Article Text

Abstract
Background The influence of marital status on the incidence of cardiovascular disease (CVD) and prognosis after CVD is inconclusive. We systematically reviewed the literature to determine how marital status influences CVD and prognosis after CVD.
Methods A search of MEDLINE and Embase in January 2018 without language restriction was performed to identify studies that evaluated the association between marital status and risk of CVD. Search terms related to both marital status and CVD were used and included studies had to be prospective in design. The outcomes of interest were CVD, coronary heart disease (CHD) or stroke incidence and mortality. We performed random effects meta-analysis stratified by the types of population by calculating odds ratios (OR) and 95% confidence intervals (95% CI).
Results Our analysis included 34 studies with more than two million participants. Compared with married participants, being unmarried (never married, divorced or widowed) was associated with increased odds of CVD (OR 1.42; 95% CI 1.00 to 2.01), CHD (OR 1.16,95% CI 1.04 to 1.28), CHD death (OR 1.43,95% CI 1.28 to 1.60) and stroke death (OR 1.55,95% 1.16 to 2.08). Being divorced was associated with increased odds of CHD (P<0.001) for both men and women while widowers were more likely to develop a stroke (P<0.001). Single men and women with myocardial infarction had increased mortality (OR 1.42, 95% CI 1.14 to 1.76) compared with married participants.
Conclusions Marital status appears to influence CVD and prognosis after CVD. These findings may suggest that marital status should be considered in the risk assessment for CVD and outcomes of CVD based on marital status merits further investigation.
- meta-analysis
- systemic review
- acute coronary syndromes
- stroke
Statistics from Altmetric.com
Introduction
Cardiovascular disease (CVD) is associated with significant morbidity and mortality.1 In order to reduce the burden of CVD, there is great interest in identifying risk factors in the general population so that those deemed to be at high risk for future cardiovascular events can be targeted for intervention. While 80% of the risk for future CVD can be predicted from known cardiovascular risk factors such as old age, male sex, hypertension, hyperlipidaemia, smoking and diabetes mellitus, the determinants for the remaining 20% risk remain unclear.2
One factor which may be associated with CVD is marital status and studies have reported inconsistent findings. The benefits of marriage on health and mortality have been demonstrated for both sexes, in different ethnic groups and appear to be independent of various sociodemographic characteristics.3 4 Better prognosis in married individuals has been reported both after myocardial infarction3 5–10 and stroke,11 12 whereas, other studies found no influence of marital status on risk of future CVD.13–15 In addition, sex differences have been observed where the degree of ‘protection’ conferred in men from being married tends to be greater.16 17 The interpretation of marital status and CVD becomes more complex with the addition of divorced and widowed groups.15 18–20
In view of these disparate findings reported in the literature, we conducted a systematic review and meta-analysis to evaluate the risk of CVD based on marital status and the influence of marital status on prognosis after CVD.
Methods
This systematic review and meta-analysis was conducted and reported according to the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).21
Eligibility criteria
We selected studies which evaluated cardiovascular events or mortality in participants according to marital status. The included studies had at least two groups (married and unmarried, divorced or widowed) and followed participants for incident cardiovascular events or mortality outcome after incident CVD. Studies of patients with suspected coronary heart disease were also included but not pooled with other studies with myocardial infarction. Only prospective studies published since 2000 were retained for analysis to limit issues related to quality of study reporting and generalisability to contemporary clinical practice. There was no exclusion of studies based on the length of follow-up, language of publication or definition of cardiovascular events such as ischaemic heart disease, coronary heart disease, myocardial infarction and stroke. However, we excluded studies of heart failure, retrospective analyses, case–control studies and those studies which did not report the numerical association between marital status and outcome. Reviews were examined for additional studies that met the inclusion criteria.
Search strategy
We searched MEDLINE and Embase from 2000 onwards using OVID SP with no date or language restriction. This search was last updated in January 2018. The exact free search terms were (‘marital status’ or ‘married’ or ‘unmarried’ or ‘widowed’ or ‘divorced’) AND (‘myocardial infarction’ or ‘acute coronary syndrome’ or ‘coronary heart disease’ or ‘ischaemic heart disease’ or ‘ischaemic heart disease’ or ‘heart attack’ or ‘stroke’ or ‘cerebrovascular disease’ or ‘cerebrovascular accident’). We checked the bibliography of relevant studies and reviews for additional studies that met the inclusion criteria.
