Article Text

Abstract
Objectives A substantial number of patients with severe tricuspid regurgitation (TR) and congestive heart failure (CHF) are medically managed without undergoing corrective surgery. We sought to assess the characteristics and outcomes of CHF patients who underwent tricuspid valve surgery (TVS), compared with those who did not.
Methods Retrospective observational study involving 2556 consecutive patients with severe TR from the Cleveland Clinic Echocardiographic Database. Cardiac transplant patients or those without CHF were excluded. Survival difference between patients who were medically managed versus those who underwent TVS was compared using Kaplan-Meier survival curves. Multivariate analysis was performed to identify variables associated with poor outcomes.
Results Among a total of 534 patients with severe TR and CHF, only 55 (10.3%) patients underwent TVS. Among the non-surgical patients (n=479), 30% (n=143) had an identifiable indication for TVS. At 38 months, patients who underwent TVS had better survival than those who were medically managed (62% vs 35%; p<0.001). On multivariate analysis, advancing age (HR: 1.23; 95% CI 1.12 to 1.35 per 10-year increase in age), moderate (HR: 1.39; 95% CI 1.01 to 1.90) and severe (HR: 2; 95% CI 1.40 to 2.80) right ventricular dysfunction were associated with higher mortality. TVS was associated with lower mortality (HR: 0.44; 95% CI 0.27 to 0.71).
Conclusion Although corrective TVS is associated with better outcomes in patients with severe TR and CHF, a substantial number of them continue to be medically managed. However, since the reasons for patients not being referred to surgery could not be ascertained, further randomised studies are needed to validate our findings before clinicians can consider surgical referral for these patients.
- heart failure
- valvular heart disease
- tricuspid regurgitation
Statistics from Altmetric.com
Introduction
Tricuspid regurgitation (TR) is a very common valvular abnormality1; however, tricuspid valve surgery (TVS) is rarely performed and is felt to be associated with significant morbidity and mortality.2 3
While there is hope that managing left heart disease would lead to a decrease in TR and hence minimise its impact, the clinical relevance of TR in patients with heart failure is being more recognised, and newer guidelines have wider indications for intervention.4–7 Nevertheless, the timing of TVS remains uncertain. Native TR is usually treated in patients undergoing cardiac surgery for other reasons, whether the regurgitation is severe or if it is moderate with evidence of Tricuspid valve (TV) annulus dilation; this represents 87% of cases of TVS.8 However, isolated TVS is relatively rare, especially for those patients who develop severe and symptomatic TR at some point after prior cardiac surgery. Many patients who meet indications for TVS do not undergo it, likely due to advanced age or comorbidities. However, the characteristics and outcomes of these medically managed patients remain ill-defined. We sought to compare the outcomes of patients with severe TR and congestive heart failure (CHF) who were medically managed to those who underwent TVS.
Methods
This was a single-centre, retrospective, observational study and was approved by our Institutional Review Board. The need for informed consent has been waived as there was minimal risk to the privacy of individuals in this retrospective observational study, according to our institutional policy. The Cleveland Clinic Echocardiography Database was queried for all adult (>18 years old) patients with severe (3+ and 4+) TR between 1 January 2011 and 31 December 2012. We excluded patients without concomitant clinical diagnosis of CHF and those who had undergone cardiac transplantation. History of CHF was collected from the Cleveland Clinic billing database based on the International Classification of Diseases, 9th and 10th Revisions, Clinical Modification diagnoses.
All patients had comprehensive echocardiographic imaging using standard views and methods including two-dimensional, pulse-wave, continuous-wave and colour Doppler imaging. Care was taken to avoid foreshortened views. Left ventricular (LV) ejection fraction, end-systolic and end-diastolic volumes were measured using the biplane method of disks.9 Right ventricular (RV) dysfunction is defined based on a comprehensive integrative approach, according to guidelines,9 including both qualitative and quantitative parameters. Predominantly, visual assessment of RV function in multiple acoustic windows, including dedicated RV views, is used in combination with measured parameters, when available, such as diffusion tension imaging-derived tricuspid lateral annular systolic velocity wave (S′) and tricuspid annular plane systolic excursion. RV function is thus determined to be normal or abnormal with three grades of dysfunction: mild, moderate or severe. TR was assessed in a comprehensive approach, according to guidelines,10 and graded as mild, moderate or severe TR. TV annular end-diastolic diameter was measured in the four-chamber view.
