Article Text

Abstract
Objective Patients with suspected acute myocardial infarction (AMI) in the setting of left bundle branch block (LBBB) present an important diagnostic and therapeutic challenge to the clinician.
Methods We prospectively evaluated the incidence of AMI and diagnostic performance of specific ECG and high-sensitivity cardiac troponin (hs-cTn) criteria in patients presenting with chest discomfort to 26 emergency departments in three international, prospective, diagnostic studies. The final diagnosis of AMI was centrally adjudicated by two independent cardiologists according to the universal definition of myocardial infarction.
Results Among 8830 patients, LBBB was present in 247 (2.8%). AMI was the final diagnosis in 30% of patients with LBBB, with similar incidence in those with known LBBB versus those with presumably new LBBB (29% vs 35%, p=0.42). ECG criteria had low sensitivity (1%–12%) but high specificity (95%–100%) for AMI. The diagnostic accuracy as quantified by the receiver operating characteristics (ROC) curve of hs-cTnT and hs-cTnI concentrations at presentation (area under the ROC curve (AUC) 0.91, 95% CI 0.85 to 0.96 and AUC 0.89, 95% CI 0.83 to 0.95), as well as that of their 0/1-hour and 0/2-hour changes, was very high. A diagnostic algorithm combining ECG criteria with hs-cTnT/I concentrations and their absolute changes at 1 hour or 2 hours derived in cohort 1 (45 of 45(100%) patients with AMI correctly identified) showed high efficacy and accuracy when externally validated in cohorts 2 and 3 (28 of 29 patients, 97%).
Conclusion Most patients presenting with suspected AMI and LBBB will be found to have diagnoses other than AMI. Combining ECG criteria with hs-cTnT/I testing at 0/1 hour or 0/2 hours allows early and accurate diagnosis of AMI in LBBB.
Trial registration number APACE: NCT00470587; ADAPT: ACTRN12611001069943; TRAPID-AMI: RD001107;Results.
- acute coronary syndromes
- acute myocardial infarction
- ECG/electrocardiogram
Statistics from Altmetric.com
Introduction
Patients with symptoms suggestive of acute myocardial infarction (AMI) account for approximately 10% of all emergency department (ED) consultations. Rapid identification of AMI as a life-threatening disorder is important for the early initiation of highly effective, evidence-based therapy.1–3 Patients presenting with suspected AMI and left bundle branch block (LBBB) to the ED represent a unique diagnostic and therapeutic challenge, as altered ventricular depolarisation masks changes in ventricular repolarisation associated with myocardial ischaemia.2
In patients presenting with ST-segment elevation myocardial infarction (STEMI), who usually can be rapidly identified with the 12-lead ECG, enormous improvements in outcomes have been achieved.1 2 These patients derive major benefit from immediate coronary reperfusion.1 2 It is currently unknown how AMI can best be diagnosed early in patients presenting with suspected AMI and LBBB.1 2 This major uncertainty is highlighted by divergent recommendations given by the respective clinical practice guidelines in the USA and Europe.1 2 Current European Society of Cardiology (ESC) guidelines state that patients with LBBB should be managed in a way similar to patients with STEMI.2 In contrast, current American Heart Association and American College of Cardiology guidelines interpret LBBB not to be diagnostic for AMI.1 Too liberal interpretation of LBBB could lead to thousands of unnecessary cardiac catheterisation laboratory activations and thousands of patients inappropriately given thrombolytic therapy each year, increased risk of complications related to inappropriate invasive procedures, prolonged hospitalisation, higher treatment costs and decreased quality of life for patients.4–6 In contrast, too restrictive interpretation of LBBB could withhold life-saving immediate reperfusion therapy from patients with large AMIs and could ultimately increase mortality.4 7
In order to address this important gap in knowledge, we aimed to first evaluate the incidence of AMI among patients with suspected AMI and LBBB recorded at ED presentation, and second to develop a comprehensive strategy for the early diagnosis of AMI in patients with LBBB.4 8 9
Methods
Study design and oversight
We enrolled adult patients presenting with suspected AMI to the ED in three large, prospective, multicentre diagnostic studies. These are the Advantageous Predictors of Acute Coronary Syndrome Evaluation (APACE),10–13 Accelerated Diagnostic Protocol to Assess patients with chest Pain symptoms using contemporary Troponins as the only biomarker (ADAPT),14 and High-sensitivity cardiac Troponin T assay for RAPID rule-out of AMI (TRAPID-AMI).15 Written informed consent was obtained from all patients (see online supplementary table 1).