Study selection process and data collection process
Two reviewers (CWW and CSK) independently screened all titles and abstracts retrieved from the search for studies that met the inclusion criteria. The full articles of studies that potentially met the inclusion criteria were reviewed and the final decision to include or exclude was made with the other reviewers. Independent double extractions were performed by two reviewers (CWW and CSK) collecting data on study design, year, country, number of participants, mean age, % male, participant inclusion criteria, comparison groups and results, while independent double extractions for quality assessment table were completed by CWW and another reviewer (AN).
Risk of bias assessment
Quality assessment of the studies was conducted based on the recommendations of the Cochrane Handbook for Systematic Review and previous published systematic reviews of observational studies.22
Data analysis
We used Review Manager V.5.3.5 (Nordic Cochrane Centre) to conduct random effects meta-analysis stratified by the type of population which were either general population, post stroke or post myocardial infarction and marital status. We used random effects because the studies were conducted in a wide range of settings in different populations, hence the need to take heterogeneity into account for the pooled effect estimate. Where possible, we chose to pool reported adjusted risk estimates from primary studies and when these data were not available, raw data were used to calculate unadjusted risk estimates. We used the I2 statistic to assess statistical heterogeneity. I2 values of 30–60% represent moderate levels of heterogeneity and sensitivity analysis was performed to evaluate analyses with high statistical heterogeneity. Publication bias was assessed by asymmetry testing with funnel plots if there was no evidence of significant heterogeneity.23 Further subgroup analyses were performed to investigate the impact of sex differences combined with marital status on various cardiovascular outcomes. Further analyses were also performed with the exclusion of studies with unclear marital status ascertainment and another with the exclusion of studies with only crude results or unadjusted results available.
Results
Description of studies included in analysis
The process of study selection is shown in figure 1. After screening, 32 studies were retained for inclusion and two additional studies were identified from a review yielding a total of 34 studies for analysis. Table 1 summarises the study designs and participant characteristics. These 34 studies, which took place in various countries including Russia, Denmark, Spain, USA, Sweden, UK, Canada, Israel, Gulf States, Japan, Finland, Greece, Turkey, Norway and China between 1963 and 2015. The follow-up period from these studies ranged from 30 days to 34 years. There were more than 2 million participants (ranging from 135 to 7 34 626 participants). Data on age are available for 1 137 571 participants from 25 studies with a mean of 58.4 years (range 42 to 77 years). The definition of unmarried used in each study is presented in the online supplementary table 1.
Supplemental material

Flow diagram of study selection.
Study design and participant characteristics
Quality assessment of included studies
The quality assessment of included studies is summarised in online supplementary table 2. Twenty-four studies were found to have used reliable methods for ascertaining the marital status which involved utilising databases,7 11 14–16 20 24 25 questionnaires,2 9 13 17 18 26–29 and interviews.9 12 19 25 30–34 Reliable outcome ascertainment was found in 25 studies either from databases,6 7 11 13–18 20 24 25 28–30 32 33 35–37 medical records,6 7 13 16 17 30 31 34 or assessment by healthcare professionals or research teams.2 18 19 29 Seventeen studies reported a low rate of loss to follow-up of <10%.2 6 7 9 13–15 17–20 24 29 30 32 33 35 Twenty-nine studies included adjusted analyses,3 6–10 13–20 24–27 29 31 33–38 three studies included unadjusted analysis9 11 12 and five studies had only crude results available.2 30 32 39 40 For assessment of publication bias, the funnel plots conducted showed no significant asymmetry in the pattern of distribution of studies (online supplementary figures 1–14).
Pooled analysis of marital status and cardiovascular outcomes
Mortality in the general population
The results for the general population as well as by gender are summarised in tables 2-4 (and online supplementary table 2 and online supplementary figures 1–2 and 4–13). Compared with married participants, unmarried participants were more likely to die from both CHD (OR 1.43, 95% CI 1.28 to 1.60, I2=57%, P<0.001, n=5) and stroke (OR 1.55, 95% CI 1.16 to 2.08, I2=0%, P=0.003, n=2) (figure 2A and figure 2B).
Follow-up and results
Risk of adverse outcomes considering marital status in the general population
Risk of adverse outcomes considering marital status in specific groups of participants

Forest plots of coronary heart disease (CHD), stroke and cardiovascular disease (CVD) deaths in unmarried vs married in the general population.
Being divorced was associated with an increased odds of CHD mortality (OR 1.33, 95% CI 1.04 to 1.70, I2=0%, n=3) (online supplementary figure 4) and stroke mortality (OR 2.33, 95% CI 1.11 to 4.89, I2=0%, P=0.03, n=1) (online supplementary figure 6). Widowed participants of either sex in these studies did not have increased CHD mortality or stroke mortality (online supplementary figures 5 and 7).
