Article Text

Abstract
Objective Bileaflet mitral valve prolapse (MVP) with either focal or diffuse myocardial fibrosis has been linked to ventricular arrhythmia and/or sudden cardiac arrest. Left ventricular (LV) mechanical dispersion by speckle-tracking echocardiography (STE) is a measure of heterogeneity of ventricular contraction previously associated with myocardial fibrosis. The aim of this study is to determine whether mechanical dispersion can identify MVP at higher arrhythmic risk.
Methods We identified 32 consecutive arrhythmic MVPs (A-MVP) with a history of complex ventricular ectopy on Holter/event monitor (n=23) or defibrillator placement (n=9) along with 27 MVPs without arrhythmic complications (NA-MVP) and 39 controls. STE was performed to calculate global longitudinal strain (GLS) as the average peak longitudinal strain from an 18-segment LV model and mechanical dispersion as the SD of the time to peak strain of each segment.
Results MVPs had significantly higher mechanical dispersion compared with controls (52 vs 42 ms, p=0.005) despite similar LV ejection fraction (62% vs 63%, p=0.42) and GLS (−19.7 vs −21, p=0.045). A-MVP and NA-MVP had similar demographics, LV ejection fraction and GLS (all p>0.05). A-MVP had more bileaflet prolapse (69% vs 44%, p=0.031) with a similar degree of mitral regurgitation (mostly trace or mild in both groups) (p>0.05). A-MVP exhibited greater mechanical dispersion when compared with NA-MVP (59 vs 43 ms, p=0.0002). Mechanical dispersion was the only significant predictor of arrhythmic risk on multivariate analysis (OR 1.1, 95% CI 1.02 to 1.11, p=0.006).
Conclusions STE-derived mechanical dispersion may help identify MVP patients at higher arrhythmic risk.
- echocardiography
- valvular heart disease
- cardiac arrest
- mitral regurgitation
- ventricular tachycardia
Statistics from Altmetric.com
Introduction
Mitral valve prolapse (MVP) is a common valvulopathy affecting 2%–3% of the general population.1 2 Although a subset of MVP patients (0.8%–2.5%) will develop cardiac arrest or sudden cardiac death,3–5 no predictors of this devastating outcome are readily available. Previously, sudden cardiac death in MVP has been linked to chordal rupture and severe mitral regurgitation (MR).6 Other studies describe a high arrhythmic risk in a bileaflet phenotype with mild MR, inferior T-wave inversions on ECG and complex ventricular ectopy.7 In this phenotype, focal myocardial fibrosis may be identified within the papillary muscles or the inferolateral base of the left ventricle (LV) on cardiac magnetic resonance (CMR) late gadolinium enhancement images and autopsy specimens.7 Focal fibrosis has been linked to the presence of mitral annular disjunction, a separation between the left atrial wall at the level of mitral valve junction and the LV free wall with associated systolic curling, leaflet hypermobility and mechanical traction on the papillary muscles and inferolateral LV base.8 However, in other arrhythmic MVP patients, diffuse interstitial fibrosis has been demonstrated using T1 mapping CMR, even without the presence of focal fibrosis, mitral annular disjunction or severe MR.9 Moreover, in electrophysiological studies, ventricular ectopy does not always originate from the LV papillary muscles or inferolateral base in MVP. LV and right ventricular outflow tracts and the anterolateral LV base have also been described as clinical foci of ventricular arrhythmia in MVP patients.10 These findings suggest the existence of a primary diffuse myopathic process that goes beyond focal myocardial traction and/or volume overload. Hence, imaging parameters of diffuse myocardial involvement become particularly important for arrhythmic risk stratification in MVP.
Speckle-tracking echocardiography (STE) can be used to quantify global longitudinal strain (GLS). Whereas GLS is a measure of overall longitudinal contraction of the myocardium, STE-derived mechanical dispersion is a parameter of heterogeneous ventricular contraction. Mechanical dispersion has been shown to be predictive of arrhythmic risk in several conditions including ischaemic heart disease, hypertrophic cardiomyopathy, dilated cardiomyopathy and arrhythmogenic right ventricular cardiomyopathy.11–13 Importantly, mechanical dispersion has been shown to correlate with the extent of myocardial fibrosis in other arrhythmogenic myopathies.12 We hypothesise that increased STE-derived mechanical dispersion is associated with a higher prevalence of arrhythmic complications in patients with MVP.