Supplemental material
The authors designed the study, gathered, analysed and reported the data according to the Standards for Reporting of Diagnostic Accuracy Studies (STARD) guidelines for studies of diagnostic accuracy16 (see online supplementary table 2), vouch for the data and analysis, wrote the paper, and made the decision to submit it for publication.
Methodology of all three cohorts
In all three cohorts, we included unselected patients presenting to the ED with acute chest discomfort. All patients underwent a clinical assessment that included standardised and detailed medical history, including assessment of chest pain characteristics, vital signs, physical examination, 12-lead ECG, continuous ECG rhythm monitoring, pulse oximetry, standard blood test, and chest radiography and echocardiography if indicated. Treatment of patients was left to the discretion of the attending physician.
Detailed methodical descriptions of all three cohorts, including study design, dates and centres, eligibility criteria and study population, routine clinical assessment, adjudication of final diagnoses, follow-up, and clinical endpoints, are shown in the online supplementary appendix. An overview of study-specific characteristics, including investigational high-sensitivity cardiac troponin (hs-cTn) measurements, adjudication of final diagnoses and specific ECG criteria for all three cohorts, is shown in online supplementary table 1 and described in detail within the online supplementary appendix.
Adjudication of specific ECG criteria
ECG adjudication was performed centrally for all three cohorts by at least two independent cardiologists blinded to all clinical information and using predefined criteria.17 18 LBBB criteria were a QRS duration of more than 120 ms, dominant S wave in V1, broad monophasic R wave in lateral leads (I, aVL, V5–V6), an absence of Q waves in lateral leads (I, V5–V6; small Q waves were still allowed in aVL) and prolonged R wave peak time >60 ms in left precordial leads (V5–V6).
ECG criteria 1–317 included ST-segment elevation of 0.1 mV or more concordant with the QRS complex in any lead (ECG criteria 1, 5 points), concordant ST-segment depression of 0.1 mV or more in lead V1, V2 or V3 (ECG criteria 2, 3 points), and ST-segment elevation of 0.5 mV or more discordant with the QRS complex in any lead (ECG criteria 3, 2 points; see online supplementary figure 1A). A score of ≥3 was suggested for the diagnosis of acute coronary occlusion within the original publication (ECG score ≥3).17 The alternative ECG criteria 318 was proposed to be superior to the original ECG criteria 3 and is defined as a negative ST:S ratio <−0.25 and at least 0.1 mV of ST-segment elevation in any lead (alternative ECG criteria 3, 2 points; see online supplementary figure 1B).19 Again, a score of ≥3 was suggested for the diagnosis of acute coronary occlusion (alternative ECG score ≥3). In case of the presence of LBBB on a previous ECG, LBBB was classified as known. Otherwise it was classified as presumably new. A differentiation between new and new presumably LBBB was not possible, because the exact onset of LBBB could not be determined in most patients. Differentiation between known and presumably new LBBB was possible in cohort 1 by retrieving previous ECG recordings from the electronic ECG storage systems of the participating institutions as well as the general practitioner in the vast majority of patients, but not in cohorts 2 and 3.
Case studies for three patients presenting with suspected AMI and LBBB are described in online supplementary figure 2, including their clinical presentation, medical history, ECG at presentation, hs-cTnT concentrations, coronary angiography results, follow-up information and adjudication diagnoses.
