Article Text

Abstract
Clinical Introduction An 82-year-old man with a history of coronary artery bypass surgery, hypertension and small bowel gastrointestinal stromal tumour underwent cardiac risk evaluation prior to surgical resection of his tumour. He was asymptomatic from a cardiovascular perspective, but his activity level was less than four metabolic equivalents. Physical examination was notable for a 2/6 systolic murmur at the apex. ECG showed sinus rhythm. A transthoracic echocardiogram was performed (figure 1 and online supplementary video 1).
Supplementary file 1

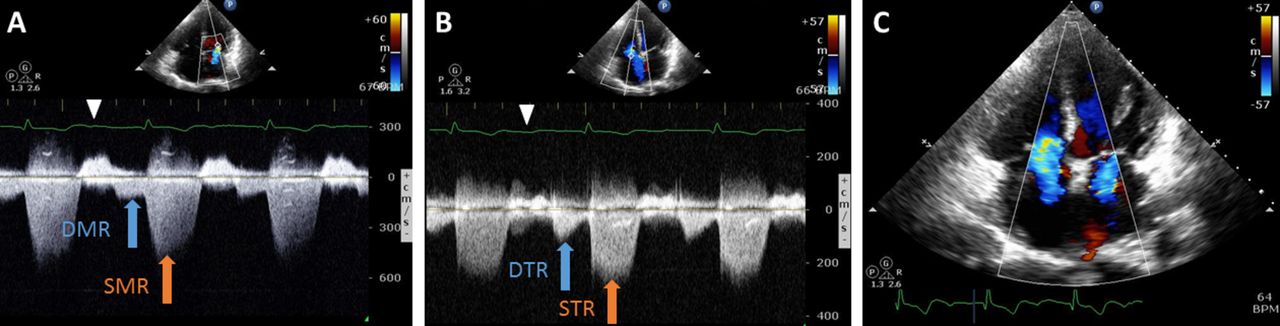
Transthoracic echocardiography. (A) Mitral valve continuous wave Doppler and (B) tricuspid valve continuous wave Doppler.
QUESTION: The findings in figure 1 are most likely due to which of the following?
Atrioventricular conduction block.
Acute severe aortic regurgitation.
Patent ductus arteriosus.
Atrial flutter.
Severe mitral stenosis.
- echocardiography
- valvular heart diseas
Statistics from Altmetric.com
Answer: A
Figure 1A,B demonstrates continuous wave Doppler tracings of mitral and tricuspid regurgitation with diastolic mitral regurgitation (DMR) and diastolic tricuspid regurgitation (DTR). DMR and DTR appear in late diastole when ventricular end diastolic pressures exceed atrial pressures, which is commonly seen in atrioventricular (AV) conduction disorders.1 2 Thus, choice A is correct given the first-degree AV block on the ECG rhythm strip (figure 2). Severely elevated ventricular filling pressures at end diastole, as seen in acute aortic/pulmonic regurgitation, may also lead to DMR/DTR.3 Choice B is incorrect because isolated aortic regurgitation would cause DMR but not DTR. Choice C is incorrect as Doppler tracings of patent ductus arteriosus would show continuous diastolic forward flow from the parasternal view of the main pulmonary artery and not from the mitral/tricuspid valves. Atrial flutter (choice D) with variable AV block has been shown to cause DMR/DTR due to AV dyssynchrony, but the ECG rhythm strip and Doppler tracings do not show atrial flutter (figure 2).4 Isolated mitral stenosis (choice E) would not be expected to cause DMR/DTR and may provide protection of the left ventricle from the high ventricular diastolic pressures that cause reversal of diastolic flow.
{kind=link}
{kind=link}
Transthoracic echocardiography. (A) Mitral valve and (B) tricuspid valve. (C) Apical four chamber with colour Doppler still image. DMR, diastolic mitral regurgitation; DTR, diastolic tricuspid valve regurgitation; SMR, systolic mitral regurgitation; STR, systolic tricuspid regurgitation; white arrowhead indicates p-wave.
Footnotes
Contributors All listed authors participated in the drafting of the submitted work and fulfil criteria for authorship. DFK: case review, manuscript planning and drafting. KA and JL: case review, manuscript drafting and critical review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.