Article Text

Abstract
Objective In patients with myocardial infarction (MI), risk factors for bleeding and ischaemic events tend to overlap, but the combined effects of these factors have scarcely been studied in contemporary real-world settings. We aimed to assess the combined associations of established risk factors using nationwide registries.
Methods Using the Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies registry, patients with invasively managed MI in 2006–2014 were included. Six factors were assessed in relation to cardiovascular death (CVD)/MI/stroke, and major bleeding: age ≥65, chronic kidney disease, diabetes, multivessel disease, prior bleeding and prior MI.
Results We studied 100 879 patients, of whom 20 831 (20.6%) experienced CVD/MI/stroke and 5939 (5.9%) major bleeding, during 3.6 years median follow-up. In adjusted Cox models, all factors were associated with CVD/MI/stroke, and all but prior MI were associated with major bleeding. The majority (53.5%) had ≥2 risk factors. With each added risk factor, there was a marked but gradual increase in incidence of the CVD/MI/stroke. This was seen also for major bleeding, but to a lesser extent, largely driven by prior bleeding as the strongest risk factor.
Conclusions The majority of patients with MI had two or more established risk factors. Increasing number of risk factors was associated with higher rate of ischaemic events. When excluding patients with prior major bleeding, bleeding incidence rate increased only minimally with increasing number of risk factors. The high ischaemic risk in those with multiple risk factors highlights an unmet need for additional preventive measures.
- risk factors
- acute coronary syndromes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Despite recent advances in treatment, patients with myocardial infarction (MI) are still at increased risk for subsequent ischaemic events and mortality. To reduce ischaemic risk, potent dual antiplatelet therapy (DAPT) is employed,1 2 where recent evidence also supports long-term DAPT with ticagrelor3 and long-term low-dose anticoagulation with rivaroxaban in addition to aspirin.4 While reducing ischaemic events, dual inhibition with antiplatelet or anticoagulation is also associated with increased bleeding risk.1–4
In previous studies, risk factors for ischaemic and major bleeding events tend to overlap and major bleeding risk has been difficult to isolate. For instance, in the DAPT score, which attempted to find a balance between ischaemic and major bleeding risk, the only bleeding-specific marker was age (in a population who had already endured 1 year DAPT).5 Key risk factors frequently used as risk enrichment criteria in clinical trials3 4 include multivessel disease (MVD),6 diabetes mellitus,7 chronic kidney disease (CKD),8 prior MI9 and higher age.10
We assessed the combined association of these risk factors in a large contemporary real-world population using nationwide registries, to see how different combinations of these factors influence the incidence of recurrent ischaemic events and bleeding.
Methods
This study was based on data from the Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies (SWEDEHEART) registry. All cardiac care units in Sweden are connected to the registry, and all coronary angiograms and percutaneous coronary intervention procedures performed in the country are registered. Data entry is achieved through a web-based interface, and data are monitored by random checks of source data, with a high reported agreement (96%).11
We combined data from SWEDEHEART with the Swedish National Patient Register that includes all hospitalisations in Sweden, and the Cause of Death Register.