Statistical analysis
The data are expressed as median±IQR for continuous variables, and for categorical variables as numbers and percentages. All variables between known LBBB and presumably new LBBB or LBBB with or without AMI were compared by Student’s t-test or Mann-Whitney U test for continuous variables or Pearson χ2 or Fisher’s exact test for categorical variables. Receiver operating characteristic (ROC) curves were constructed to assess the sensitivity and specificity for concentrations of hs-cTnT/I at presentation and their 1-hour or 2-hour absolute changes. A positive predictive value (PPV) of 80% was considered necessary to proceed with early coronary angiography20 for the derivation of cut-off concentrations. In cohort 1 (derivation cohort) we performed a univariate regression analysis using the selection operator least absolute shrinkage and selection operator (LASSO) to find predictors for the model. Variables who entered this model have been previously selected based on their availability in all three cohorts, shown differences within the baseline characteristics tables and based on their clinical importance. Additionally, the numbers of variables were restricted to the number of events (AMI in patients with LBBB). In cohorts 2 and 3 (validation cohorts), we used the same variables as in cohort 1, if they have shown a statistically significant difference. All hypothesis testing was two-tailed, and p values of less than 0.05 were considered to indicate statistical significance. All statistical analyses were performed with the use of IBM SPSS Statistics for Windows V.24.0.
Results
Study population
Overall, 8830 patients were available for analysis (see online supplementary figure 3). LBBB was present in 247 patients (2.8%; . AMI was the final diagnosis in 30% (75 of 247 patients; of patients with LBBB, with similar incidence in those with known LBBB versus those with presumably new LBBB (29% vs 35%, p=0.42). Patients with known LBBB had similar baseline characteristics as those with presumably new LBBB (see online supplementary table 3). Patients with LBBB were older, had more cardiovascular risk factors and more often pre-existing cardiac disease, including coronary artery disease (CAD) in 54%, as compared with 33% in the overall population (table 1; see online supplementary tables 4–8).

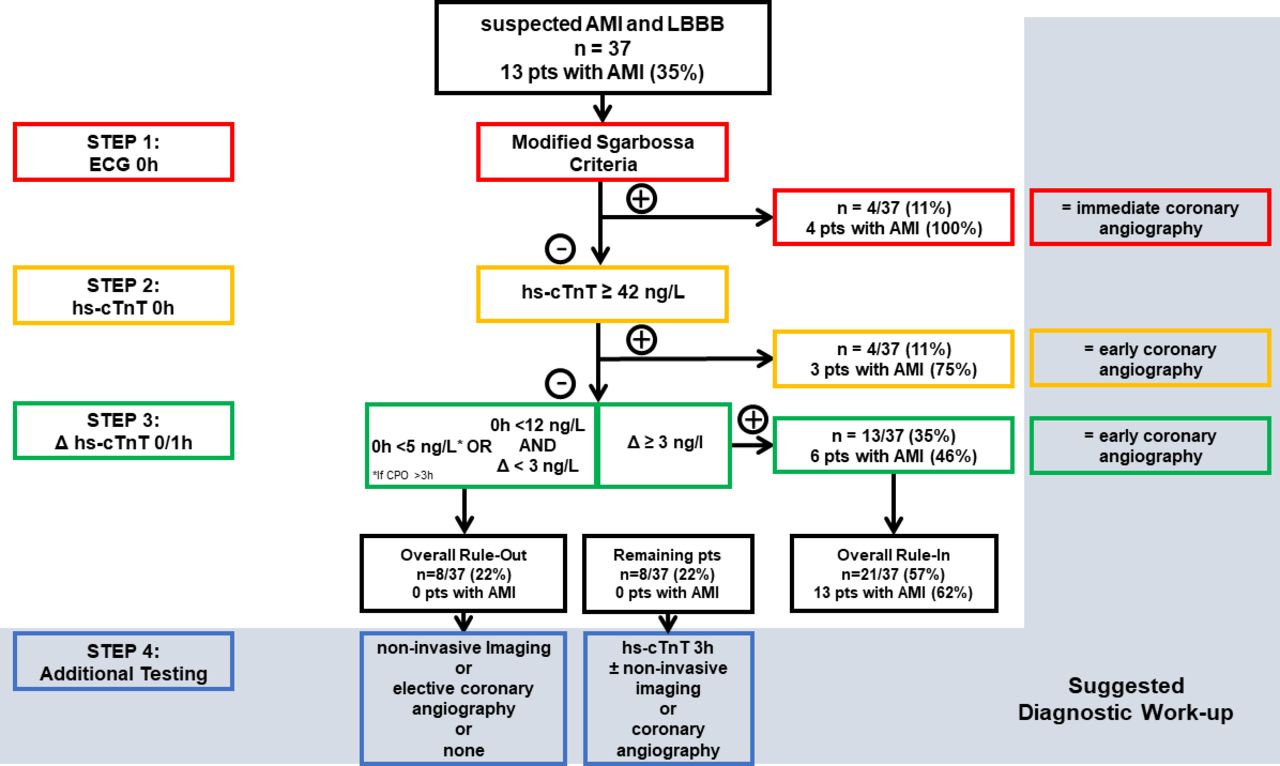
Integrated diagnostic work-up in cohort 1. Flow chart representing the integrated diagnostic work-up for patients presenting with left bundle branch block and suspected AMI in cohort 1 using hs-cTnT. AMI, acute myocardial infarction; hs-cTn, high-sensitivity cardiac troponin; CPO, chest pain onset; LBBB, left bundle branch block; pts, patients.
Baseline characteristics of cohort 1