Methods
Study population
Through query of the University of California, San Francisco clinical and echocardiographic database, we identified 483 consecutive MVP cases between January 2013 and December 2016. Of these, 32 patients had a history of significant ventricular arrhythmia (A-MVP) based on (1) complex ventricular ectopy on Holter/event monitor or (2) implantable-cardioverter defibrillator (ICD) placement for aborted cardiac arrest. Complex ventricular ectopy was defined as the presence of couplets, ventricular bigeminy, non-sustained or sustained ventricular tachycardia.11 14 An additional 32 consecutive MVP patients without a history of ventricular arrhythmia (NA-MVP) were identified based on (1) a negative Holter/event monitor or (2) no complaint of palpitations while being regularly followed by a local cardiologist. Patients were excluded if they had a history of documented coronary artery disease, prior myocardial infarction, cardiac surgery, congenital heart defects, significant aortic valve disease, poor echocardiographic image quality or low frame rate. Five patients were removed from the NA-MVP group based on the exclusion criteria, with a final number of 27 NA-MVP cases. Coronary artery disease was assessed in all A-MVP patients using a stress ECG study (8), a stress echocardiogram (13), a nuclear stress test (6) or coronary angiography (5).
Thirty-nine age-matched and gender-matched healthy volunteers without MVP were selected from the Health eHeart Study to serve as controls. The Health eHeart Study is an internet-based cardiovascular cohort study with available echocardiograms in a subset of participants living in the San Francisco Bay Area.14 All individuals in the control group were free from cardiovascular disease and had normal physical examination, ECGs and supine bicycle exercise studies.
The following baseline demographic and clinical information was obtained for each study participant: age, gender, body surface area, heart rate, systolic/diastolic blood pressure, use of cardiac medications, history of atrial fibrillation, hypertension, diabetes mellitus and tobacco use. Patient ECGs from the time of their index echocardiogram were reviewed and assessed for QT-interval, QRS width and the presence of T-wave inversions.
All participants gave written informed consent.
Standard echocardiography
MVP patients underwent routine two-dimensional echocardiography studies using a variety of commercially available cardiovascular ultrasound machines as part of standard clinical evaluation. Healthy controls underwent complete echocardiographic evaluation as part of a research protocol within the Health eHeart Study (Vivid E9, GE Healthcare).15 The following echocardiographic parameters were collected in all study participants: LV ejection fraction, LV end-diastolic and end-systolic volume, LV mass, left atrial volume, presence and type of MVP, presence of mitral annular disjunction, degree of MR and the presence of right ventricular dilatation (basal diameter ≥4.2 cm) or visual systolic dysfunction (yes/no). LV ejection fraction, LV mass and left atrial volume were quantified as previously described.15 LV volumes, LV mass and left atrial volume were indexed to body surface area. MR was quantified using the largest vena contracta width by two-dimensional colour Doppler in either a parasternal or apical three-chamber long axis view.15 MVP was diagnosed as leaflet displacement >2 mm beyond the mitral annulus in a parasternal or apical three-chamber long-axis view.1 The presence of mitral annular disjunction was assessed qualitatively in the parasternal long-axis view as a separation between the left atrial wall at the level of mitral valve junction and the LV free wall.
Speckle-tracking echocardiography
STE analysis was performed retrospectively using the TomTec Image Arena V.4.6 Software. Representative two-chamber, three-chamber and four-chamber images with maximal endocardial definition were selected from the index echocardiograms of each patient. The endocardial border of the LV was outlined by the operator in the end-systolic frame of each image. Speckle-tracking of each of the 18 LV segments was conducted throughout the cardiac cycle. Minor adjustments were made if necessary by the operator to maximise tracking. The peak systolic strain was obtained for each segment and averaged for all 18 as a representation of GLS. The time from onset Q/R wave on ECG to the point of peak strain was defined as the time to peak strain. LV mechanical dispersion was defined as the SD of the time to peak strain in all 18 segments.