Cardiovascular risks in general population
Unmarried participants were 1.4 times more likely to develop CVD (OR 1.42, 95% CI 1.00 to 2.01, P=0.05, n=1) (figure 3C) with a slight increase in the odds of developing CHD (OR 1.16, 95% CI 1.04 to 1.28, I2=69%, P=0.006, n=8) (figure 3A), but no difference was observed for incident stroke (P=0.15, n=4) compared with married participants (figure 3B).

Forest plot of coronary heart disease (CHD), stroke and cardiovascular disease (CVD) events in unmarried vs married in the general population.
Results for divorced and widowed patients is shown in table 3. Being divorced in both sexes were 1.3 times more likely to develop CHD (OR 1.35, 95% CI 1.20 to 1.53, I2=0%, P<0.001, n=3) (online supplementary figure 10) with a slight increase in incident stroke odds (OR 1.15, 95% CI 1.01 to 1.29, I2=53% P=0.02, n=4) (online supplementary figure 12). In contrast, widowed participants were more likely to develop a stroke (OR 1.16, 95% CI 1.09 to 1.23, I2=0%, P<0.001, n=4) (online supplementary figure 13) but not CHD (P=0.07, n=1) (online supplementary figure 11).
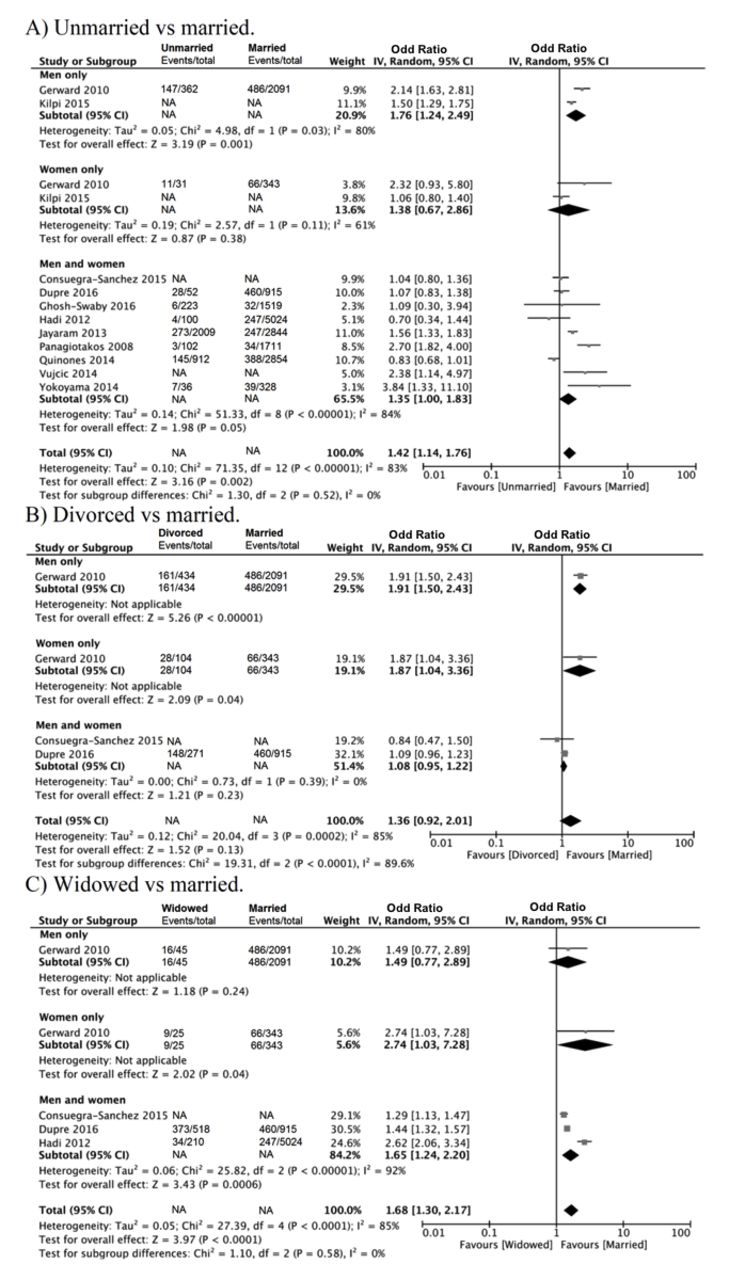
Mortality in CVD population (MI and stroke)
Results for participants with CVD, for the whole population and stratified by gender are summarised in figure 4 and table 4. Mortality was significantly higher for unmarried patients who sustained a myocardial infarction (OR 1.42, 95% CI 1.14 to 1.76, I2=83%, P<0.002, n=11) (figure 4A). Being divorced is not associated with increased mortality after MI (P=0.13, n=3) (figure 4B). For widowed participants, the increased odds of death post-MI was almost 1.7 times (OR 1.68, 95% CI 1.30 to 2.17, I2=85%, P<0.001, n=4) (figure 4C).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of post myocardial infarction mortality by marital status.
