Article Text

Abstract
Objective Long-term prognosis of patients with coarctation of the aorta (CoA) is impaired due to the high prevalence of hypertension and consequent cardiovascular complications. Although stent implantation results in acute anatomical and haemodynamic benefit, limited evidence exists regarding the late clinical outcome. In this meta-analysis, we aimed to evaluate the medium-term effect of stent placement for CoA on systemic blood pressure (BP).
Methods PubMed, EMBASE and Cochrane databases were searched for non-randomised cohort studies addressing systemic BP ≥12 months following CoA stenting. Meta-analysis was performed on the change in BP from baseline to last follow-up using a random-effects model. Subgroup analyses and meta-regression were conducted to identify sources of heterogeneity between studies.
Results Twenty-six studies with a total of 1157 patients and a median follow-up of 26 months were included for final analysis. Meta-analysis showed a 20.3 mm Hg (95% CI 16.4 to 24.1 mm Hg; p<0.00001) reduction in systolic BP and an 8.2 mm Hg (12 studies; 95% CI 5.2 to 11.3 mm Hg; p<0.00001) reduction in diastolic BP. A concomitant decrease in the use of antihypertensive medication was observed. High systolic BP and peak systolic gradient at baseline and stenting of native CoA were associated with a greater reduction in systolic BP at follow-up.
Conclusions Stent implantation for CoA is associated with a significant decline in systolic and diastolic BP during medium-term follow-up. The degree of BP reduction appears to be dependent on baseline systolic BP, baseline peak systolic gradient, and whether stenting is performed for native or recurrent CoA.
- aortic coarctation
- endovascular procedures for aortic and vascular disease
- hypertension
- meta-analysis
Statistics from Altmetric.com
Introduction
Coarctation of the aorta (CoA) is a congenital narrowing of the thoracic aortic lumen and accounts for approximately 5%–7% of all patients with congenital heart disease.1 Although the majority of patients undergo successful surgical repair in early childhood, systemic hypertension remains an important concern with a prevalence reported up to 60% during long-term follow-up.2 Consequently, the prognosis of CoA patients is reduced due to hypertension-related complications, including accelerated coronary artery disease, heart failure, aneurysm formation and stroke.3 Although the presence of residual obstruction is an important substrate for hypertension, many hypertensive CoA patients show no evidence of recurrent stenosis. Hence, the underlying cause of hypertension in this population remains subject of debate. It has been reported that abnormal aortic arch geometry, particularly a hypoplastic or gothic arch, is associated with hypertension.4 Additionally, the presence of a generalised vasculopathy, reduced aortic wall distensibility, altered blood flow patterns and impaired baroreceptor sensitivity have been suggested as predisposing factors for persistent hypertension.5 6
Over the last decades, stent implantation by transcatheter approach has replaced surgical repair as the treatment of choice for adolescents and adults with native CoA, since it is associated with fewer acute complications compared with surgery, while short-term haemodynamic outcomes are comparable.7 Furthermore, stenting is preferred in adults with discrete, recurrent CoA.8 Although stent implantation has shown to effectively reduce aortic gradient with favourable anatomical results, there is uncertainty concerning the late effects on blood pressure (BP) and adverse cardiovascular events.9 10 To date, only a limited number of studies with significant heterogeneity in population characteristics and follow-up duration have addressed this issue.10–12 Recent evidence indicates that in particular the systolic BP (SBP) is predictive of cardiovascular risk in young and middle-aged adults.13 Consequently, the primary aim of this meta-analysis was to elucidate the effect of stent placement on medium-term SBP in patients with CoA. Second, we sought to identify parameters influencing this effect of stenting in CoA.