Two independent observers (SE and FND) performed measurements of mechanical dispersion on 10 MVP patients blinded to clinical data to ensure obtained values were reproducible. Intraobserver and interobserver variabilities for GLS in MVP have been previously reported.16
Statistical analyses
Continuous variables were assessed for normality using quantile-quantile plots. Normally distributed variables were summarised as mean and SD. Non-normally distributed variables were expressed as median and quartiles. Categorical data were expressed as number and percentage of total patients in each group. Differences between groups were assessed using the Χ2 test for categorical variables and the general linear model or Wilcoxon rank sum test for continuous variables. Logistic regression analysis was performed for the prediction of arrhythmic risk in MVP patients using several models. For the first model, the following variables were selected for inclusion in the multivariate analysis: bileaflet involvement and mechanical dispersion were selected based on meeting statistical significance (p0.05) in the univariate logistic regression analyses and degree of MR (assessed by vena contracta width) was forced into the model. The second model included only mechanical dispersion and MR vena contracta width. The third model included only bileaflet involvement and MR vena contracta width. Reproducibility of mechanical dispersion measurements was expressed as the intraclass correlation coefficient. Two-tailed p values of <0.05 were considered statistically significant. Analyses were performed using standard statistical software (SAS V.9.4, SAS Institute, Cary, North Carolina, USA).
Results
Baseline clinical characteristics