After a stroke, there was no difference in mortality between unmarried and married participants (P=0.47, n=3) (online supplementary figure 14).
Mortality in post-cardiac catheterisation population
In the post-cardiac catheterisation population consisting of a heterogeneous cohort of patients under elective investigation for possible coronary artery disease or acutely following a myocardial infarction, there was no significant difference in all-cause mortality in the unmarried, divorced and widowed groups when compared with married participants with adjusted hazard ratio (aHR) 1.14 (95% CI 0.95 to 1.37), aHR 1.23 (95% CI 0.98 to 1.55), and aHR 1.24 (95% CI 0.99 to 1.54), respectively. Both the unmarried and widowed participants were at increased risk of cardiovascular death, corresponding aHR 1.33 (95% CI 1.06 to 1.68) and aHR 1.62 (95% CI 1.23 to 2.13), respectively, but the risk was not significant in divorced participants (aHR 1.27, 95% CI 0.95 to 1.69).
Discussion
To the best of our knowledge, this is the first evidence synthesis to quantify the evidence base using meta-analysis to evaluate the relationship between marital status and cardiovascular disease. Our analysis showed that compared with married individuals, being unmarried was associated with increased CHD and both CHD and stroke mortality in the general population. Similarly, we observed greater odds of death from CHD and stroke in divorced compared with married individuals. Finally, in the widowed population only stroke incidence was elevated with similar odds in both sexes. Our analysis also describes important differences in prognosis with regard to mortality according to marital status in patients with incident cardiovascular disease. In participants who suffered a myocardial infarction, being unmarried was associated with greater odds of mortality compared with a married individual, with a non-significant trend in widowed or divorced individuals. In our analysis, no significant gender effect was observed for the association between marital status and developing CVD and death from CVD in any groups of participants, although differences in total mortality were noted.
We have built on the current understanding of marital status and adverse outcomes in several ways. First, a previous meta-analysis of 53 studies demonstrated higher all-cause mortality in never married, divorced and widowed married versus married individuals,41 but the study did not explore any specific causes of death or cardiovascular disease. A more recent review published by Manfredini et al describes the improved health status and reduced cardiovascular risk with married status but it did not quantify the relationships with meta-analysis.42 Our updated review with 34 studies has built on the findings of these reviews to quantify the relationship between marital status and CVD while considering the unmarried, divorced and widowed status of the populations assessed.
Several mechanisms have been suggested to account for the observed protective effect of marital status on CVD, especially in men. Social causation theory suggests that individuals benefit from spousal support.43 For example, living with another person allows earlier recognition and response to warning symptoms,16 25 especially if a myocardial infarction becomes instantly disabling.25 Studies have reported that unmarried patients had longer delays in seeking medical help7 8 16 44 and longer total ischaemic times44 which directly influences both the timing and proportion of participants being treated with either thrombolysis or invasive cardiac procedures that reduce mortality.7 8 In addition, spouses, particularly wives, encourage concordant health behaviour such as a healthy lifestyle13 16 19 45 and adherence to treatment5 13 16 19 45 that promote cardiovascular health. In contrast, marital dissolution is noted to affect the health behaviour mentioned above negatively.29 Moreover, Wu et al reported that compared with married individuals, unmarried individuals were twice more likely to be non-adherent to their prescribed medications which was the strongest predictor of better outcome in their study.45 There are greater financial resources, especially in households with a dual income, making better healthcare more accessible.13 16 30 Furthermore, one of the benefits of being married or with a partner may be increased participation in cardiac rehabilitation which improves outcomes after cardiovascular disease.46
Stress-related theory suggests that partner loss or poor-quality relationships may have a negative impact on the economic, behavioural and emotional well-being of an individual which may reduce one’s ability to prevent, detect and treat illness.33 Biologically, stress may ultimately worsen cardiovascular risk factors such as hypertension, reduced heart rate variability, impaired vagal tone, hyperlipidaemia, diabetes and the progression of atherosclerosis.9 29 32 The buffering hypothesis suggests that informational or emotional resources from a spouse promote adaptive behaviour and may reduce excessive neuroendocrine response to acute or chronic stressors.17 35 This translates into a decrease in progression of atherosclerosis and other pathological processes, thus reducing the risk of CVD.