Methods
Search strategy and study selection
This meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.14 PubMed, EMBASE and Cochrane Library were searched for non-randomised cohort studies reporting on mean SBP at baseline and at least 12 months after stent implantation, using keywords related to aortic coarctation, stent implantation and BP. The exact search terms used are provided in online supplementary methods S1. Additionally, ClinicalTrials.gov, WHO ICTRP, Google Scholar and OpenGrey were searched for unpublished trials and grey literature. No restrictions regarding language and year of publication were applied. We excluded case reports, reviews, (editorial) comments, animal studies and studies evaluating the outcomes of stenting as a bridging strategy to subsequent surgical intervention. Two authors (TAM, EW) independently screened all titles and abstracts of articles identified by the initial search and then reviewed the full text of potentially relevant articles. Any discrepancies were resolved by discussion with a third study member (MV). Reference lists of selected studies were manually searched to identify other eligible studies.
Supplemental material
Assessment of certainty of evidence
The outcomes change in SBP and change in diastolic BP (DBP) were assessed on certainty of evidence by two independent reviewers (TAM, EW) using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach.15 GRADE criteria included risk of bias, inconsistency, indirectness and imprecision. Risk of bias assessment of individual studies was based on the criteria for observational studies as described in the GRADE guidelines (online supplementary table S1).16 Control of potential confounding factors was evaluated, including the change in use of antihypertensive medication (AHM), restenosis and/or reintervention for CoA during follow-up, change in body mass index and other secondary causes of hypertension (primary hyperaldosteronism, renal artery stenosis, chronic renal disease and obstructive sleep apnoea).
Data extraction
Data from the eligible studies were extracted by one researcher (TAM) using prespecified forms and subsequently confirmed by a second study member (EW). Variables included first author, title, year of publication, study design, number of subjects, gender, age at stent implantation, type of CoA (native or recurrent), peak systolic gradient (PSG) preintervention and directly postintervention, average follow-up duration, mean SBP and DBP, prevalence of hypertension and the use of AHM. PSG measurements were only extracted when measured invasively during cardiac catheterisation. BP data were recorded prior to stent implantation, during follow-up and at last follow-up. The prevalence of hypertension was recorded according to the definition of hypertension used in a particular study. When necessary, authors of the studies were contacted for additional data.
Statistical analysis
For the description of individual study characteristics, dichotomous variables are expressed as percentages and continuous variables as mean or median, depending on the description used in the study. Distributions across studies are shown as median and range. For pooled analysis, the absolute change in SBP and DBP from baseline to last follow-up and 95% CIs were used. This effect size metric was considered clinically relevant, as absolute reductions in SBP and DBP have shown to be highly associated with a reduction in adverse cardiovascular events.17 In contrast, the change in prevalence of hypertension was not considered an appropriate outcome measure, since definitions of hypertension may vary across studies, reference values for children and adults differ, and dichotomising BP values may result in bias and loss of information.18 When the SD of BP change was missing, this was calculated using the corresponding p value. A conservative approach was applied regarding non-exact p values, for example, <0.05, by using the upper limit for analysis. When no p value was provided, an imputed correlation coefficient was used according to the Cochrane Handbook for Systematic Reviews of Interventions section 16.1.3.2.19 As the outcome may have been affected by the used material, technique of the operator and the age of participants, we expected the effect size to vary between studies. Therefore, a random-effects model was used. The inverse of the variance was used to weigh individual studies. Heterogeneity was assessed using the I2 statistic and judged as substantial when I2 >50%.20 However, I2 should be interpreted in relation to the sample size of included studies, as I2 may increase with larger studies. To examine possible sources of between-study heterogeneity and to identify potential effect modifiers, subgroup analyses on SBP change were performed. The prespecified selection of subgroup variables was based on clinical and methodological characteristics identified by previous studies and considered relevant by the authors. These included gender, age, native versus recurrent CoA, baseline SBP, baseline and poststenting PSG, change in AHM use, follow-up duration, study design, publication year, method of BP measurement and incomplete follow-up. The impact of potential effect modifiers was further explored by bivariate random-effects meta-regression. Sensitivity analyses were conducted to assess the robustness of the overall effect on SBP by using a fixed-effects model and by subsequently leaving one study out of the meta-analysis. To identify potential publication bias, a funnel plot was created, which was visually inspected and quantified on asymmetry by the Egger’s test. The ‘trim and fill’ method was used to adjust for potential publication bias.21P values <0.05 were considered statistically significant. For meta-regression and assessment of publication bias, Comprehensive Meta-Analysis V.3 (Biostat, Englewood, New Jersey, USA) software was used and all other statistical analyses were conducted using Review Manager V.5.3 (The Nordic Cochrane Centre, Copenhagen, Denmark).