A total of 97 patients were included in the analysis: 59 patients with MVP and 39 healthy controls. MVP patients were similar to controls in regard to age, gender, body surface area, systolic blood pressure, history of hypertension and QRS duration (all p0.05) (table 1). There were 12 MVPs with a history of atrial fibrillation, but none during echocardiographic evaluation. MVP patients had higher average HR (p<0.001), longer QTc duration (p=0.022) and greater utilisation of antiarrhythmic medications (p=0.026) (table 1).
Clinical characteristics of mitral valve prolapse patients and controls
Baseline echocardiographic characteristics
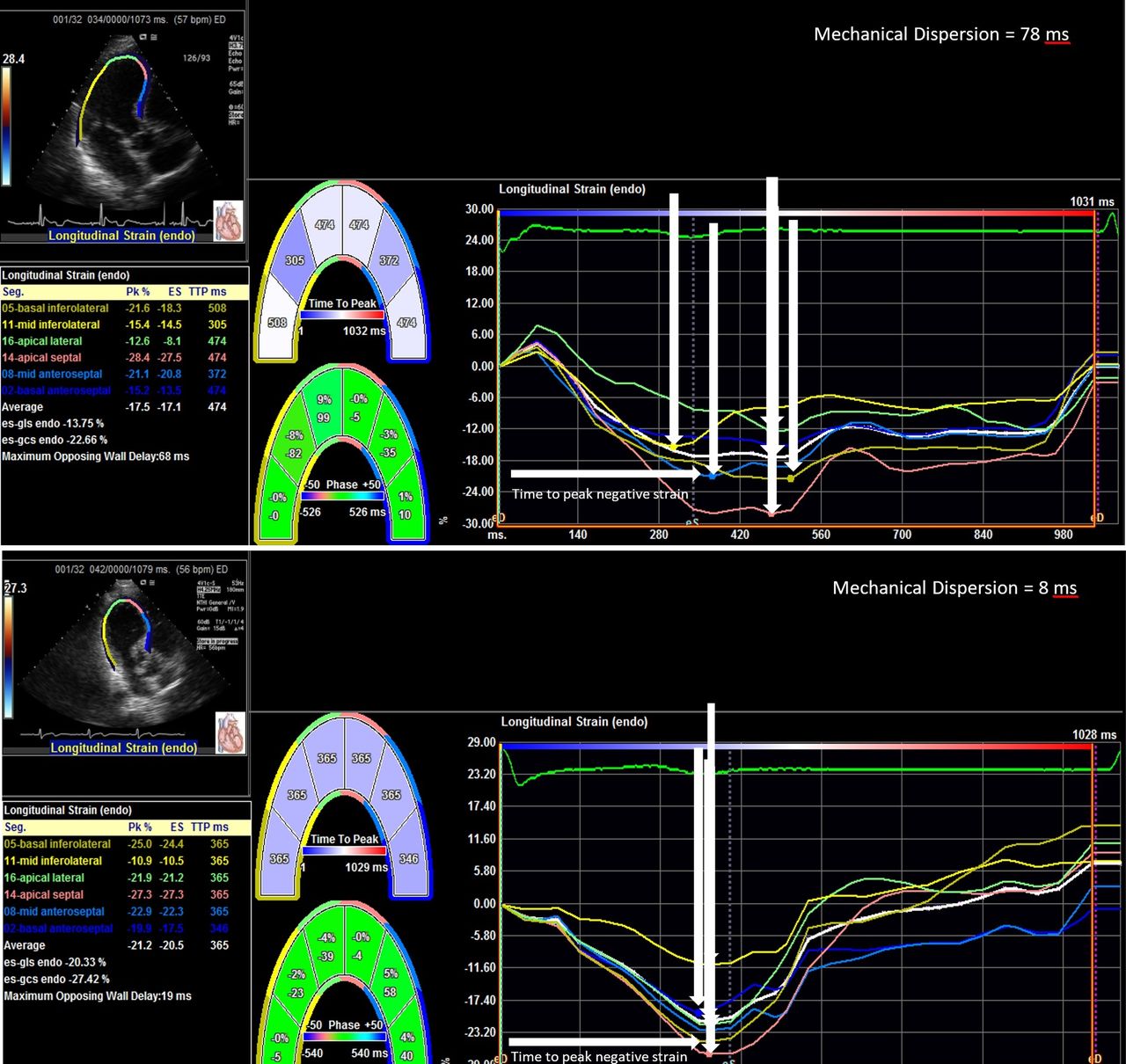
MVP patients differed significantly from controls in regard to their echocardiographic characteristics (table 1). MVP patients had higher LV end-diastolic volume index, LV end-systolic volume index, LV mass index, left atrial volume index and greater degree of MR (all p<0.05) (table 1). The majority of MVP patients had bileaflet prolapse (56%) and trace or mild MR (vena contracta width <0.3 cm) (66%). Only 13 patients had evidence of mitral annular disjunction (22%), all of which had bileaflet MVP. Overall, GLS was lower among MVP patients (−19.7% vs −21%, p=0.045). MVP subjects had higher mechanical dispersion (52 vs 42 ms, p=0.005) compared with controls (figures 1 and 2).
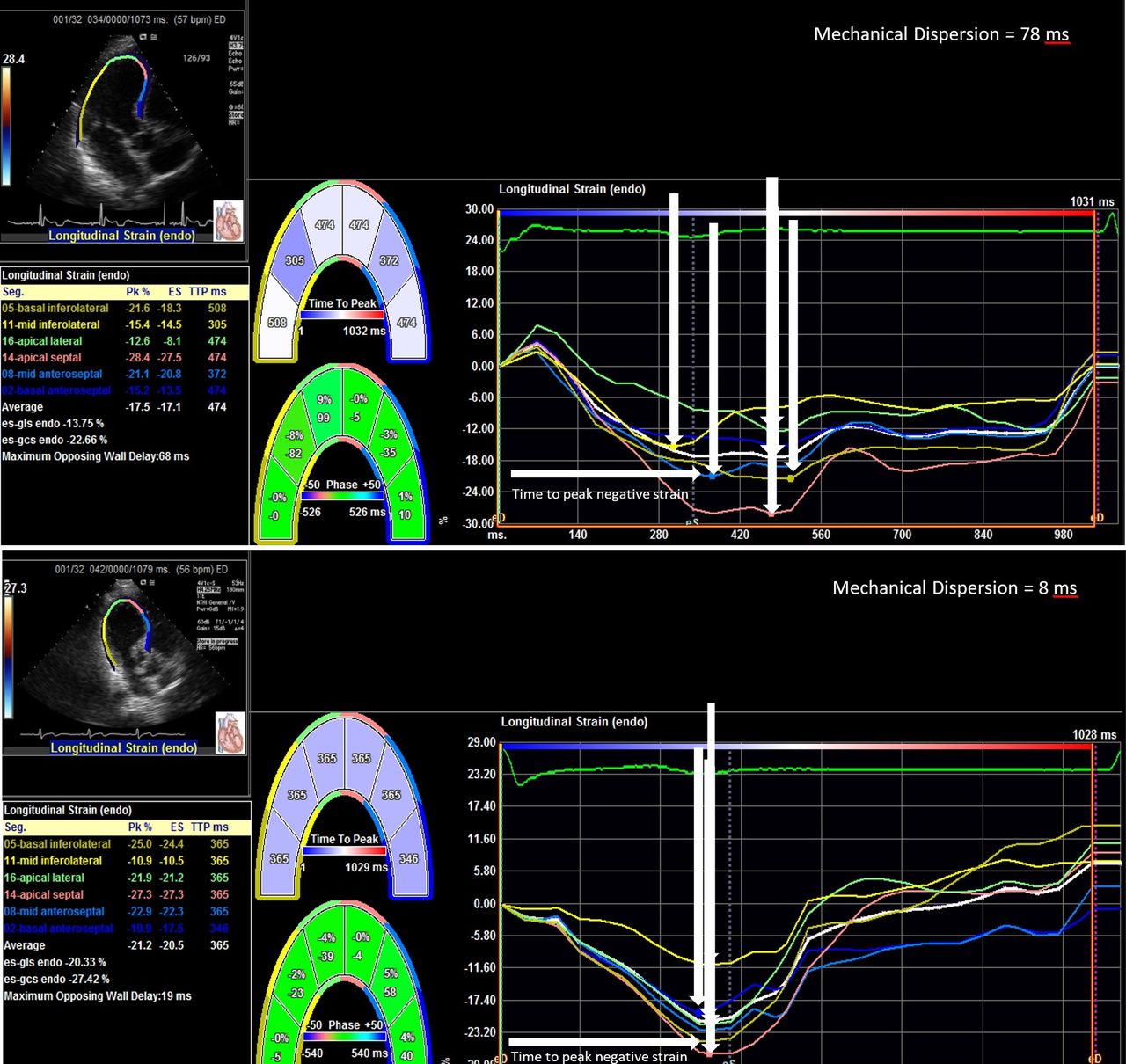
Examples of Tomtec Image Arena measurements of global longitudinal strain (GLS) and time to peak strain (TTP) in arrhythmic mitral valve prolapse (A-MVP) patients (top panel) and non-arrhythmic mitral valve prolapse patients (NA-MVP) (bottom panel). Greater variability in the TTP of each left ventricular (LV) wall segment is seen in the A-MVP patients compared with the NA-MVP patients reflecting increased mechanical dispersion. GLS is defined as the average peak systolic strain for all 18 LV segments. Mechanical dispersion is defined as the SD of the time to peak strain in all 18 LV segments.