The primary endpoint was all-cause mortality. Left heart disease was defined as patients with LV ejection fraction ≤40% and/or significant left valvular heart disease involving the mitral valve and/or aortic valve. Mitral valve disease was considered significant if there was moderate to severe mitral stenosis (mean gradient ≥5 mm Hg) or moderate to severe mitral regurgitation (≥2+). Aortic valve disease was deemed significant when there was severe aortic stenosis (aortic valve area <1 cm2) or moderate to severe aortic regurgitation (≥2+). Evidence of pulmonary hypertension was defined as RV systolic pressure ≥40 mm Hg, while acknowledging that RV systolic pressure is often underestimated by echocardiography (relying on the Bernoulli equation) in the presence of severe TR, and this would systematically apply to all included patients.
Patient characteristics were determined using the electronic medical records. Data collected included: comorbidities (history of atrial fibrillation/flutter, coronary artery disease, peripheral vascular disease, diabetes mellitus, hypertension, chronic lung disease, hyperlipidaemia, infective endocarditis, pulmonary embolism, New York Heart Association functional class, cardiac pacing and prior open heart surgery), dates of CHF-related hospitalisation, echocardiographic variables (RV function, LV ejection fraction, RV systolic pressure, tricuspid annulus dimension, presence and of mitral and/or aortic valve diseases), intervening TVS and survival. In cases where the date of death was not available, we used the patient’s last encounter date, and same was applied for patients who lost to follow-up.
Continuous variables were expressed as mean±SD, Mann-Whitney test was used to compare continuous variables, while χ2 and Fisher exact tests were used to compare categorical variables. We used the Kaplan-Meier method to estimate survival as well as CHF-related hospitalisation in patients with and without TVS over the study period, and differences between patient groups were tested with the log-rank test. Bivariable and multivariable time-dependent covariate in Cox proportional hazard regression models were used to evaluate the association between TVS and other patient characteristics and mortality. Variables with p<0.2 in bivariable analysis were considered eligible to enter the multivariable model. The associations were expressed as HRs and their 95% CIs. A p<0.05 was considered statistically significant. Same analyses were performed after excluding patients who underwent isolated TV replacement as it is associated with worst outcomes. To eliminate potential confounding factors and bias, propensity-score matching was performed to account for significant differences in baseline characteristics including age, infective endocarditis and significant left side valve disease and LVEF ≤40%. A propensity score was generated for each patient in the standard fashion by performing a logistic regression for TVS versus non-TVS patients. Patients were matched 1:3 to the nearest neighbour with a propensity calliper of 0.1. Kaplan–Meier analysis was performed afterwards to estimate survival in patients with and without TVS. Statistical analyses were performed with SPSS V.25.0 and Stata IC Software V.14.2.
Results
We identified 2556 patients with severe TR (3+ or 4+) by echocardiography. We excluded patients without associated history of CHF (n=1971) and patients who underwent cardiac transplantation (n=51). A total of 534 patients were included in the final analysis. The majority of patients had functional TR (98.5%), mean age was 70.8 years, 49% were male patients, 75% were symptomatic (New York Heart Association functional class III–IV), 75% had significant left heart disease, 80% had evidence of pulmonary hypertension, 50% had a cardiac pacing device (pacemaker or defibrillator) and 44% had history of previous cardiac surgery (table 1). Patients with functional TR included those with underlying pulmonary hypertension (80%), significant mitral valve disease (70%) and RV dysfunction (mild 26%, moderate 32% and severe 19%). Only 55 of 534 patients (10.3%) had TVS during the study period: 39 had combined TV repair, 11 had isolated TV repair and 5 had isolated TV replacement. These patients were younger (67 vs 71 years, p=0.015), had higher incidence of infective endocarditis (11% vs 3%, p=0.007), significant left valvular heart disease (62% vs 40%, p=0.002) but lower heart failure with reduced ejection fraction (42% vs 58%, p=0.002) when compared with the patient group who did not have TVS. Patients who underwent TVS had better survival over a median follow-up period of 38 months (IQR 10–74), (62% compared with 35%, p<0.001) (figure 1), while the 30-day mortality after TVS was 5.5% (n=3).