Results
Literature retrieval and study characteristics
A total of 2314 articles were identified by the initial search. After duplicate removal and screening of titles and abstracts, 128 articles were assessed on eligibility by full-text review. Subsequently, 26 studies met the criteria for inclusion in the meta-analysis.7 10–12 22–43 An overview of the study selection and reasons for exclusion are presented in figure 1.
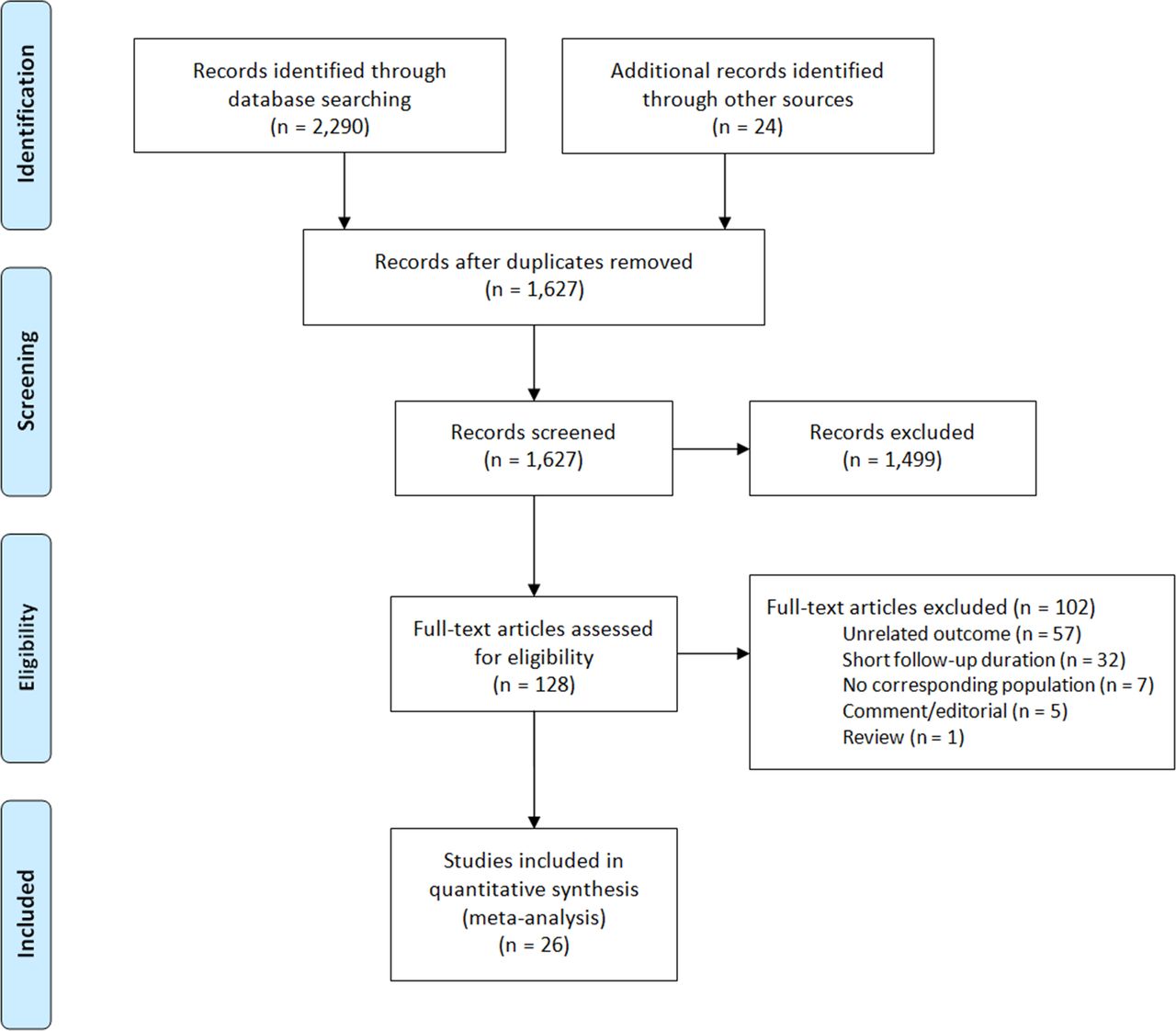
PRISMA flow diagram showing the study selection process.14 PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Table 1 provides the characteristics of the included studies. Age at intervention ranged from 11 to 41 years (median 29 years) and the majority of patients was treated for native CoA as opposed to recurrent CoA (67% vs 33%, respectively). Median length of follow-up was 26 months (range 12–120).