Study population
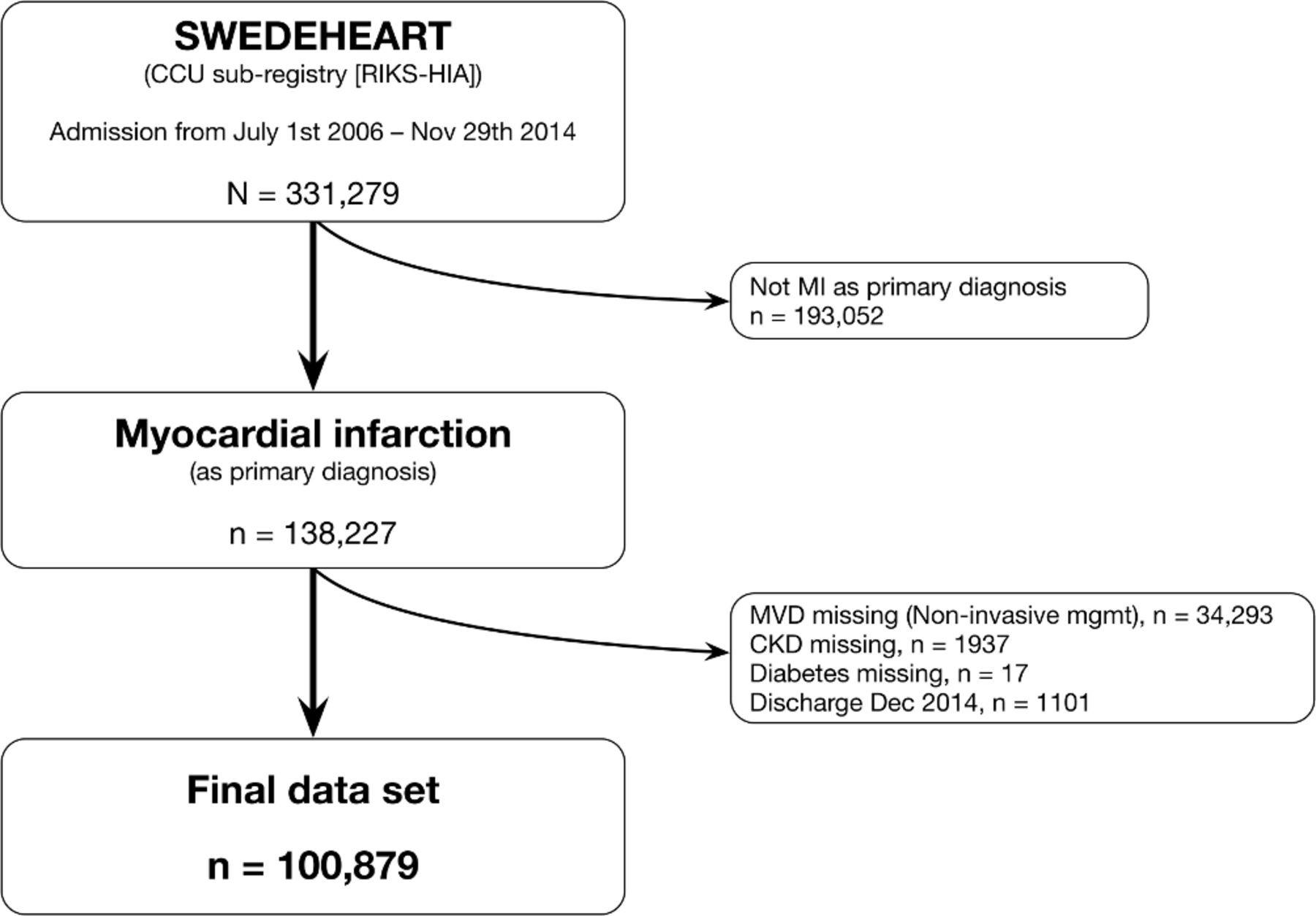
During the study period, 2006–2014, there were 103 934 individuals admitted for MI and managed invasively with coronary angiography (figure 1). Of these, a total of 3055 (2.9%) individuals had missing information in one or more of the risk factors studied and were excluded, yielding a study population of 100 879 individuals. Given the small proportion with missing values, we conducted complete case analyses without any attempts of imputation.

Selection of study population. CCU, cardiac care unit; CKD, chronic kidney disease; MI, myocardial infarction; MVD, multivessel disease; SWEDEHEART, Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies; RIKS-HIA, Swedish Register of Information and Knowledge about Swedusg Heart Intensive Care Admissions.
Risk factors
The following risk factors were selected a priori based on their previously strong associations with outcomes in patients with MI and because of their use as enrichment criteria in clinical trials3: age ≥65, MVD (defined as two or more vessels or left main with a stenosis ≥50% at coronary angiography), CKD (defined as an estimated glomerular filtration rate below 60 mL/min/1.73 m2 calculated by the CKD-Epidemiology Collaboration formula), diabetes mellitus, prior MI (previous International Classification of Diseases 10th Revision [ICD-10] diagnosis I21–I23) and prior major bleeding (using the same ICD-10 codes as below).