Kaplan-Meier curve for survival according to TVS patient group. TVS, tricuspid valve surgery.
Baseline characteristics
Among the non-surgical patients (n=479), through chart review, we identified 143 (30%) who had an indication for TVS based on the 2014 American College of Cardiology/American Heart Association and 2017 European Society of Cardiology guidelines for valvular heart disease.5 6 These included: (1) severe TR at the time of left heart surgery (n=14); (2) severe primary symptomatic TR (n=5); (3) severe secondary symptomatic TR (n=102); and (4) secondary symptomatic TR with mild to moderate RV dysfunction but without severe LV dysfunction or severe pulmonary hypertension (n=23). In categories 3 and 4, left heart disease (which includes HFrEF (EF <40%) and/or significant left side valve disease) was present in 64% and 57% of patients, respectively.
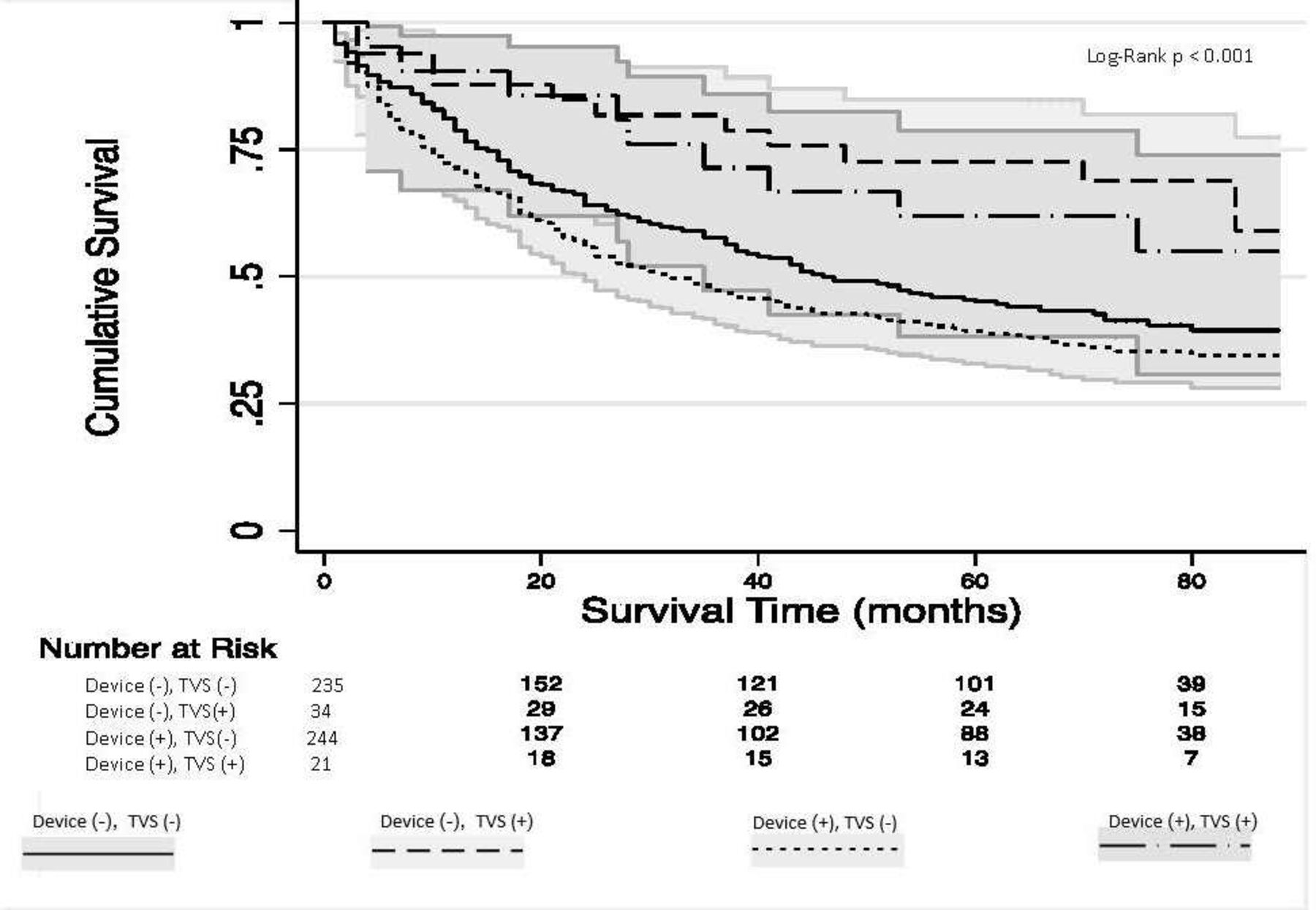
On multivariate analysis, age (HR 1.23; 95% CI 1.12 to 1.35 per 10−year increase in age) and moderate (HR 1.39; 95% CI 1.01 to 1.90) or severe (HR 2; 95% CI 1.40 to 2.80) RV dysfunction were associated with higher mortality, while TVS was associated with improved survival (HR for death 0.44, 95% CI 0.27 to 0.71) (table 2). In patients with implanted cardiac devices (n=265), 21 patients underwent TVS. In these patients, the mortality associated with TVS was similar to that of the general cohort (HR 0.45; 95% CI 0.22 to 0.93). Figure 2 shows the effect of presence of implanted cardiac devices in patients undergoing TVS. The best survival was in patients with no cardiac devices who underwent TVS (n=34) followed by patients