Characteristics of the individual studies assessing BP after CoA stenting
Meta-analysis of studies evaluating systemic BP after CoA stenting
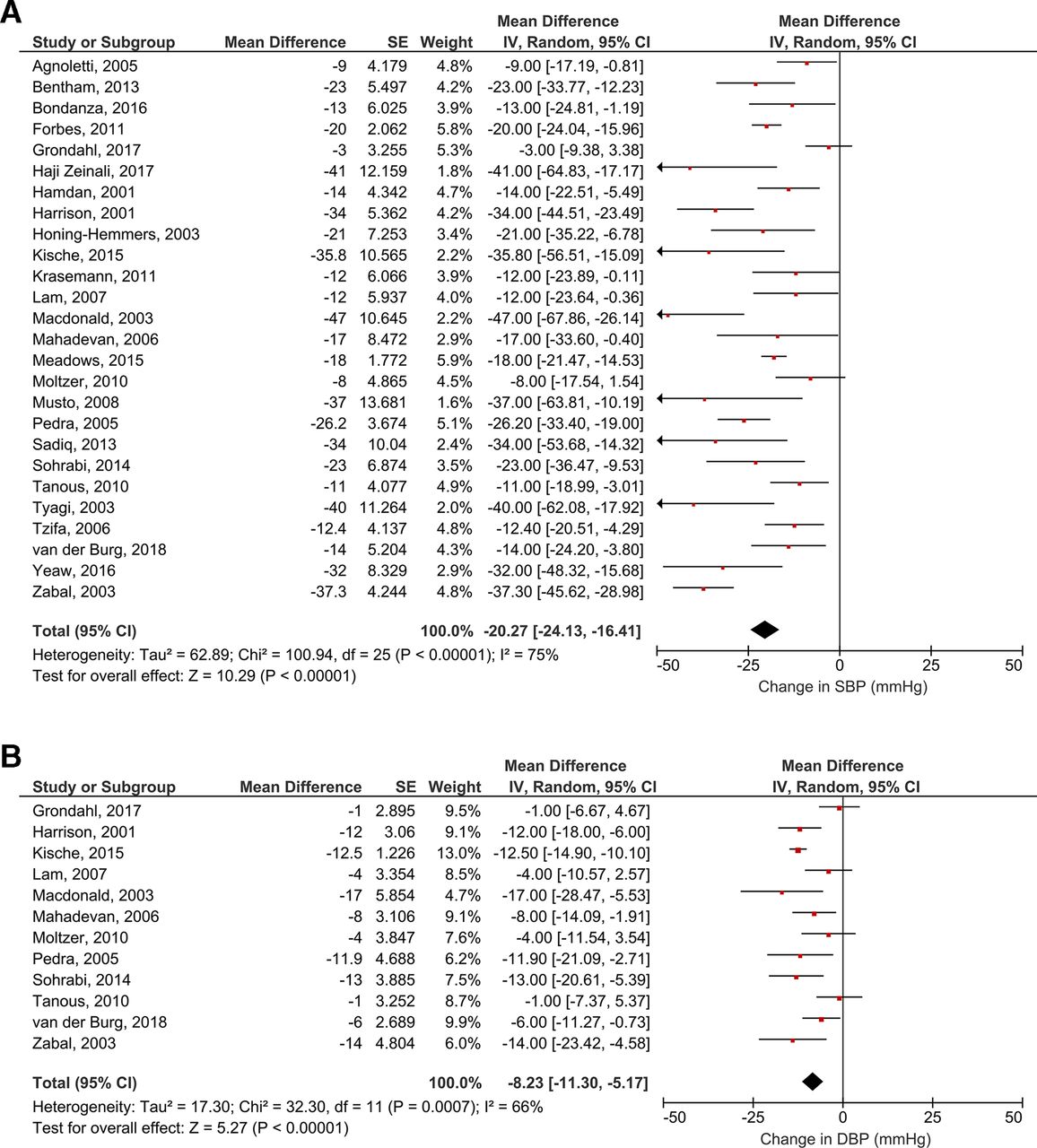
Twenty-six studies enrolling a total of 1157 subjects were used for random-effects meta-analysis on the absolute change in SBP from baseline to last follow-up (figure 2A). In 25 studies only cuff SBP measurements were used and in 1 study a combination of cuff and invasive SBP measurements. Substantial heterogeneity was observed across the included studies (I2=75%). Stent implantation was associated with a pooled reduction in SBP of 20.27 mm Hg (95% CI 16.41 to 24.13 mm Hg; p<0.00001). Additionally, 12 studies including 413 patients evaluated the change in DBP. Meta-analysis showed a significant decrease in DBP after stent implantation (8.23 mm Hg, 95% CI 5.17 to 11.30 mm Hg; p<0.00001; figure 2B). The certainty of evidence for both outcomes was rated as low (online supplementary table S2).

{kind=link}
{kind=link}
Forest plots showing the pooled mean change in SBP (A) and DBP (B) from baseline to last follow-up using a random-effects model. Data are presented as mean difference (mm Hg) and 95% CI. DBP, diastolic blood pressure; IV, inverse variance; SBP, systolic blood pressure; SE, standard error.
Table 2 shows the stratification of studies by various subgroups. The overall decline in SBP was more pronounced in patients aged 18 years and older and patients treated for native compared with recurrent CoA. Furthermore, increased SBP and PSG at baseline and a decrease in AHM use were associated with a greater reduction in SBP at last follow-up. No significant association was found between study design and SBP change.
Mean change in systolic blood pressure (SBP) from baseline to last follow-up among various subgroups