Echocardiography
Echocardiographic findings were similar in LBBB patients with AMI as compared with LBBB patients without AMI (see online supplementary table 9). Most patients with LBBB had moderately reduced left ventricular ejection fraction (median 40%), a dilated left atrium (70%), left ventricular hypertrophy (56%) and wall motion abnormalities (79%).
Coronary intervention
In patients with AMI and LBBB, coronary intervention was performed in the left anterior descending coronary artery in 16%, in the left circumflex artery in 13%, in a venous bypass graft in 8.9% and in the right coronary artery in 4.4% (table 1).
ECG criteria
Seventeen patients (12%) fulfilled at least one of the specific ECG criteria for AMI detection. Each criteria or their combination in a score had a sensitivity ranging from 1% to 12% and a specificity ranging from 95% to 100% (table 2; see online supplementary figure 4A). We found no differences for specific ECG criteria pertaining to the culprit lesion. Thirteen per cent of patients with specific ECG criteria were found to have the culprit lesion in the left main vessel, ramus interventricularis anterior (RIVA), ramus circumflexus (RCX) or arteria coronaria dextra, respectively.
Diagnostic performance of ECG criteria in all cohorts
High-sensitivity cardiac troponin T/I
Blood concentrations of hs-cTnT and (h)s-cTnI at presentation and their early absolute changes were significantly higher in LBBB patients with AMI as compared with those with other final diagnoses (see online supplementary figure 5). Diagnostic accuracy as quantified by the area under the ROC curve (AUC) was very high (at presentation AUC for hs-cTnT 0.91, 95% CI 0.85 to 0.96; and AUC for hs-cTnI 0.89, 95% CI 0.83 to 0.95; table 3). hs-cTnT levels ≥42 ng/L (hs-cTnI ≥45 ng/L, s-cTnI ≥52 ng/L) provided a PPV of 80% (95% CI 64% to 90%) for AMI, and together with known CAD (OR 4.6, 95% CI 2.0 to 10.4) predicted AMI in multivariate analysis in LBBB patients (OR 31.4, 95% CI 10 to 98.7; table 3; see online supplementary table 10 and figure 4B).
Diagnostic performance of hs-cTn (T and I) and s-cTnI in LBBB patients in all three cohorts
Suggested diagnostic work-up
In cohort 1 at least one specific ECG criteria were positive in 17 of 140 (12%) patients with LBBB and suspected AMI, of whom 8 (47%) patients had an AMI. Of 140 patients, 38 had hs-cTnT concentration at presentation ≥42 ng/L, of whom 29 (76%) had an AMI. Of 140, 11 (8%) had an hs-cTnT 0/1-hour absolute change concentration ≥3 ng/L, of whom 8 (73%) had an AMI (figure 1). In both validation cohorts, using this step-by-step approach resulted in similar findings and high accuracy to identify patients for the suggested work-up (figures 2 and 3).