Outcomes
The primary outcome was the composite of MI, stroke and cardiovascular death (CVD). As secondary analyses, we assessed each component individually. MI was defined as a rehospitalisation with an ICD-10 diagnosis of I21–I23, stroke as an ICD-10 diagnosis of I60–I64 (ie, including both ischaemic and bleeding strokes, to use a definition that as closely as possible resembles that of most randomised controlled trials in ischaemic heart disease1–3) and CVD as death with a primary cause in the I chapter of ICD-10. Major bleeding was defined as previously described by Friberg and Skeppholm12; including hospitalisation for intracranial (ICD-10 I60–I62, S064–S066), gastrointestinal (K25–K28, K22.6, K29.0, K62.5, K66.1, K92.0–K92.2, I85.0, I93.8), urogenital (N02, R31.9, N93.9, N95.0, N501A) or other bleeding (H11.3, H13.3, H35.6, H43.1, H45.0, H92.2, I31.2, J94.2, M25.0, T81.0, D50.0, D62.9, R04, R58).
Statistical analysis
Patient characteristics are reported as frequencies and percentages for categorical variables, and as median (IQR) for continuous variables.
Unadjusted Kaplan-Meier risks (%) for the primary and secondary outcomes are plotted for each risk factor. Differences in unadjusted risk in relation to each risk factor were assessed with the log-rank test. As sensitivity analyses, we also assessed outcomes from a landmark at 1 year, and performed analyses where ischaemic events also were censored by bleeding events (in addition to death and end of follow-up) and bleeding events similarly censored also by ischaemic events.
Cox proportional hazards models were fitted for the primary composite outcome and major bleeding, respectively; both unadjusted models and models adjusting for the other risk factors (age ≥65, CKD, diabetes mellitus, MVD, prior MI, prior major bleeding) as well as sex. Results are presented as HRs with 95% CIs. The proportional hazards assumption was assessed by visual inspection of the Schoenfeld residuals without any indication of violation of this assumption. Competing risk models (Fine-Gray) were fitted as sensitivity analyses.
Frequencies of patients having combinations of risk factors are presented as an UpSet plot (limited to risk factor combinations with at least 30 patients), and the incidence rates per 100 person-years of the ischaemic composite endpoint and major bleeding across these combinations of risk factors are shown in scatter plots. In addition, the incidence rates for these outcomes are reported in tabular form in the online supplementary material.
All analyses were conducted using R V.3.3.1 and V.3.5.1; with the ggplot2, UpSetR and survsup packages used for visualisation.
Results
Baseline characteristics are shown in table 1. In the 100 879 patients who had invasively managed MI, 20 831 (20.6%) experienced CVD/MI/stroke and 5939 (5.9%) major bleeding during a median follow-up of 3.6 years. Overall, 31% of patients were women, but with increasing number of risk factors, an increasing proportion of patients were women, with 39.6% women in the subset of patients with all six risk factors (online supplementary table S1).
Supplemental material
Baseline characteristics and discharge medications
Event rates in relation to single risk factors
In figures 2 and 3, the cumulative incidences of CVD/MI/stroke and bleeding are shown (for CVD alone see online supplementary figure S1). While the risk of major bleeding events was substantially lower than for ischaemic events, all of the assessed risk factors were associated with an increased risk of both ischaemic events and bleeding events (p<0.001 for all). This was consistently seen in a landmark analysis (assessing events from 1 year onwards in patients who were event free up until that time; online supplementary figure S2), and in additional sensitivity analyses where ischaemic events were censored by major bleeding (in addition to death and end of follow-up), and bleeding events were censored by ischaemic events (in addition to death and end of follow-up; online supplementary figures S3 and S4). In a sensitivity analysis of patients with atrial fibrillation (representing 6.6% of the population), patterns of event rates in relation to risk factors for both CVD/MI/stroke and major bleeding were similar as in the full population (data not shown).

CVD/MI/stroke: Kaplan-Meier estimates of CVD/MI/stroke in relation to risk factors. CKD, chronic kidney disease; CVD, cardiovascular death; MI, myocardial infarction; MVD, multivessel disease.
