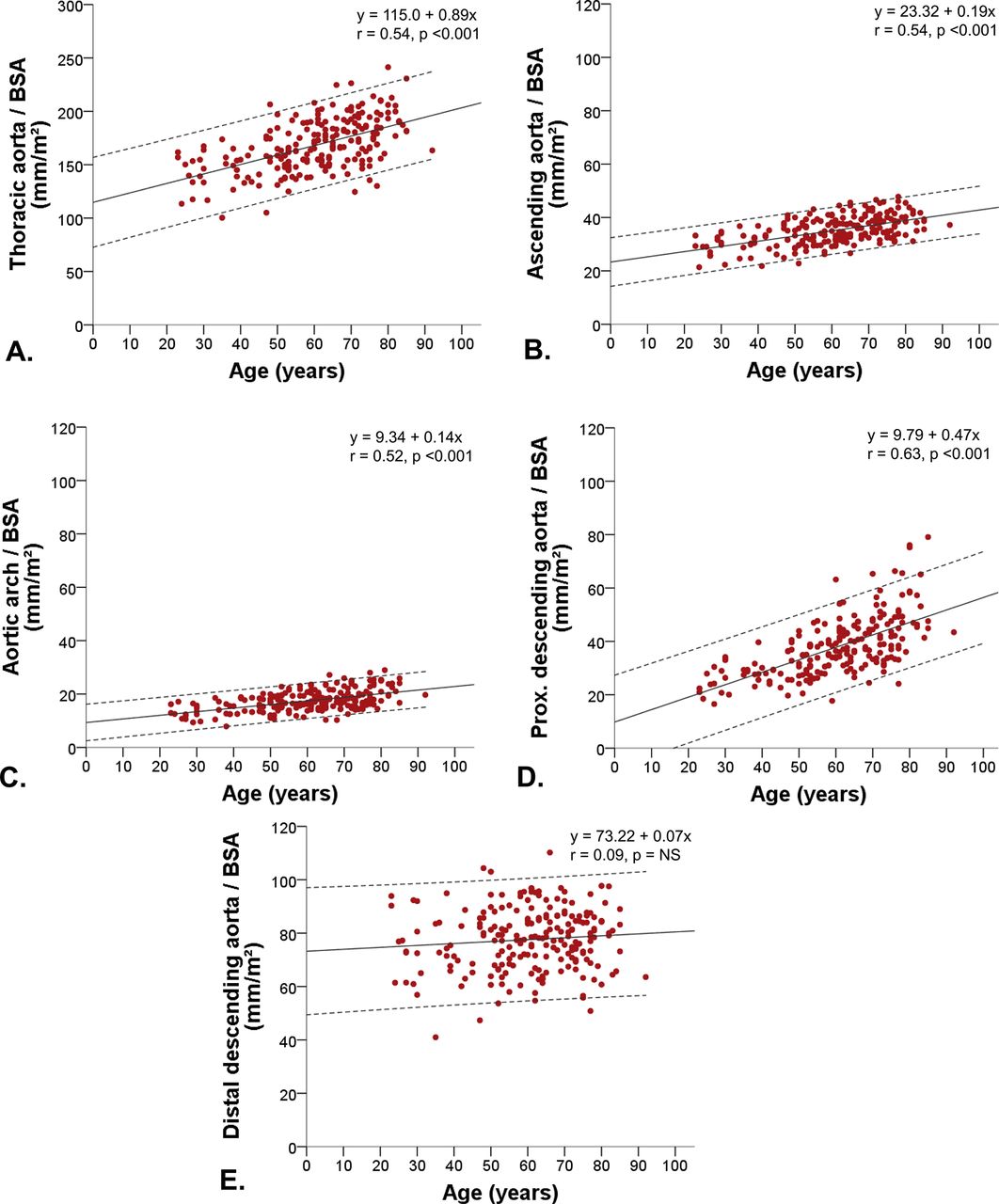
Relation between age and BSA-indexed aortic length. BSA-indexed length of the (A) entire thoracic aorta, (B) ascending aorta, (C) aortic arch, (D) proximal descending aorta and (E) distal descending aorta. The dashed lines mark the 95% prediction intervals. As can be derived from these graphs, elongation is most prominent in the proximal descending aorta. BSA, body surface area; NS, not significant.