Comparison of mechanical dispersion between controls, all mitral valve prolapse patients (MVP total), arrhythmic MVP patients (A-MVP) and non-arrhythmic MVP patients (NA-MVP). A-MVP patients had significantly higher mechanical dispersion compared with controls (mean 59 vs 42 ms, p<0.001) and NA-MVP patients (mean 59 vs 43 ms, p<0.001). There was no difference in mechanical dispersion between the control and the NA-MVP groups (p=0.78).
Ventricular arrhythmia
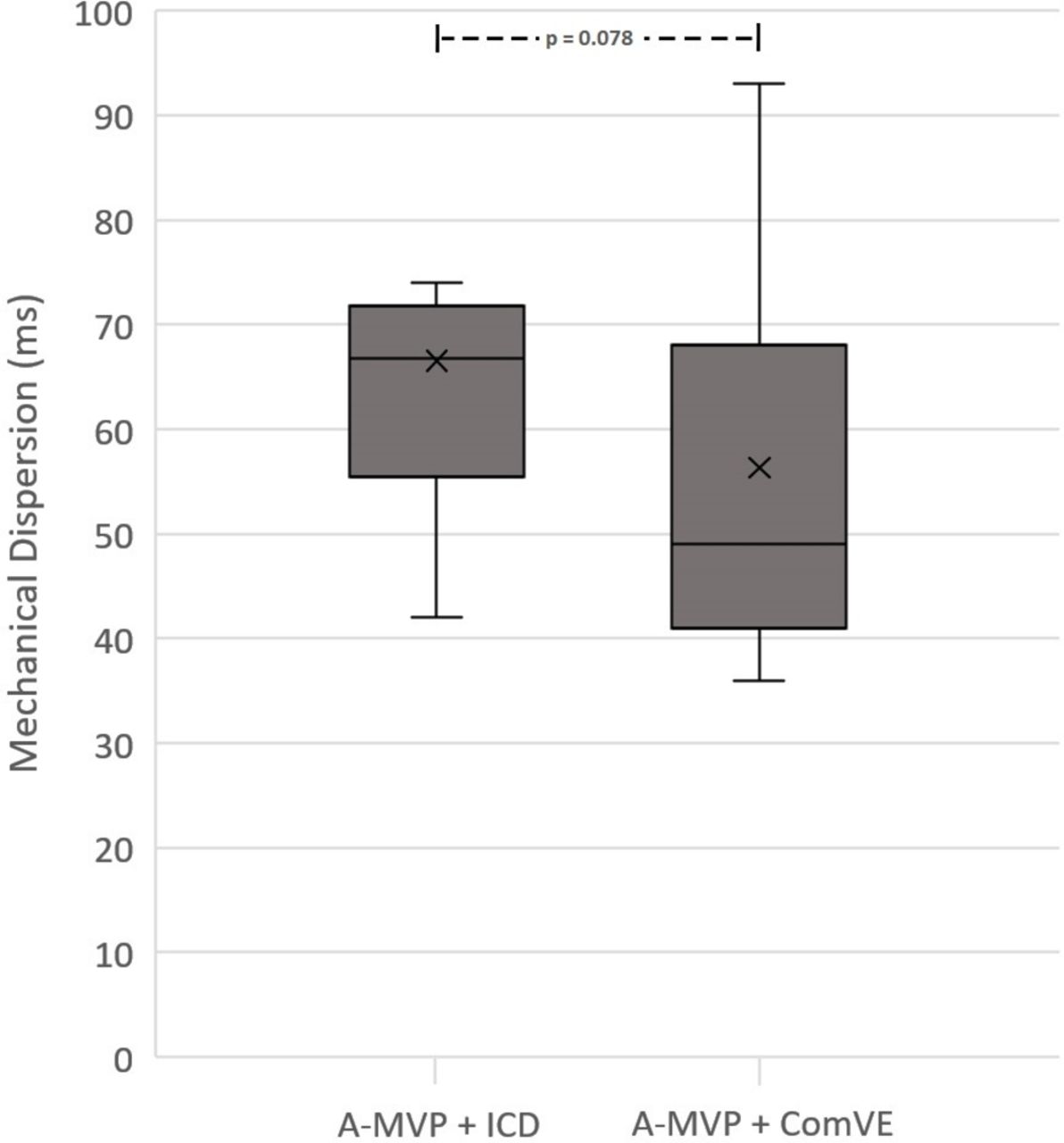
Out of the 59 MVP patients included in our study, 32 were arrhythmic MVP (A-MVP). Of these, 23 patients had complex ventricular ectopy (17 with ventricular tachycardia) on Holter/event monitor and 9 patients had secondary prevention ICDs. There were no relevant differences between the A-MVP and NA-MVP patients in all baseline clinical parameters apart from the use of antiarrhythmic medications (p=0.009) (table 2) in the A-MVP group. There were no differences in standard echocardiographic parameters between A-MVP and NA-MVP patients apart from a greater prevalence of bileaflet MVP in the A-MVP group (p=0.031) (table 2). Specifically, the number of patients with moderate or severe MR (vena contracta width ≥0.3 cm) or with mitral annular disjunction was similar between the two groups (p=0.56 and p=0.97, respectively). GLS was also similar between A-MVP and NA-MVP patients (p=0.37). Mechanical dispersion, however, was significantly higher in the A-MVP group than in the NA-MVP group (mean 59±21 ms vs mean 43±12 ms, p<0.001) (figure 2). Within the A-MVP group, patients treated with an ICD had higher