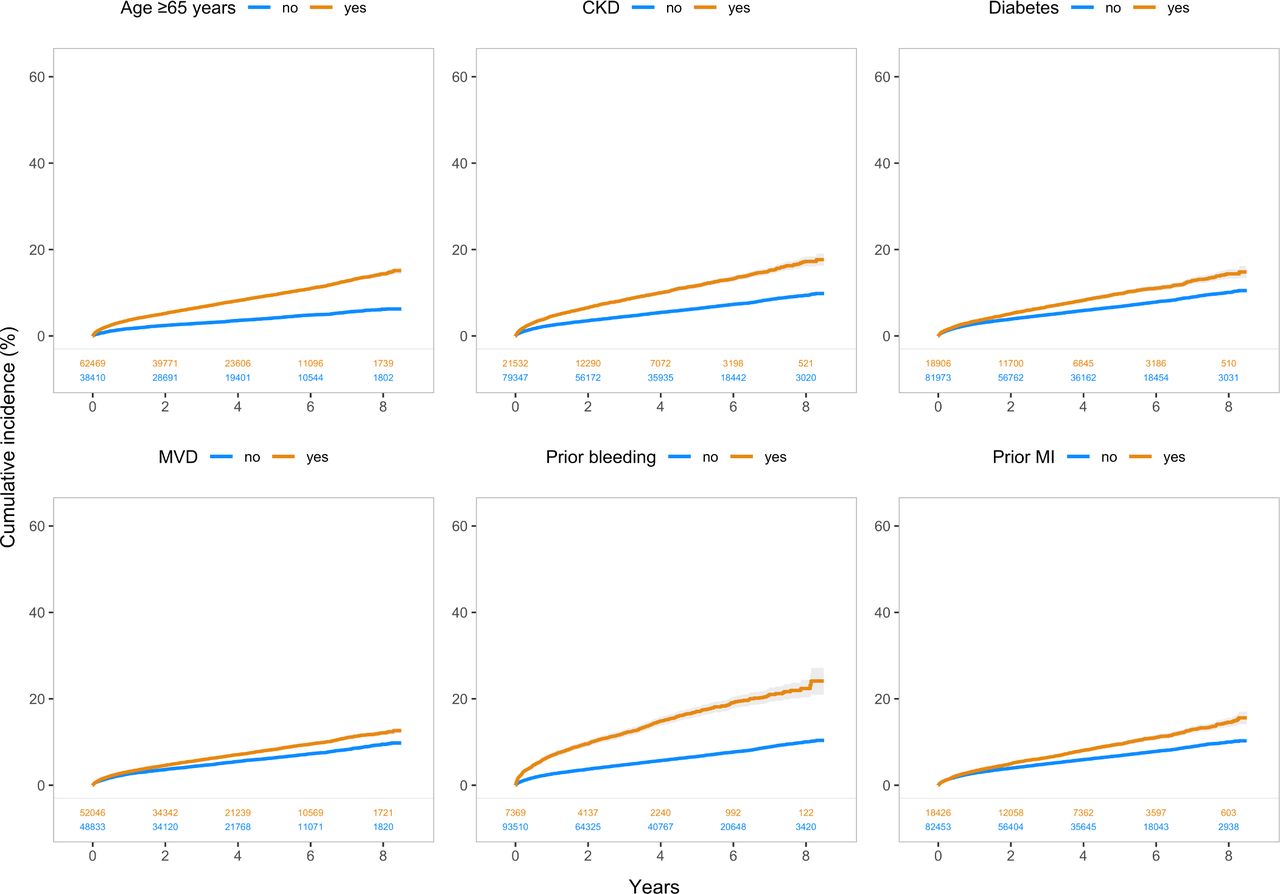
Major bleeding: Kaplan-Meier estimates of major bleeding in relation to risk factors. CKD, chronic kidney disease; MI, myocardial infarction; MVD, multivessel disease.
Cox models
In the adjusted Cox models, all six risk factors were associated with CVD/MI/stroke and all risk factors but prior MI were associated with bleeding (table 2). However, the HRs were closer to 1 for bleeding events than for ischaemic events for all factors but age and prior bleeding, showing higher HR for bleeding than for ischaemic events. In sensitivity analyses by competing risk models, these estimates remained similar (online supplementary table S2).