Integrated diagnostic work-up in cohort 2. Flow chart representing the integrated diagnostic work-up for patients presenting with LBBB and suspected AMI in cohort 2 using hs-cTnI. One patient with LBBB and AMI had not all hs-cTnI measurements at presentation and after 2 hours available. AMI, acute myocardial infraction; CPO, chest pain onset;hs-cTn, high-sensitivity cardiac troponin; LBBB, left bundle branch block; pts, patients.
{kind=link}
{kind=link}
{kind=link}
Integrated diagnostic work-up in cohort 3. Flow chart representing the integrated diagnostic work-up for patients presenting with LBBB and suspected AMI in cohort 3 using hs-cTnT. AMI, acute myocardial infarction; hs-cTn, high-sensitivity cardiac troponin; LBBB, left bundle branch block; pts: patients.
The performance of the individual ECG criteria, of hs-cTnT and hs-cTnI in general, and their respective cut-off concentrations optimised for use in patients with LBBB in particular, was similar among the three cohorts.
Discussion
This analysis is based on three large, prospective, multicentre diagnostic studies with central adjudication of AMI by independent cardiologists applying the universal definition of AMI.3 It was performed to contribute to advancing the clinical care of patients presenting with symptoms suggestive of AMI and LBBB to the ED. We report five major findings.
First, 2.8% of patients presenting with suspected AMI to the ED had LBBB. These patients were older and more often had pre-existing cardiovascular disorders including CAD. Second, the majority of patients presenting with suspected AMI and LBBB were finally found to have non-cardiac disorders and cardiac disorders other than AMI. The incidence of AMI was 30% in LBBB patients and similar in patients with known LBBB versus new/presumably new LBBB. Third, specific ECG criteria had low sensitivity, but high specificity for AMI. Integrating the alternative ECG criteria 3 to the specific ECG score resulted in a sensitivity of 12% and a specificity of 97%. Fourth, the diagnostic accuracy of hs-cTnT and hs-cTnI concentrations at ED presentation and their early changes within 1 hour or 2 hours was very high, and together with a history of known CAD hs-cTnT/I concentrations at presentation predicted the presence of AMI in multivariate analysis. hs-cTnT concentrations at presentation with a predefined PPV of at least 80% for AMI were 42 ng/L or higher (hs-cTnI ≥45 ng/L, s-cTnI ≥52 ng/L). Interestingly, these (h)s-cTnT/I cut-off levels providing a PPV for AMI of 80% in patients with LBBB were similar to those recommended in the current ESC guidelines for the rule-in of AMI in general.21 Fifth, a novel triage algorithm integrating specific ECG criteria as the first step, hs-cTnT/I at presentation as the second, and the 0/1-hour absolute change in hs-cTnT/I as the third step provided high accuracy and efficacy for the early detection of AMI and thereby for the selection of patients for immediate and early coronary angiography in both the derivation and external validation cohorts.