mechanical dispersion than the arrhythmic MVPs with complex ventricular ectopy alone (mean 67±17 ms vs mean 56±22 ms, p=0.078) (figure 3). Mechanical dispersion was not significantly different between monoleaflet or bileaflet MVP (mean 48±16 ms vs mean 55±21 ms, p=0.33). The NA-MVP group was similar to controls with regard to mechanical dispersion (mean 43±12 ms vs mean 42±10 ms,p=0.78). In our first multivariate model including mechanical dispersion, bileaflet involvement and MR vena contracta width, mechanical dispersion was the only significant predictor of arrhythmic risk (OR 1.1, 95% CI 1.02 to 1.11, p=0.006) (table 3). In the second multivariate model including only mechanical dispersion and MR vena contracta width, mechanical dispersion remained the only significant predictor of arrhythmic risk (OR 1.1, 95% CI 1.02 to 1.12, p=0.004). Bileaflet involvement was the most important predictor of ventricular arrhythmia in the third multivariate model including only bileaflet involvement and MR vena contracta width (OR 3.6, 95% CI 1.2 to 10.8, p=0.023).
Clinical characteristics of mitral valve prolapse patients with and without a history of ventricular arrhythmia
Multivariate regression analysis for the outcome of ventricular arrhythmia in mitral valve prolapse
Reproducibility
Reproducibility for mechanical dispersion was good with a correlation coefficient of 0.80 (95% CI 0.78 to 0.84).

{kind=link}
{kind=link}
{kind=link}
Comparison of mechanical dispersion between arrhythmic mitral valve prolapse patients (A-MVP) treated with an implantable-cardioverter defibrillator (ICD) and A-MVP with complex ventricular ectopy on monitor (ComVE). Mechanical dispersion was higher in A-MVP treated with an ICD compared with A-MVP with ComVE (mean 67 vs 56 ms, p=0.078).