Cox proportional hazards models
Event rates in relation to combinations of risk factors
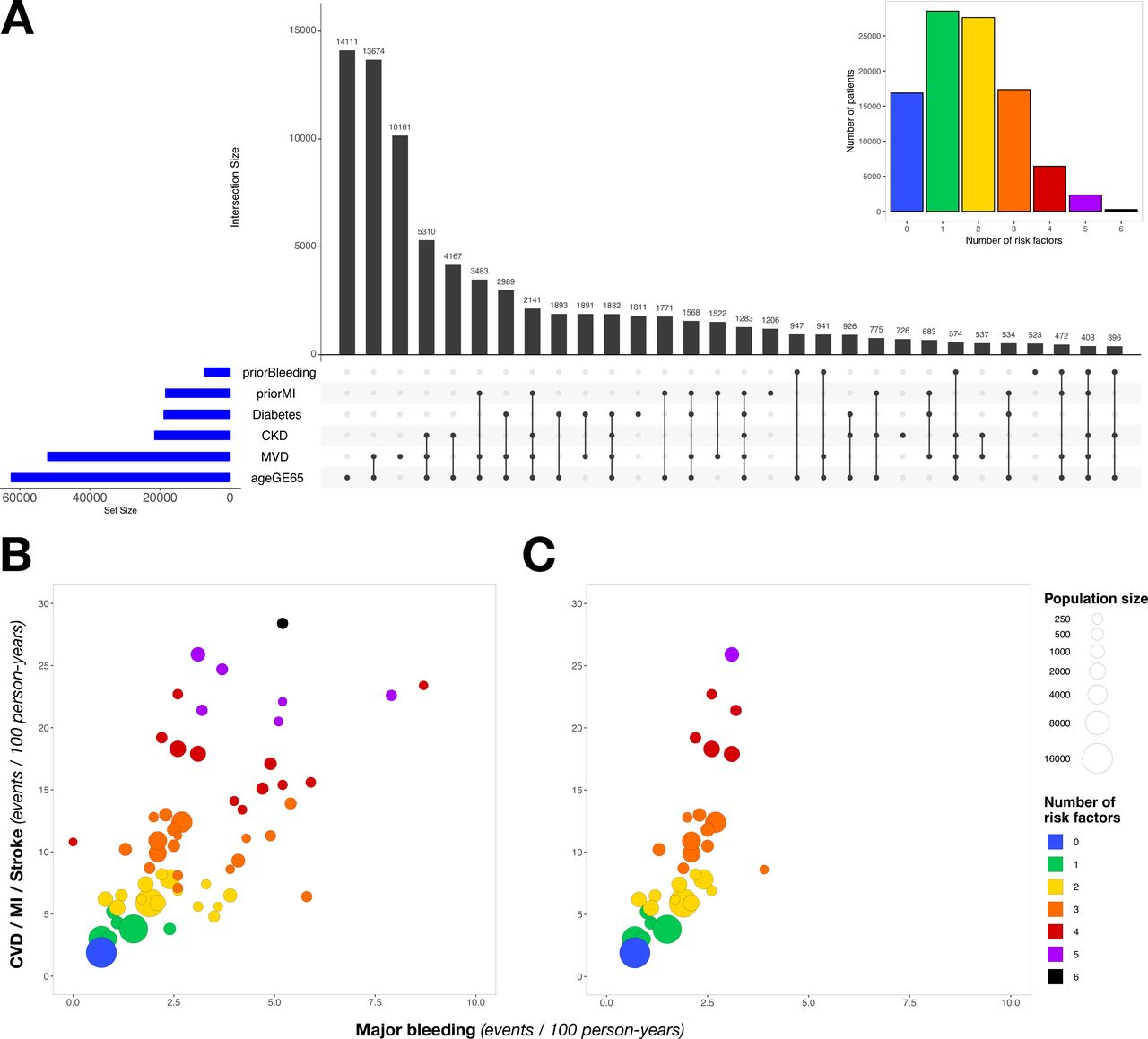
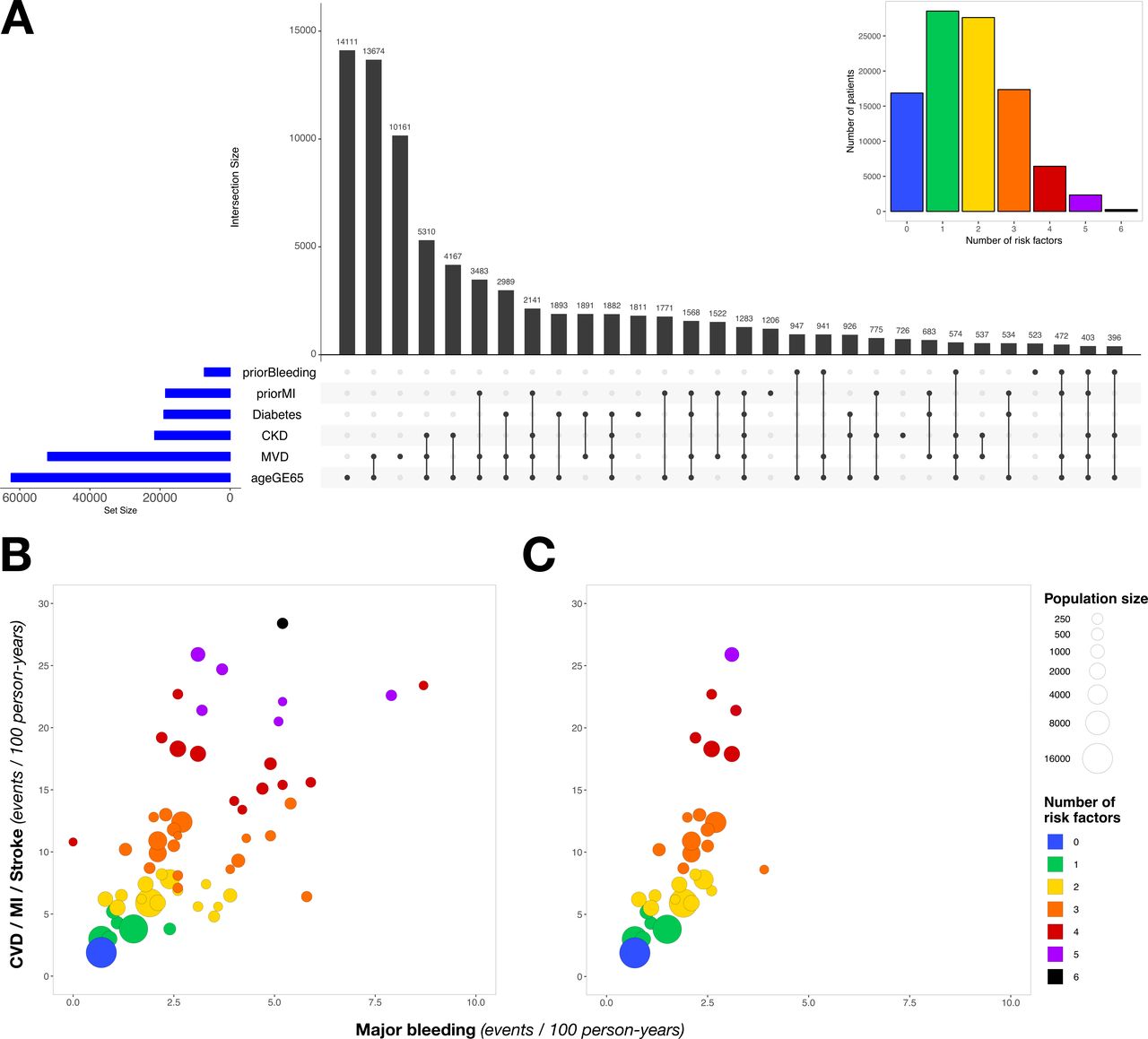
Combinations of risk factors are shown in figure 4A (includes combinations with at least 30 patients; for all possible combinations, see supplementary figure S5). The majority of patients (53.5%) had two or more risk factors, while 17 969 patients (18%) did not have any risk factor. Incidence rates per 100 person-years for CVD/MI/stroke and bleeding for these combinations are shown in figure 4B,C, tables 2 and 3 and in the online supplementary table S3. With each added risk factor, there was a marked but gradual increase in incidence rate of the composite endpoint (figure 4B). This was also seen for bleeding, but to a lesser extent and largely driven by prior bleeding as the strongest risk factor. When assessing patients who had no prior bleeding, increasing number of risk factors remained associated with a substantial increase in incidence rate for ischaemic outcomes, while bleeding incidence rate increased only minimally with increasing number of risk factors (figure 4C).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Combinations of risk factors and incidence of ischaemic and bleeding events. Panel (A) shows combinations of risk factors (in patients with at least one risk factor). Each black bar represents a combination of risk factors and indicates how many patients have that specific combination. The dots below the black bars indicate which risk factors are present in that group. The blue bars represent the total number of patients having each risk factor. The coloured inset (top right) shows the distribution of risk factor counts in the population. In panel (B) the incidence rates for major bleeding (X axis) and CVD/MI/stroke (Y axis) in relation to combinations of risk factors are shown (lines indicate 95% confidence intervals). In panel (C) the risk factor combinations that do not include prior bleeding are highlighted. (Panels A–C [except inset] include risk factor combinations with at least 30 patients.) CKD, chronic kidney disease; CVD, cardiovascular death; GE, greater than or equal to; MI, myocardial infarction; MVD, multivessel disease.