Aortic geometry
The tortuosity ratios of the ascending aorta, aortic arch and distal descending aorta were not significantly related to age. The tortuosity of the proximal descending aorta was moderately associated with age (r=0.38, P=0.004) and increased from mean 1.07 (at age 20 years) to 1.21 (at age 80 years).
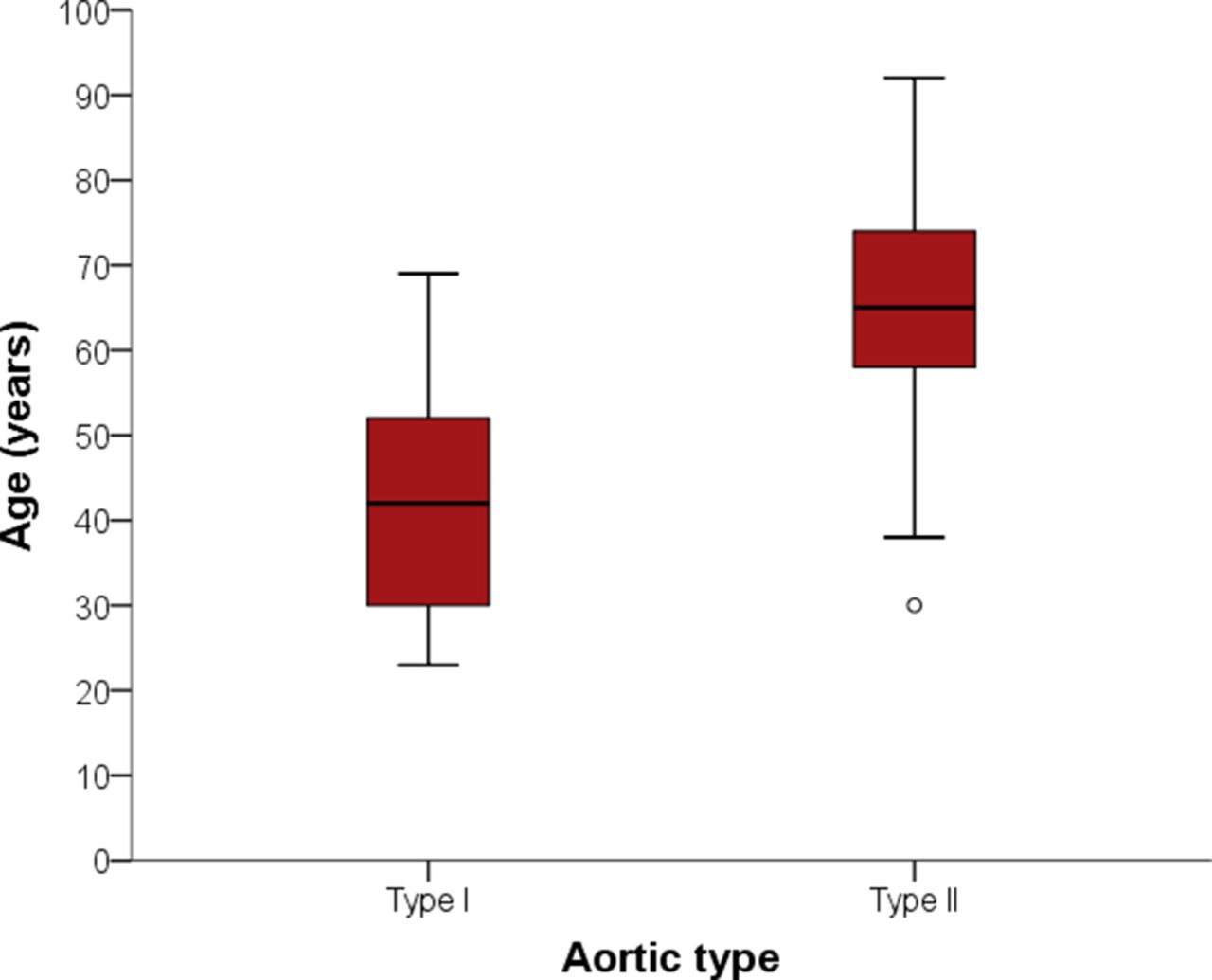
During life, the morphology of the thoracic aorta changed markedly: younger patients exhibited a type I aorta (n=49), whereas a type II aorta was mainly observed in the elderly (n=161, figures 3 and 4). Multivariable logistic regression analysis revealed age, proximal descending aortic length and hypertension to be independent predictors of aortic type (table 2). The morphology of the aorta was not influenced by BSA, gender or cardiovascular risk factors other than hypertension.