These findings from 8830 patients presenting with suspected AMI to the ED extend and corroborate previous work on patients with LBBB.17 18 22–27 Results derived from selected patients enrolled in clinical trials of new pharmacological therapies had indicated that patients with likely AMI who have new or presumably new LBBB should undergo rapid reperfusion therapy.2 This strategy has recently been challenged by retrospective single-centre studies from unselected ED cohorts or STEMI networks suggesting that most patients with symptoms suggestive of AMI with new or presumably new LBBB do not have AMI.24 25 28–31 However, these studies had important methodological limitations, including retrospective design, use of administrative coding for AMI, use of cardiac biomarkers with poor sensitivity such as CK-MB or previous-generation cTn, and lack of adherence to the universal definition of AMI.1 2
Our study overcomes these limitations and provides detailed guidance on how currently available diagnostic tools can best be used in patients with LBBB to balance the benefits and risks associated with early coronary angiography.1 2 Only one-third of patients presenting with symptoms suggestive of AMI and LBBB to the ED will be found to have AMI as final diagnosis, irrespective of known or presumably new LBBB. Due to their high specificity, specific ECG criteria should be used to immediately triage patients towards rule-in of AMI and immediate coronary angiography such as in patients with STEMI (around 6%–12% of patients with LBBB). Patients not meeting these ECG criteria do have only a slightly higher overall incidence of AMI as compared with patients without LBBB and should undergo standard testing for hs-cTn.1 2 8 14 15 Already the measurement at presentation provides very high diagnostic accuracy and allows to rapidly rule-in additional patients for early coronary angiography, if hs-cTn blood concentrations are substantially elevated (≈15% of patients with LBBB).8 14 15 21 In all remaining patients, the second hs-cTn blood concentration determined 1–2 hours after presentation will allow identification of additional patients with AMI in case of a relevant absolute change and triage them for early coronary angiography. In patients not meeting any of the three rule-in criteria, the likelihood of having AMI is very low. Still, as with all other early triage algorithms, detailed clinical assessment including chest pain characteristics and possibly additional hs-cTnT/I measurements at 3 hours helps in selecting the most appropriate cardiac imaging modality to follow: echocardiography, non-invasive stress imaging, coronary CT angiography, coronary angiography, or none in patients in whom the diagnostic work-up already has established a definite alternative cause of acute chest discomfort at that time, such as pneumonia or pulmonary embolism (figures 1–3 and online supplementary figure 6A,B).20
Among LBBB patients with AMI, culprit lesions most often were in the RIVA and RCX. This distribution differs from all-comers with AMI.17 18 22–27
Potential limitations of the present study merit consideration. First, while a relevant percentage of patients had LBBB recorded on a previous ECG and were classified as known LBBB, as in all previous studies, the exact onset of LBBB was unknown in many patients and LBBB had to be classified as new or presumably new in APACE. This inherent limitation can only be overcome in patients with implantable devices such as pacemakers and loop recorders. In cohorts 2 and 3, limited data on previous ECGs were available; therefore, differentiation between known LBBB and presumably new LBBB was not possible for all patients. Second, although all three studies tried to be broad in the exact definition of its inclusion criteria in order to reflect the clinical challenge, we wish to acknowledge that it is unclear whether the findings of this study can also be extrapolated to patients with AMI presenting with uncommon symptoms such as exclusively with weakness.32 Third, our findings were derived from patients presenting with symptoms suggestive of AMI to the ED. While our study designs ensure the generalisability to this setting, our findings may not apply to settings with a much lower pretest probability for AMI such as patients presenting to a general practitioner, and settings with a much higher pretest probability such as patients in shock or after cardiac arrest transferred directly to a catheter laboratory. Additional studies are necessary in these settings. Fourth, this study required written informed consent. Accordingly, our findings may not apply to critically ill patients unable to provide informed consent, such as patients after cardiac arrest or patients in cardiogenic shock. These patients were eligible only in cohort 2, where a retrospective consent or a consent given by family members was possible. Unfortunately, this limitation also applies to diagnostic tests in general. Fifth, we cannot comment on LBBB in patients with terminal kidney failure, as these patients were excluded in cohorts 1 and 3.
In conclusion, most patients presenting with symptoms suggestive of AMI and LBBB to the ED will be found to have diagnoses other than AMI and should not be considered an STEMI equivalent. An integrated triage algorithm including specific ECG criteria with high specificity, as well as hs-cTnT/I concentrations at presentation and their 0/1-hour or 0/2-hour changes, provides high diagnostic accuracy and efficacy in helping in the selection of patients for immediate and/or early coronary angiography.
Key messages
What is already known on this subject?
Patients with suspected acute myocardial infarction (AMI) in the setting of left bundle branch block (LBBB) present an important diagnostic and therapeutic challenge to the clinician.
What might this study add?