Discussion
In the current investigation, we demonstrate that increased STE-derived mechanical dispersion is associated with a higher prevalence of arrhythmic complications in patients with MVP. This association is independent of LV systolic function, degree of MR and the presence of bileaflet MVP. Prior investigations have focused on the bileaflet phenotype and the mechanistic hypothesis of focal myocardial traction/fibrosis as the primary determinant of malignant ventricular arrhythmia. In some studies of arrhythmic MVP, monoleaflet MVP cases were completely excluded, leading to selection bias.10 In our study, however, MVP patients with all types of leaflet involvement (including anterior and posterior) were included, reflecting true clinical scenarios where complex ventricular ectopy or need for ICD do not occur only in bileaflet MVP.
Despite the evidence of focal or replacement fibrosis in the papillary muscles or inferolateral base in some arrhythmic MVP cases, the mechanism of arrhythmia in MVP is typically not re-entry. Triggered activity with delayed afterdepolarisations is more commonly observed in MVP, a mechanism also seen in long QT syndrome, a condition co-existent with MVP in some cases.17 Moreover, triggered activity with early afterdepolarisations can occur when normal cell-to-cell coupling is disrupted in the setting of diffuse or interstitial fibrosis.18 This pattern of fibrosis has been demonstrated using T1 mapping CMR in arrhythmic MVP, often in the absence of focal fibrosis by late gadolinium enhancement and even without significant MR.9 19 Finally, on electrophysiology studies of arrhythmic MVP, premature ventricular complexes and ventricular tachycardia can arise from sites other than the LV papillary muscles or basal inferolateral wall previously associated with focal fibrosis on CMR. Additional arrhythmogenic foci include the fascicles, the right/left ventricular outflow tracts, the septal aspect of the mitral annulus and the basal anterolateral wall.7 10
The imaging and electrophysiological findings described point to a diffuse, possibly primary myocardial process that goes beyond the mechanistic theory of focal papillary muscle traction as a unique explanation for malignant arrhythmias in MVP. Furthermore, histological studies have demonstrated diffuse myocardial fibrosis in a small subgroup of patients with sudden cardiac death without clear structural heart disease.20 An underlying primary diffuse myocardial process may explain why some but not all individuals with MVP-related significant MR die suddenly or why not all MVP with a cardiac arrest have bileaflet MVP with focal myocardial fibrosis. Hence, global rather than segmental parameters of myocardial function may be better suited to highlight a diffuse myocardial involvement in MVP. Mechanical dispersion or heterogeneous contraction is a global strain parameter reflective of electrical dispersion. In our MVP study, mechanical dispersion is a better predictor of arrhythmic risk compared with other traditional ‘focal’ parameters such as mitral annular disjunction, which was not significantly different in univariate analysis between A-MVP and NA-MVP and bileaflet MVP, which was dropped from the multivariate model. Bileaflet involvement was the only significant predictor of arrhythmic risk in a smaller multivariate model inclusive of degree of MR but not mechanical dispersion. However, when mechanical dispersion was introduced into the model the association between bileaflet MVP and ventricular arrhythmia was no longer statistically significant. Similar values of mechanical dispersion between NA-MVP and controls further suggest that heterogeneous contraction and electrical dispersion specifically characterise arrhythmic but not all MVP subjects.
Although the majority of MVP patients in our samples had less than moderate MR, we did not exclude the 18 patients with moderate or severe MR in order to avoid selection bias. Despite inclusion of such cases, the association of mechanical dispersion with risk of ventricular tachycardia or sudden cardiac arrest was independent of degree of MR. These findings suggest that a primary rather than a secondary or MR-related myopathy may be responsible for arrhythmic complications in MVP.
Abnormal mechanical dispersion has been described in other arrhythmogenic conditions such as ischaemic, dilated and hypertrophic cardiomyopathies, and arrhythmogenic right ventricular cardiomyopathy. In hypertrophic cardiomyopathy, mechanical dispersion has been linked with the degree of diffuse myocardial fibrosis by T1 mapping CMR.12 Interestingly, mechanical dispersion has also been shown to be increased in long QT syndrome, a condition co-segregating with MVP as noted above.17 In our sample, the QTc interval was greater in MVP compared with controls, although was similar in A-MVP versus NA-MVP.