Univariable and multivariable logistic regression analysis showing predictors for aortic morphology

The influence of age on aortic type. Box plot showing the age differences between aortic types: type I is more prevalent in younger individuals, while type II aorta is mainly observed in the elderly.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Three-dimensional CT models of the aorta. Three-dimensional modelled CT images of the aorta of a female aged 24 years (A) and a female aged 85 years (B). In part A, a type I aorta is displayed, as the apex of the arch is located between the branch vessels. Part B depicts a type II aorta, as the apex has shifted to a position distally of the left subclavian artery.
Discussion
Premature vascular ageing plays a major role in the development of CVD, as it forms the basis for specific pathophysiological disease mechanisms to act on. An extensive body of literature describes the relation between common features of vascular ageing, such as reduced vessel compliance and luminal dilatation, and the occurrence of cardiovascular events.19–21 Information on aortic length, however, is scarce, since older imaging techniques did not provide for an accurate and 3D visualisation of the thoracic aorta. Using latest CT equipment and acquisition protocols, we have assessed the longitudinal dimensions of the aorta in apparently healthy subjects. By implication, we have shown that it is possible to assess aortic length on routinely acquired CT, even if scans were not specifically acquired for a focused visualisation of the aorta. The main findings of the current study are that: i) the thoracic aorta and its individual segments lengthen with increasing age, ii) the extent of elongation differs between segments and iii) the morphology of the thoracic aorta (aortic type) changes over time. As shown, the ascending aorta only grows modestly during life, while the greatest increase in length is observed in the segment distal to the arch branch vessels. This results in a notable change of aortic morphology. Whereas the younger aorta typically looks like a candy cane (type I aorta), the older aorta unfolds and is more ‘question mark-shaped’ (type II aorta, figure 4). Few previous studies have addressed the age-related alterations of aortic length. Sugawara et al investigated aortic length in healthy volunteers, but concluded that elongation occurs in the ascending aorta only.11 However, their study defined the ascending aorta as the distance between the root and the apex of the aorta. As we have shown, the position of the apex changes during life and, therefore, the measurements by Sugawara et al represent an alteration of aortic morphology rather than lengthening of the tubular ascending aorta. To avoid indistinctness, we would advocate the use of anatomical landmarks in the assessment of aortic length, as supported by current guidelines.15–17 Rylski et al investigated gender-related and age-related differences of aortic diameters and length, which were found to be largest in males.22 BSA-indexed aortic lengths (but not diameters) were comparable between genders and increased in a similar pattern when compared with the current study. We have additionally shown that the geometry of the thoracic aorta changes with increasing age and postulate that these changes could reflect an (un)successful vascular ageing process. Future studies are warranted to investigate the prognostic importance of changes of longitudinal aortic dimensions.
The question arises how our results can be explained from a biomechanical point of view. It has been suggested that aortic elongation is part of a gradual remodelling process as a result of ‘material fatigue’ of the vessel wall.10 11 23 The lifelong exposure to pulsatile strain causes fracture and breakdown of elastin fibres, which results in structural remodelling. Besides elongation and dilatation, this theory explains age-related vascular stiffening, as the reduction of elastin content impairs vessel compliance. Two reasons provide a possible explanation for the differences in elongation between various segments. First, elastin content is highest in the aortic arch and proximal descending aorta.24 25 Following the principles of material fatigue, one would expect these segments to be more prone to remodelling, which is in line with the findings of the current study. Second, the distal descending aorta is fixated to the spine by the intercostal arteries and endures only little longitudinal strain,26 whereas the more proximal aortic segments can move relatively freely in the longitudinal direction. Circumferential strain values, however, are comparable throughout the entire thoracic aorta.26 This provides a plausible explanation for the fact that diameter increase is more prominent than length increase in the distal descending aorta, whereas the opposite applies to the more proximal segments of the thoracic aorta.6
Clinical perspective
Our findings evoke several clinical questions. First, future research could address the clinical implications of aortic elongation. It has been postulated that aortic length plays a role in the occurrence of aortic dissection, which is the result of an imbalance between the biological strength of the aorta and forces exerted on its wall.27 To date, the transverse diameter is the only recognised anatomical risk factor for dissection and the sole marker used in the stratification towards prophylactic aortic surgery. However, luminal diameters are considered to be a poor risk predictor for dissection, as the majority of patients (either presenting with Stanford type A or type B dissection) would not have met the threshold for preventative aortic repair.28–30 In part II of this two-part article, we will investigate the hypothesis that excessive aortic elongation could also play a role in the development of aortic dissection.