The course of SBP in the included studies is depicted in online supplementary table S3. Median SBP decreased from 152 mm Hg (132–178) at baseline to 128 mm Hg (119–154) at last follow-up. Although various definitions of hypertension were used across studies, the proportion of patients with hypertension decreased from 78% (53%–100%) to 27% (5%–82%) after stenting (online supplementary table S4). This was accompanied by a 40% reduction in patients using any AHM. Of patients remaining on AHM, the dosage was reduced in 70% of cases. The overall number of antihypertensive agents was decreased from 1.6 (0.8–2.3) at baseline to 1.1 (0.7–1.4) after stent implantation.
Meta-regression
Similar to subgroup analyses, the covariates native CoA, SBP at baseline, PSG at baseline and change in AHM use were associated with SBP change in meta-regression (online supplementary table S5). Outcome measurement by 24-hour ambulatory BP monitoring (ABPM) was associated with less SBP reduction compared with office BP measurement. Meta-regression showed no association between age and SBP change.
Sensitivity analyses and publication bias
The significant decrease in SBP after stent implantation observed in the random-effects model persisted in the fixed-effects model (mean difference −18.22, 95% CI −19.90 to −16.53; p<0.00001). Further sensitivity analyses by excluding one study at a time from meta-analysis revealed that no single study significantly changed the pooled effect estimate.
Visual inspection of the created funnel plot showed relative asymmetry, thereby raising concerns of publication bias (online supplementary figure S1). Although quantification of asymmetry by the Egger’s test did not reach statistical significance (p=0.12), we aimed to correct for potential publication bias using the ‘trim and fill’ method (online supplementary figure S2). Application of this method did not change the overall effect.