with cardiac devices who underwent TVS (n=21), patients with no cardiac device who did not have TVS (n=235) and finally patients who had implanted devices and did not have TVS (n=244).
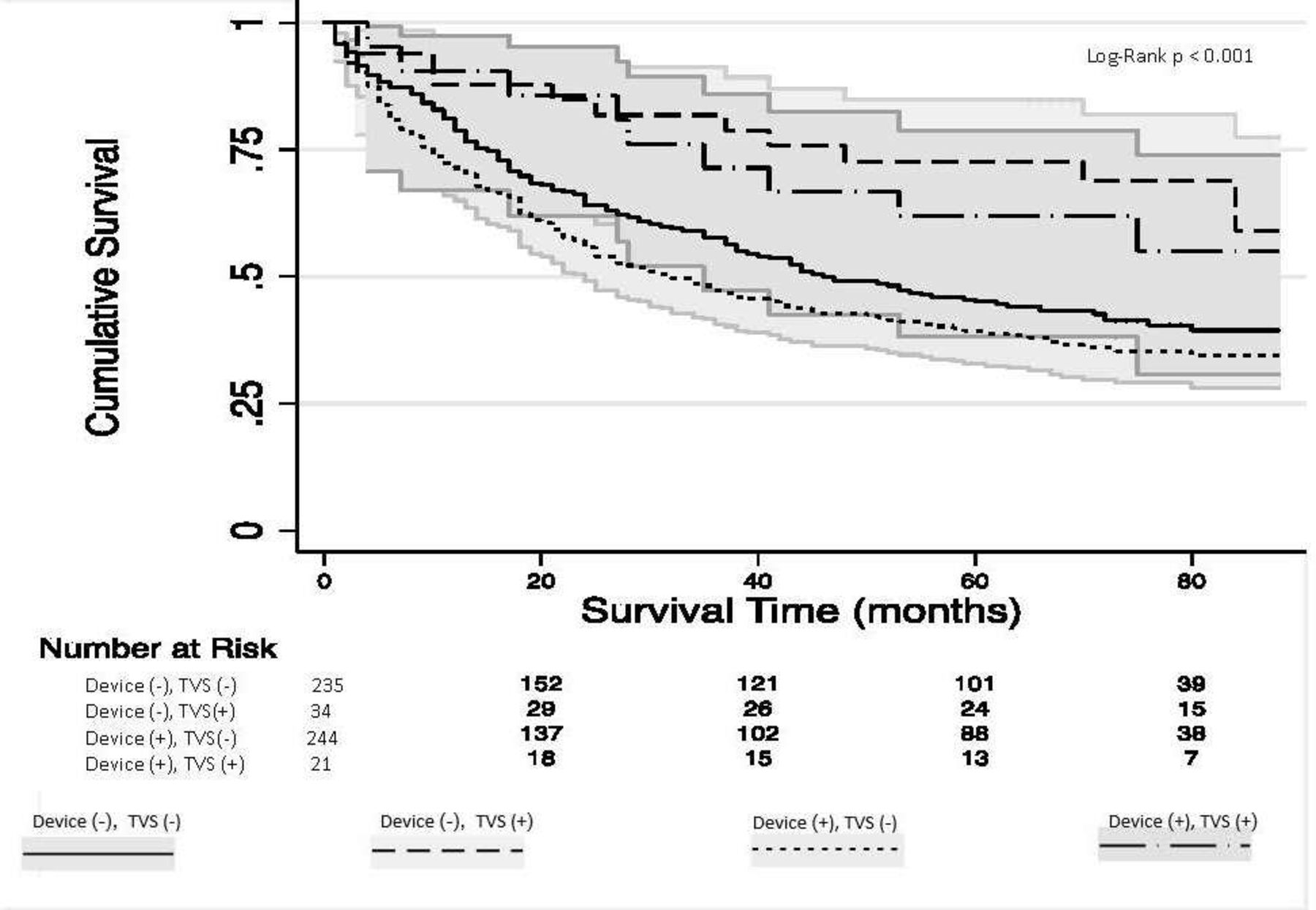
Kaplan-Meier curve for survival according to presence of cardiac device and TVS. TVS, tricuspid valve surgery.
Bivariable and multivariable association between patient characteristics and mortality
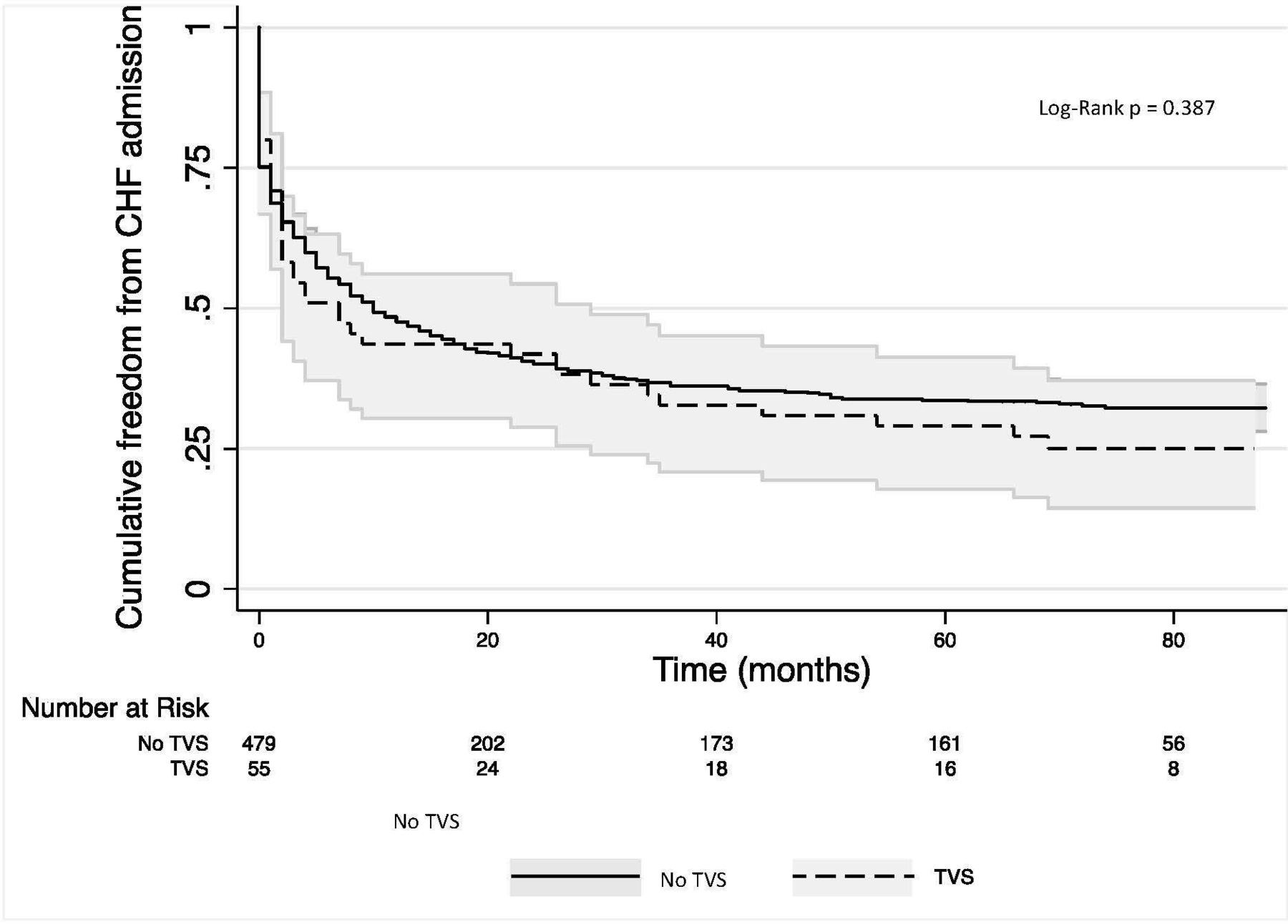
CHF-related hospitalisations rose from 52% in year 1% to 66% by year 5 in the non-TVS group, compared with 56% and 71% in the TVS group. However, the difference over time was not statistically significant (figure 3).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curve for heart failure-related hospitalisation according to TVS patient group. CHF, congestive heart failure; TVS, tricuspid valve surgery.
After excluding patients who underwent isolated TV replacement (n=5), the survival benefit of TVS was sustained: mortality HR 0.44, 95% CI 0.27-.072; p=0.001 (online supplementary table S1, figure S1). Furthermore, after propensity score matching, TVS showed sustained survival advantage when compared with non-TVS group (online supplementary table S2, figure S2).
Supplemental material
Discussion
There are three main findings from this study. First, only a minority (10%) of patients with severe TR and CHF undergo surgery, even though a good proportion of non-surgical patients (~1/3) had an indication for intervention. Second, TVS is associated with improved survival. Third, the rates of readmission are similar over time between TVS and non-TVS patient groups.