Furthermore, our findings should be taken into account in the assessment of arterial stiffness. Pulse wave velocity (PWV) is the velocity at which the arterial pulse propagates through the circulatory system and is the gold standard technique for measurements of arterial stiffness. It is measured as PWV=distance (m)/Δt (transit time in s), in which t is the time delay between the arrival of two waveforms obtained at different anatomical locations (usually at the level of the carotid and femoral arteries). The distance covered by the waves is usually assimilated to the surface distance between the two recording sites. Our results indicate that this technique only provides approximations of the distance travelled by the pulse waves, as vessel length differs between individuals and changes with increasing age. The use of 3D-imaging methods allows for exact distance measurements between two recording sites and, thus, for more precise calculations of PWV.
Study limitations
A few limitations of the current study should be addressed. First, we used a cross-sectional study design, whereas a longitudinal design could be preferred to investigate an ageing process. However, to investigate aortic elongation, one would need to conduct a study with a near lifelong follow-up duration, which carries insuperable constraints for both patient and researcher.
Second, CT examinations were performed for clinical purposes, which implicates that a substantial number of subjects were exposed to cardiovascular risk factors such as hypertension and hyperlipidemia. Our study sample therefore represents a population that is encountered in daily clinical practice, rather than a population of entirely healthy volunteers. As patients aged 50–70 years undergo CT more frequently, these are somewhat over-represented in our study population. The greater variance of aortic length in the elderly should be taken into consideration in the prediction of aortic length.
Third, CT acquisitions were performed without ECG synchronisation. Nevertheless, in none of the included scans did we encounter motion artefacts that could hamper the accuracy of length measurements. With the acquisition parameters as described above, the entire thoracic aorta can be acquired within one rotation of the scanner tube. With rotation times as short as 250 ms, acquisition time only covers a small fraction of the R-R interval, which explains the absence of motion artefacts. Scans acquired with older scanners (and, thus, longer acquisition times) will more likely benefit from ECG synchronisation.
Key messages
What is already known on this subject?
The age-related influence of age on circumferential aortic dimensions has been studied extensively. However, age-associated changes of longitudinal aortic dimensions have not been well-studied, since more advanced imaging methods are required to study the complex three-dimensional geometry of the aorta. It is generally thought that the aorta lengthens with increasing age. An autopsy study measured aortic length, but ex vivo measurements may not represent those in vivo (eg, due to loss of autonomous nerve innervation). No previous non-invasive imaging studies structurally investigated segmental aortic length and the age-related change of aortic geometry.
What might this study add?
This study provides an elaborate description of evolution of longitudinal aortic dimensions throughout life and the subsequent effect on the geometry of the thoracic aorta.
How might this impact on clinical practice?
The current study provides more insight into the normal ageing process of the thoracic aorta. It can thereby increase the understanding of pathophysiological mechanisms in aortic diseases (such as in aortic dissection).
References
Footnotes
Contributors All listed author contributed in the following way to the manuscript. BPA and SH (corresponding author): conceptualisation, data acquisition, data analysis, data interpretation, drafting and writing of the manuscript, final approval and agreement to be accountable for all aspects of the work. SG: data acquisition, data interpretation, drafting and writing of the manuscript, final approval and agreement to be accountable for all aspects of the work. ECC: conceptualisation, data acquisition, manuscript review, final approval and agreement to be accountable for all aspects of the work. RV: data analysis, data interpretation, drafting and writing of the manuscript, final approval and agreement to be accountable for all aspects of the work. EN, JGM, HJGMC: conceptualisation, data interpretation, manuscript review, final approval and agreement to be accountable for all aspects of the work. PSN, JEW, SS: conceptualisation, data interpretation, drafting and writing of the manuscript, final approval and agreement to be accountable for all aspects of the work.
Funding This work was supported by Stichting de Weijerhorst, Maastricht, Limburg, The Netherlands.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Institutional Medical Ethics Committee Maastricht University Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Aortic and vascular disease