Discussion
This meta-analysis provides insight into the medium-term BP course of patients who underwent stenting of aortic coarctation. Combining the outcomes of 26 studies with a total of 1157 patients, we show that stent implantation is associated with a significant reduction in SBP and DBP, which is sustained up to 10 years of follow-up. The most pronounced effects were observed in patients aged 18 years and older, patients with high SBP and PSG at baseline, and those treated for native CoA. The decline in SBP was in conjunction with a decrease in the use of AHM.
Short-term outcomes of CoA stenting have been extensively studied and are generally considered satisfying with significant decrease of aortic gradient.9 25 Furthermore, the Congenital Cardiovascular Interventional Study Consortium reported that stenting compares favourably to surgical repair and balloon angioplasty in terms of acute complications.7 Although treatment success is often measured by short-term results, little is known about the medium-term efficacy of stent implantation. Our results suggest a clinically relevant reduction in SBP and DBP during medium-term follow-up, as it has been shown that an SBP reduction of 10 mm Hg and DBP reduction of 5 mm Hg significantly attenuate the risk of major cardiovascular events.17 Importantly, as stated above, this effect could not be attributed to an increased use of AHM poststenting. In contrast, we report a concomitant 40% decline in patients using any AHM, which is likely a consequence of the SBP reduction. However, at late follow-up, over one-third of patients were still in need of AHM for adequate BP control.
Although most patients in the included studies were normotensive at late follow-up, a substantial minority remained hypertensive. The mechanisms responsible for persistent or recurrent hypertension in CoA are poorly understood. Over the last years, there is increasing evidence suggesting that the compliance of the aortic wall plays a role in the origin of persistent hypertension.5 44 Since CoA is considered not merely a discrete lesion but instead part of a generalised vasculopathy, increased resistance of the peripheral vasculature may comprise an additional substrate for hypertension.6 Furthermore, reduced baroreceptor sensitivity and abnormal arch geometry, particularly a hypoplastic or gothic arch, have been linked to the development of hypertension in CoA patients.4 45 A small retrospective study found that stent implantation for aortic arch hypoplasia may significantly attenuate BP, despite potential technical difficulties.46 Inadequate recognition of haemodynamically relevant CoA may provide another explanation for hypertension in this patient cohort. For instance, the influence of anaesthesia during cardiac catheterisation may lead to an underestimation of PSG in an active state. The application of pharmacological agents mimicking physical activity (eg, catecholamines) could be of additional value to determine the true extent of obstruction. Furthermore, more sensitive non-invasive techniques, such as four-dimensional flow MRI and computational flow dynamics, may be useful to distinguish between haemodynamically relevant and non-relevant stenosis.47
In this study, several parameters were found to influence the extent of BP reduction after stenting. Notably, a high baseline PSG was associated with a more pronounced decrease in SBP, while no significant SBP decline was observed with a baseline PSG value <20 mm Hg. These results are in accordance with current guidelines, stating that a PSG >20 mm Hg is suggestive of haemodynamically relevant CoA requiring intervention.8 In contrast, mild residual PSG directly after stent implantation was not associated with persistent hypertension during follow-up. Interestingly, our results indicate that patients treated for recurrent CoA are at greater risk to develop residual hypertension compared with native CoA patients. It is known that prior surgical repair is associated with increased aortic stiffness, which may be partly due to the use of non-compliant prosthetic material and scar tissue.5 44 Discrepancies in baseline BP offer another potential explanation for this difference. Since patients with a previous intervention are closely followed up, reintervention may already be considered in the case of borderline hypertension, whereas native CoA patients generally present with more severe hypertension. It is well known that high baseline BP is predictive of a greater response to antihypertensive treatment, which is consistent with Wilder’s principle.48 This association may have biased our observation that patients<18 years of age, who typically have a lower baseline BP compared with adults, show less decline in SBP after stenting. In fact, stent implantation in children has shown to adequately protect from developing late hypertension, possibly by counteracting the maladaptive vascular changes that are frequently seen in older patients.49 The prognostic implications, rather than the expected absolute BP decline, may guide clinical decision-making in children. Although it is known that late surgical repair is associated with the development of chronic hypertension in CoA, the effect of age at stent implantation is less clear.2 Our results do not show a disadvantage for older patients in terms of BP reduction. However, no definite conclusions can be drawn considering the median follow-up of 26 months, which underlines the importance of studies with longer follow-up after stenting.