TR is a common problem. The prevalence of any TR in patients who underwent echocardiography is reported to be as high as 65%–85%,11 with significant TR (grade >2/4) being present in about 1.2%–10.2% of patients.12 13 Moreover, the occurrence of significant TR is expected to increase as the incidence of LV dysfunction increases.14 This is particularly relevant as increasing TR severity is associated with worse survival. In a study of 5223 veterans in the US Veterans Health Administration system who were followed up for 4 years, the 1-year survival of patients with severe TR was only 64% (compared with 92% with no TR or 90% with mild TR). The poor outcomes were independent of age, biventricular systolic function, RV size and inferior vena cava dilatation.15 In another study of 813 medically managed patients with moderate or severe, isolated TR in South Korea, the 5-year survival was only 74%, independent of patient age.16 TR has also been independently associated with reduced long-term survival in patients with ischaemic or idiopathic LV systolic dysfunction, with or without clinical heart failure.17
In our cohort of patients with severe TR and CHF, only 10% (n=55) underwent TVS. Approximately one-third of the non-surgical patients had an indication for intervention (unmet need). These included patients with severe TR at the time of left heart surgery (n=14), severe symptomatic TR (n=102) and those with symptomatic TR but mild to moderate RV dysfunction, no severe LV dysfunction and no severe pulmonary hypertension (n=23). Over a median follow-up period of 38 months (IQR10-74), patients who underwent TVS had better survival suggesting that a more aggressive approach for patients with significant TR is beneficial. This is especially relevant given that severe TR is associated with worse survival, independent of age or ventricular dysfunction.15 18
In symptomatic patients with severe TR, management is often limited to conservative measures including use of diuretics, which may improve symptoms without survival benefit.17 Many patients who meet an indication for TVS are deemed to be at high risk, due to advanced age and/or comorbidities. However, many patients with mild to moderate TR who undergo isolated left heart surgery may develop severe TR subsequently, and particularly in these patients, reoperative TVS is associated with worse outcomes, especially with worsening RV function.19 20 Interestingly, one-third of patients included in the Trivalve registry developed severe TR after left heart surgery.21
In our study, the rates of readmission were similar over time between patients who were treated medically and the postsurgical group (figure 3). It is also worth mentioning that outcomes of TVS in patients with severe TR and implantable cardiac devices were similar to those in the general cohort. Patients who have a device and undergo TVS still have a better survival than patients who do not have a device and do not undergo TVS. This is an important finding as we have previously demonstrated in our institution that almost one-third of patients with a pacemaker device have 3/4+ TR0.22 While the current study is small, it does suggest that the presence of implantable cardiac devices does not seem to hinder the survival benefit conferred by TVS.
Our study has certain limitations. It was a retrospective analysis from a single-centre using electronic medical records. Given input constraints of electronic medical records, it is challenging to ascertain causes for non-referral without ambiguity. Moreover, half of the patients had previous implantable cardiac devices and were all deemed to have functional TR though this could not be ascertained. Also, it should be noted that RV systolic pressure is usually underestimated in patients with severe TR; accordingly, patients with evidence of pulmonary hypertension would be underrecognised. Furthermore, in patients who underwent TVS in addition to left-sided surgery, the isolated benefits of TVS are difficult to discriminate from those related to the corrective left-sided surgery. Also, many of the available variables were insignificant at the bivariable regression, hence they were not included at the multivariable analysis. This could be related to a relatively small sample size, and the generalisability of our findings to a larger cohort is unknown. Finally, patients who underwent TVS were younger and had better LV and RV systolic functions and hence may have had favourable prognosis even prior to their surgery.
In conclusion, medical management of patients with severe TR and CHF is associated with poor outcomes and high mortality. In these patients, TVS, though rarely performed, appears to be associated with improved survival. However, since the reasons for patients not being referred to surgery could not be ascertained, further randomised studies are needed to validate our findings before clinicians can consider surgical referral for these patients. We acknowledge our findings are hypothesis generating but hope our study can inspire the design and implementation of future trials for validation.
Key messages
What is already known on this subject?
Tricuspid valve surgery (TVS) is underused, likely due to advanced patients’ comorbidities and high surgical risk.
The characteristics and outcomes of these medically managed patients remain ill-defined.
What might this study add?
Nearly one-third of heart failure patients with tricuspid regurgitation (TR) are being medically managed despite having an indication for TVS.
Patients who underwent TVS had lower mortality at 1 and 5 years compared with those who were medically managed (13% vs 29% at 1 year, and 33% vs 61% at 5 years, respectively).
How might this impact on clinical practice?
Further randomised studies are needed before clinicians can consider surgical referral for patients with severe TR and heart failure.
In the meantime, clinicians should consider their options carefully to tailor their treatment for severe TR in patients with heart failure.
References
Footnotes
Contributors AK, VM, YMS, RDG, LN, AH, DM and CM were all involved in the conception, design, analysis and interpretation of the data. AK, RDG, JN, AK, BG, LR, SCH and SK were involved in drafting of the manuscript and revising it critically for important intellectual content. SK made the final approval of the manuscript. All authors are in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of this work will be appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.