Incidence rates of CVD/MI/stroke and major bleeding across different combinations of risk factors excluding prior bleeding
In patients who did not have prior bleeding, the incidence rates for CVD/MI/stroke were generally severalfold higher than for major bleeding (table 3), with CKD, with the highest rates of CVD/MI/stroke in those with a large number of risk factors. In patients with prior bleeding the incidence rates for ischaemic events were similarly high in those with multiple risk factors, but the incidence rates for major bleeding were generally substantially higher than in those without prior bleeding (table 4).
Incidence rates of CVD/MI/stroke and major bleeding across different combinations including prior bleeding
Discussion
In this study, we assessed the combined association of key risk factors on ischaemic and bleeding events. We show that a majority of patients in a real-world setting have two or more risk factors. In addition, increasing number of risk factors is associated with increasing rates of ischaemic events, and to a lesser degree also with bleeding events. When excluding patients with prior bleeding, bleeding incidence rate was low and increasing number of risk factors was associated only with minimal increase in bleeding incidence rate, whereas an increasing number of risk factors were associated with a marked increase in ischaemic events.
All risk factors assessed represent chronic conditions that influence long-term risk. The substantially higher incidence rate of ischaemic events in those with multiple risk factors compared with only a single risk factor suggests an unmet need for additional preventive measures, possibly with prolonged DAPT3 or anticoagulation with rivaroxaban.4 In patients with established coronary heart disease revascularised with drug-eluting stents, prolonged DAPT (30 months vs 12 months) reduced the risk of ischaemic events, but increased the risk of major bleeding.13 Similarly, the Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared with Placebo on a Background of Aspirin–Thrombolysis in Myocardial Infarction 54 (PEGASUS-TIMI 54) trial demonstrated that long-term ticagrelor treatment, as compared with placebo, reduced the risk of CVD, MI or stroke, but increased the risk of major bleeding.3 Although a similar relative benefit was observed with ticagrelor over placebo in a substudy of patients included in PEGASUS-TIMI 54 with and without MVD, those with MVD had a greater absolute risk reduction and the number needed to treat tended to be lower.14
Recent evidence suggests that our current classification of type 2 diabetes is quite coarse. In a data-driven cluster analysis of patients with type 2 diabetes, five distinct replicable clusters of patients could be identified, with differing risk of diabetic complications and course of the disease.15 Increasing knowledge about such subgroups, and specific studies of improved phenotyping of diabetes in the setting of manifest coronary heart disease are warranted.
CKD is also a well-established risk factor for cardiovascular disease, however often overlooked, where there is a progressive increase in risk for cardiovascular mortality by decreasing renal function.8
About 7% of patients in our study had a history of major bleeding as an inpatient diagnosis, which was the strongest predictor of new major bleeding. This is in line with the Predicting Bleeding Complication in Patients Undergoing Stent Implantation and Subsequent Dual Antiplatelet Therapy (PRECISE-DAPT) score, recommended by current guidelines for assessing bleeding risk,16 in which prior bleeding also was the strongest bleeding predictor.17 While improved outcomes by using bleeding risk scores in this setting have not been demonstrated in prospective randomised trials, guidelines reflect that it may be reasonable with a shorter DAPT duration in those with high bleeding risk, and consequently, a prolonged DAPT duration in most patients in whom the bleeding risk is estimated to be low.16 When we in this study excluded patients with prior bleeding, the incidence rate of major bleeding remained low, with only minimal absolute increases with increasing number of other risk factors. Thus, by excluding patients with prior bleeding events from prolonged potent antithrombotic strategies a greater tolerability for these therapies can be expected. Our findings suggest that although risk scores and even biomarkers (eg, Growth Differentiation Factor-1518) could provide more precise estimates of bleeding risk, absence of prior bleeding in patients with multiple risk factors could be considered reassuring in terms of risk/benefit balance of more intense treatment.