Furthermore, selection theory has been introduced which assumes that individuals with poor health are less likely to establish or maintain long-term relationships such as marriage.5 33 Also, Floud et al suggested the possibility that healthy women may be less likely to divorce,13 although Akimova et al reported that divorced and single women were more highly educated and had a higher qualified occupation which results in greater financial independence and better quality of life.35
In widowed populations, there is less variation in CVD incidence and mortality between sexes with some studies showing women do more poorly than men. Vujcic et al showed that the proportion of women who lived alone increased with age while the proportion of men who lived alone decreased with age.9 Possible explanations include women tend to be younger than their husbands and have a longer life expectancy.9 Thus, it is postulated that widowed women tend to be older and more support is needed to meet their healthcare requirement. This study has several strengths and limitations. This is the largest study to date with a sample size of more than 2 million compared with the smaller sample sizes of previous reviews.41 42 We were able to quantify the risk with meta-analysis which was not performed in the previous studies.42 In terms of generalisability, the current review included populations from various age groups, ethnicities and geographic locations making the findings generalisable to different populations. We used a comprehensive search strategy of the literature and excluded case-control and retrospective studies to reduce the possibility of bias. Finally, results with the greatest extent of adjustments were used for the analysis in this study.
The major limitation of this study is the inconsistent variable adjustments across studies, which poses a risk of confounding. Adjustment for cardiovascular risk factors was often incomplete in many of the studies analysed, which may have influenced our result. In addition, this review is not an individual patient meta-analysis so information is solely derived from published material. The lack of information on same-sex spouses and quality of marriage limit further insight into the impact of marriage. Moreover, heterogeneity exists across studies in terms of study methodology. For example, the definition of CVD varied across the studies and the follow-up period was inconsistent with some long-term studies (>15 years of follow-up) where management might have changed over time.7 19 20 30 36 37
Future work should focus on whether marital status is a surrogate marker of other adverse health behaviour or cardiovascular risk profiles that underlies our reported findings and whether targeted interventions should focus on such high-risk groups. The association between cohabitation/living with someone and CVD should be explored as it may be a confounding factor in this study. In Quinones et al, the replacement of marital status with cohabitation yielded the same protective effect although slightly less pronounced.33 Fournier et al suggested that having information of ‘living alone’ versus ‘living with someone’ instead of married versus not married would have been more useful.43
In conclusion, being married appears to be associated a lower cardiovascular mortality and incidence of CVD in a general population and mortality after myocardial infarction. While current evidence may demonstrate an association between marital status and mortality and CVD, lack of social support might be a mitigating factor. Future research should focus around whether marital status is a surrogate marker for other adverse health behaviour or cardiovascular risk profiles that underlies our reported findings, or whether marital status should be considered as a risk factor by itself.
Key questions
What is already known about this subject?
While 80% of the risk for future cardiovascular disease (CVD) can be predicted from known cardiovascular risk factors such as hypertension, smoking and diabetes mellitus, the determinants for the remaining 20% risk remain unclear.
One factor which may be associated with CVD is marital status and studies have reported inconsistent findings.
What does this study add?
Our analysis showed that compared with married individuals, being unmarried was associated with increased all cause mortality, coronary heart disease (CHD) and both CHD and stroke mortality in the general population.
Similarly, we observed a greater odds of death from CHD and stroke in divorced compared with married individuals.
In the widowed population only stroke incidence was elevated with similar odds in both sexes.
How might this impact on clinical practice?
These findings may suggest that marital status should be considered in the risk assessment for CVD.
Acknowledgments
We acknowledge the ASPIRE Summer Studentship programme at Keele University for the support of this work.
References
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
Contributors MAM and CSK conceived and planned the study. CSK and CWW performed the search for relevant studies. Data were screened, extracted and analysed by CSK and CWW. CWW wrote the first draft of the paper. All authors contributed to the interpretation of the findings and critically revised it for intellectual content.
Funding This work is supported by the ASPIRE Summer Studentship programme at Keele University.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Correspondence
- Miscellaneous