Specific ECG criteria in LBBB patients, including concordant ST-segment elevation (criteria 1) or depression (criteria 2) or pronounced discordant ST-segment elevation (criteria 3), in specific ECG leads and an alternative ECG criteria, including ST-segment depression or elevation discordant with the QRS complex with a magnitude of at least 25% of the QRS complex (alternative criteria 3), together with suggested high-sensitivity cardiac troponin ((h)s-cTn) thresholds (eg, hs-cTnT ≥42 ng/L at presentation), allow an accurate and immediate triage to coronary angiography in patients with LBBB and symptoms suggestive of AMI.
How might this impact on clinical practice?
An integrated triage algorithm including specific ECG criteria with high specificity, as well as hs-cTnT/I concentrations at presentation and their 0/1-hour or 0/2-hour changes, provides high diagnostic accuracy and efficacy in helping in the selection of patients for immediate and/or early coronary angiography.
Acknowledgments
We thank the patients who participated in the study, the staff of the EDs, the research coordinators and the laboratory technicians (particularly Esther Garrido, Irina Klimmeck, Christine Kruse, Sabrina Laule and Fausta Chiaverio) for their most valuable efforts.
References
Footnotes
TN and LC contributed equally.
Twitter @CRIBasel @Thomas_Nest
Contributors TN, JB, RT (cohorts 1 and 3), JG (cohort 2) and CM had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding Cohort 1 (APACE) was supported by research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the European Union, the Cardiovascular Research Foundation Basel, the University Hospital Basel, Abbott, Beckman Coulter, bioMerieux, BRAHMS, Roche, Nanosphere, Siemens, Singulex and 8sense. Cohort 2 (ADAPT) was supported by Queensland Emergency Medicine Research Foundation, Christchurch Heart Institute, Health Research Council and Heart Foundation of New Zealand, and Christchurch Emergency Care Foundation. Cohort 3 (TRAPID-AMI) was sponsored by Roche. The sponsors had no role in the design of the study, analysis of the data, preparation of the manuscript or the decision to submit the manuscript for publication.
Competing interests CM has received research grants from the Swiss National Science Foundation and the Swiss Heart Foundation, the European Union, the Cardiovascular Research Foundation Basel, 8sense, Abbott, Alere, AstraZeneca, Beckman Coulter, bioMerieux, BRAHMS, Critical Diagnostics, Nanosphere, Roche, Siemens, Singulex and the University Hospital Basel, as well as speaker or consulting honoraria from Abbott, Alere, AstraZeneca, BG Medicine, bioMerieux, BMS, Boehringer Ingelheim, BRAHMS, Cardiorentis, Daiichi Sankyo, Novartis, Roche, Sanofi, Singulex and Siemens. LC reports grants from Roche and from Abbott, during the conduct of the study, grants from Roche, grants and personal fees from Abbott Diagnostics, grants from Siemens, grants from Radiometer, personal fees from AstraZeneca, and grants from Alere, outside the submitted work. BL has served as a consultant for Roche Diagnostics, Beckman Coulter, Siemens Healthcare Diagnostics, Radiometer Medical, bioMérieux Clinical Diagnostics, Philips Healthcare and Fiomi Diagnostics. TR has received research grants from the Swiss National Science Foundation (PASMP3-136995), the Swiss Heart Foundation, the University of Basel, the Professor Max Cloetta Foundation, and the Department of Internal Medicine, University Hospital Basel, as well as speaker’s honoraria from BRAHMS and Roche. EG has received honoraria for lectures from Roche Diagnostics, BRAHMS, Thermo Fisher and Mitsubishi Chemical Europe. MC has received research support and speaking honoraria from Roche, Thermo Fisher and Novartis. RT reports speaker honoraria from BRAHMS and Roche. WP reports grants from Roche and from Abbott, during the conduct of the study, and grants from Roche, grants and personal fees from Abbott Diagnostics, grants from Siemens, grants from Radiometer, personal fees from AstraZeneca, non-financial support from Bayer, personal fees from Hospira and grants from Alere, outside the submitted work. MRG has received speaking honoraria from Abbott and a research grant from the Swiss Heart Foundation. JB has received speaking honoria from Siemens. GB is an employee of Roche Diagnostics. JWP is supported by a Senior Research Fellowship from the Canterbury Medical Research Foundation, Emergency Care Foundation and Canterbury District Health. All other authors declare that they have no conflict of interest with this study.