Taken together, the findings from our study highlight that a majority of patients with acute coronary syndrome in a real-life setting have multiple risk factors, which increase the risk of subsequent events. Although overlap between ischaemia and bleeding is evident, increasing number of risk factors is associated with higher incidence rate of ischaemia than bleeding, and when excluding patients with prior bleeding, increasing number of risk factors is associated with a marked increase in ischaemic incidence rate, while bleeding incidence rate remains quite similar. As such, the risk-benefit balance will be different in patients with different risk factor profiles, and given recent and coming treatment options for these risk factors, there is potential to address this unmet need to further improve long-term outcomes in patients with MI by personalised treatment.
Limitations
There are limitations with this study. Events were captured based on ICD codes from national registries. While this allows for virtually no loss of follow-up, events were not adjudicated (however, the validity of diagnoses in the Swedish National Patient Register is high19), and only includes diagnoses made during hospitalisations. Therefore, less severe bleeding events not requiring hospitalisation were not captured. We studied a limited number of key risk factors based on their previously reported strong association with outcomes and their use as risk enrichment in randomised controlled trials. This is by no means exhaustive, and it is acknowledged that other risk markers could be of value, including history of peripheral arterial disease and circulating biomarkers.
Conclusions
The majority of patients with MI had two or more established risk factors. An increasing number of risk factors were associated with higher incidence of ischaemic events. When excluding patients with prior major bleeding, bleeding incidence rate was low and increased only minimally with increasing number of risk factors. The higher incidence rate of ischaemic events in those with multiple risk factors highlights an unmet need for additional preventive measures.
Key messages
What is already known on this subject?
Risk factors for bleeding and ischaemic events tend to overlap, but the combined associations have scarcely been studied in a real-world nationwide contemporary cohort.
What might this study add?
This study explores the combination of these risk factors and how these associate with ischaemic and bleeding outcomes. A majority (53.5%) had two or more risk factors. Increasing number of risk factors is associated with increasing rates of both ischaemic events and bleeding. When assessing only patients without prior bleeding, increasing number of risk factors was still associated with increasing rates of ischaemic events (with an incidence of 25.9 [95% CI 24 to 27.9] per 100 person-years in the group with the highest incidence of ischaemic events), whereas bleeding event rate remained low (incidence of 3.9 [95% CI 1.7 to 7.6] per 100 person-years in the group with the highest bleeding incidence).
How might this impact on clinical practice?
These findings highlight the importance of assessing patient bleeding history, which could have implications in decisions regarding intensity and duration of secondary preventive treatment.
References
Footnotes
Contributors Conception and design: DL, DE, BS, LPH, MJ, TJ, SKJ. Analysis and interpretation of data: DL, DE, BS, LPH, MJ, TJ, SKJ. Drafting the article: DL. Revising the article: DL, GS, DE, BS, LPH, MJ, TJ, SKJ. Provided intellectual content of critical importance to the work described: all authors. Final approval of the version to be published: all authors.
Funding This study was supported by AstraZeneca.
Competing interests DL reports being an employee at Uppsala University and affiliated with Uppsala Clinical Research Center during the time this work was conducted, but has since been employed by AstraZeneca. BS reports institutional research grants from AstraZeneca, Novartis and Abbott. LPH reports being employed by AstraZeneca. MJ reports lecture fees from AstraZeneca and Pfizer. TJ has received consultant and lecture fees from AstraZeneca, MSD and Aspen. SKJ reports institutional research grants from AstraZeneca.
Ethics approval The study was approved by the Ethics Committee in Uppsala.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data supporting the conclusions in this article and additional data are available upon request. Please contact the corresponding author.
Patient consent for publication Not required.