A previous study has examined strain parameters of early systolic shortening and postsystolic stretch in MVP.16 The group showed that these parameters were significantly different between MVP and controls when averaged over all myocardial segments, with differences more prominent in the lateral and basal segments. However, when patients with palpitations and ECG abnormalities were compared with individuals without this presentation, regional abnormalities were not significantly different. Overall, mechanical dispersion as a global measure of heterogeneous contraction may be easier to use as an arrhythmic risk predictor compared with the segmental strain parameters described. Because segmental parameters depend on the time during systole, the type of leaflet involvement and the degree of MR,16 their use may not be easily applicable to everyday clinical flow.
GLS, a measure of overall longitudinal contraction of the myocardium was slightly lower in the overall MVP group compared with controls. This difference was borderline statistically significant and was likely driven by the higher number of subjects with MR in the MVP group. GLS was similar between A-MVP and NA-MVP in univariate analysis. This finding may be related to the fact that GLS is an average measurement of peak strain and may not reflect the complex temporal relationships between different myocardial segments.
Strengths and limitations
This study supports our hypothesis that greater mechanical dispersion is associated with a higher prevalence of ventricular arrhythmia in MVP. To our knowledge, this study is the first to investigate the role of mechanical dispersion in arrhythmic risk stratification for MVP. Moreover, we examined consecutive arrhythmic MVP patients irrespective of leaflet involvement or degree of MR to avoid selection bias and better reflect true clinical scenarios.
There are several noteworthy limitations to our study. First, the modest sample size may have impacted the statistical significance of certain comparisons. Additionally, the small number of A-MVP subjects limited our ability to include all potential predictors of ventricular arrhythmia in our multivariate model. Second, given that the minority of our patients had an aborted cardiac arrest, we used the presence of complex ventricular ectopy (inclusive of ventricular tachycardia) as a surrogate for arrhythmic MVP. This may have led to increased heterogeneity within our cohort, however A-MVP with ICD placement for aborted cardiac arrest had the highest mechanical dispersion, suggesting a gradation of mechanical dispersion in the highest risk patients. Third, CMR data were not included in our investigation as CMRs were clinically available only in five A-MVP but not in NA-MVP subjects. Fourth, we used an off-line strain-analysis system which is based on an 18 segment rather than the 16 segment model used in other analytical packages (General Electrics).13 17 Although this system will need to be tested in a different population, the fact that all MVP patients and controls were analysed using the same software assures that our findings are accurate within our study population. Finally, our study is retrospective. Hence, the ability of mechanical dispersion to assess the risk of ventricular arrhythmia in a longitudinal fashion is unclear. Given the above limitations, our findings are preliminary and require the confirmation in larger prospective multicentre studies.
Conclusions
Increased STE-derived mechanical dispersion may help identify MVP patients at higher risk for ventricular arrhythmia. The association between mechanical dispersion and MVP-related arrhythmic complications is independent of LV systolic function, degree of MR and type of leaflet involvement. Further studies are needed to correlate increased mechanical dispersion with myocardial fibrosis in MVP.
Key messages
What is already known on this subject?
Patients with mitral valve prolapse (MVP) are known to be at higher risk for ventricular arrhythmias, especially those with myocardial fibrosis on cardiac magnetic resonance imaging (CMR).
Mechanical dispersion by speckle-tracking echocardiography is a global strain parameter reflective of electrical dispersion previously evaluated in other arrhythmogenic cardiomyopathies but never studied in MVP.
What might this study add?
We demonstrate that increased mechanical dispersion is associated with a higher prevalence of arrhythmic complications in MVP.
This association is independent of left ventricular systolic function, degree of mitral regurgitation and type of leaflet involvement.
How might this impact on clinical practice?
Mechanical dispersion by speckle-tracking echocardiography may become an additional and readily obtainable marker of arrhythmic risk in MVP.
Further studies are needed to correlate increased mechanical dispersion with myocardial fibrosis in MVP.
References
Footnotes
Contributors SE: design of the study, analysis and interpretation of data, manuscript drafting. RG: analysis and interpretation of data, manuscript drafting. LL: identification of study patients, manuscript drafting. DB: acquisition of echocardiographic images, manuscript editing. QF: statistical analysis of data, manuscript editing. GN: statistical analysis of data, manuscript editing. TPA: conception of the study, critical manuscript revision for important intellectual content. NBS: conception of the study, critical manuscript revision for important intellectual content. FD: conception and design of the study, review of the data and their analysis, critical manuscript revision.
Funding This work was supported by research grant NIH K23HL116652, NIH R03HL145238 and by the UCSF Senate Resource Allocation Program (FND).
Competing interests None declared.
Ethics approval The study was approved by the University of California, San Francisco Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.