Limitations
This meta-analysis has several limitations. First, the included studies were observational, which may have resulted in an underestimation or overestimation of the true effect size. Furthermore, significant heterogeneity was observed across studies, which could not be sufficiently explained by subgroup analyses and meta-regression. This heterogeneity may be partly due to differences in selection criteria between studies, including SBP and PSG at baseline and treatment of native or recurrent CoA. Therefore, one should be cautious to directly extrapolate these findings to individual patients. Another limitation is the dubious reliability of BP assessment, which consisted of regular office measurements in most studies. Previous studies have reported that ABPM is superior to office measurements in the prediction of cardiovascular events and may therefore be a more useful tool in clinical practice.50 Due to the lack of ABPM, patients may have been falsely classified as either normotensive or hypertensive. Studies using ABPM showed less decline of SBP in meta-regression, thereby suggesting that the true effect on SBP may be smaller than the overall observed effect. However, only two studies used ABPM and therefore no definite conclusions can be drawn. We believe it is of major importance to include ABPM in future studies with CoA patients. Moreover, a significant number of studies failed to specify whether the right or left arm was used for BP assessment. Since hypoplasia of the aortic arch is frequently seen in CoA patients, this may have affected BP measurements. Additionally, our results suggested the presence of publication bias. Although adjustment did not significantly alter the pooled outcome, intrinsic limitations when correcting for publication bias have to be taken into account.19 Using GRADE, the certainty of evidence for both outcomes was rated as low, which was due to inconsistency and high risk of bias caused by unreliable BP measurements, failure to control for confounding and incomplete follow-up.
Conclusions
Significant medium-term haemodynamic improvement is observed after stent implantation for CoA, which may effectively reduce the hazard of late cardiovascular complications. Stenting of native CoA and high baseline SBP and PSG were associated with the most pronounced BP reduction after stenting. Controversy exists regarding the underlying mechanisms causing persistent or recurrent hypertension in individual patients. To identify patients at high risk of persistent hypertension, studies focusing on aortic flow dynamics and optimisation of invasive gradient assessment may help in future clinical decision-making in this patient cohort.
Key messages
What is already known on this subject?
It is known that systemic hypertension remains an important source of cardiovascular complications and mortality in patients with coarctation of the aorta (CoA). Treatment of CoA by stent implantation has shown to substantially decrease aortic gradient. However, the effect of stent implantation on medium-term systemic blood pressure is less clear.
What might this study add?
This meta-analysis demonstrates that stenting of CoA is associated with a significant reduction in systolic and diastolic blood pressure during medium-term follow-up. The degree of blood pressure reduction is mainly dependent on baseline systolic blood pressure, baseline peak systolic gradient, and whether stenting is performed for native or recurrent CoA.
How might this impact on clinical practice?
The results of this study provide insight into the medium-term haemodynamic consequences of stent implantation for CoA, which may impact future clinical decision-making in this patient cohort. Prospective studies are needed to identify patients at high risk of persistent hypertension.
Acknowledgments
We would like to thank Paulien H Wiersma for her support with the systematic search and Rob JPM Scholten for his statistical contribution.
References
Footnotes
Contributors Conception and design of the research: TAM and MV. Selection of studies, data extraction and risk of bias assessment: TAM, EW and MV. Analysis and interpretation of the extracted data: TAM, MGS and MV. Drafting of the manuscript and critical appraisal: TAM, EW, MGS, GJK, MMCM, FM, GTS, PD, BJB, RdW, BJMM and MV. Approval of the final version: TAM, EW, MGS, GJK, MCMM, FM, GTS, PD, BJB, RdW, BJMM and MV. Guarantor: TAM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.