Ethics approval The studies were carried out according to the principles of the Declaration of Helsinki and approved by the local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available from the corresponding author upon request.
Collaborators Petra Hillinger, MD (Department of Cardiology and Cardiovascular Research Institute Basel (CRIB), University Hospital Basel, Switzerland; GREAT network); Karin Grimm, MD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland; GREAT network); Ursina Honegger, Msc (Department of Cardiology and CRIB, University Hospital Basel, Switzerland); Nicolas Schaerli, MD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland; GREAT network); Nikola Kozhuharov, MD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland; GREAT network); Claudia Stelzig, Msc (Department of Cardiology and CRIB, University Hospital Basel, Switzerland); Michael Freese, SN (Department of Cardiology and CRIB, University Hospital Basel, Switzerland); Zaid Sabti, MD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland; GREAT network); Joan Walter, MD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland; GREAT network); Lorraine Sazgary, MD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland; GREAT network); Caroline Kulangara, PhD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland); Kathrin Meissner, RN (Department of Cardiology and CRIB, University Hospital Basel, Switzerland); Deborah Mueller, MD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland; GREAT network); Beatriz Lopez, MD (GREAT network; Emergency Department, Hospital Clinic, Barcelona, Catalonia, Spain); Emilio Salgado, MD (GREAT network; Emergency Department, Hospital Clinic, Barcelona, Catalonia, Spain); Esther Rodríguez Adrada, MD (Emergency Department, Hospital Clinico San Carlos, Madrid, Spain); Damian Kawecki MD (2nd Cardiology Department, Zabrze, University of Silesia, Katowice, Poland); Jiri Parenica, MD (University Hospital Brno, Czech Republic); Eva Ganovska, MD (University Hospital Brno, Czech Republic); Katharina Rentsch, PhD (Laboratory Medicine, University Hospital Basel, Switzerland); Andreas Buser, MD (Blood Bank and Department of Hematology, University Hospital Basel, Switzerland); Jens Lohrmann, MD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland); Roland Bingisser, MD (Emergency Department, University Hospital Basel, Switzerland); Samyut Shrestha, MD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland); Fabio Stallone, MD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland); Roger Abaecherli, PhD (Department of Cardiology and CRIB, University Hospital Basel, Switzerland; GREAT network); James McCord, MD (Henry Ford Heart & Vascular Institute, Henry Ford Health System, Detroit, Michigan, USA); Richard Nowak, MD (Emergency Department, Central Manchester University Hospitals NHS Foundation Trust, Manchester Academic Health Sciences Centre, Manchester, UK); Richard Body, PhD (Emergency Department, Central Manchester University Hospitals NHS Foundation Trust, Manchester Academic Health Sciences Centre, Manchester, UK; Cardiovascular Sciences Research Group, University of Manchester, Oxford Road, Manchester, UK); Christopher R deFilippi, MD (Department of Medicine, University of Maryland School of Medicine, Baltimore, Maryland, USA); Robert H Christenson, PhD (Department of Pathology, University of Maryland School of Medicine, Baltimore, Maryland, USA); Mauro Panteghini, MD (Department of Biomedical and Clinical Sciences ’Luigi Sacco', University of Milan Medical School, Milan, Italy); Mario Plebani, MD (Department of Laboratory Medicine, University Hospital Padova, Italy); Franck Verschuren, MD (Cliniques Universitaires St-Luc and Universite Catholique de Louvain, Brussels, Belgium); John French, PhD (Liverpool Hospital and University of New South Wales, Sydney, Australia); Silvia Weiser, PhD (Roche Diagnostics Germany, Penzberg, Germany); Carina Dinkel, PhD (Roche Diagnostics Germany, Penzberg, Germany); Dagmar I Keller, MD (Emergency Department, University Hospital Zürich, Switzerland); Nicolas Geigy, MD (Emergency Department, Kantonsspital Liestal, Switzerland).
Correction notice Since this article was published online, changes have been made to figures 1-3 and the supplementary files.
Patient consent for publication Obtained.