Article Text

Abstract
Objectives Atrial secondary mitral regurgitation (ASMR) is a clinically distinct form of Carpentier type I mitral regurgitation (MR), rooted in excessive atrial and mitral annular dilation in the absence of left ventricular dysfunction. Mitral valve annuloplasty (MVA) is expected to provide a more durable solution for ASMR than for ventricular secondary MR (VSMR). Yet data on MR recurrence and outcome after MVA for ASMR are scarce. This study sought to investigate surgical outcomes and repair durability in patients with ASMR, as compared with a contemporary group of patients with VSMR.
Methods Clinical and echocardiographic data from consecutive patients who underwent MVA to treat ASMR or VSMR in an academic centre were retrospectively analysed. Patient characteristics, operative outcomes, time to recurrence of ≥moderate MR and all-cause mortality were compared between patients with ASMR versus VSMR.
Results Of the 216 patients analysed, 97 had ASMR opposed to 119 with VSMR and subvalvular leaflet tethering. Patients with ASMR were typically female (68.0% vs 33.6% in VSMR, p<0.001), with a history of atrial fibrillation (76.3% vs 33.6% in VSMR, p<0.001), paralleling a larger left atrial size (p<0.033). At a median follow-up of 3.3 (IQR 1.0–7.3) years, recurrence of ≥moderate MR was significantly lower in ASMR versus VSMR (7% vs 25% at 2 years, overall log-rank p=0.001), also when accounting for all-cause death as competing risk (subdistribution HR 0.50 in ASMR, 95% CI 0.29 to 0.88, p=0.016). Moreover, ASMR was associated with better overall survival compared with VSMR (adjusted HR 0.43 95% CI 0.22 to 0.82, p=0.011), independent from baseline European System for Cardiac Operative Risk Evaluation II surgical risk score.
Conclusion Prognosis following MVA to treat ASMR is better, compared with VSMR as reflected by lower all-cause mortality and MR recurrence. Early distinction of secondary MR towards underlying ventricular versus atrial disease has important therapeutic implications.
- cardiac surgical procedures
- atrial fibrillation
- mitral valve insufficiency
Data availability statement
Individual deidentified participant data are not available. The study protocol and delineation of study cohorts can be shared on reasonable request.
Statistics from Altmetric.com
Introduction
Functional or secondary mitral regurgitation (MR) in the presence of structurally normal mitral valve leaflets is traditionally attributed to left ventricular (LV) remodelling and dysfunction.1 2 The optimal surgical management of this ‘ventricular secondary mitral regurgitation’ (VSMR) is an unresolved issue, and prognosis remains poor despite its high prevalence.3 4
In contrast, ‘atrial secondary mitral regurgitation’ (ASMR)—rooted in left atrial (LA) remodelling and isolated annular dilation—finds itself at the other end of the secondary MR spectrum.5 6 Little is known about the optimal treatment strategy for this Carpentier type I MR, typically found in longstanding atrial fibrillation (AF)5 and/or heart failure with preserved ejection fraction.7 A therapeutic approach targeting the annulus might lead to better results in this annular disease state, when compared with VSMR with subannular disease. Yet data on outcome and repair durability are scarce. The objectives of this study were to explore outcomes after mitral valve annuloplasty (MVA) for ASMR versus VSMR and to compare rates of MR recurrence between both groups.
Methods
Study population
All consecutive MVA procedures performed between November 2010 and April 2018 were retrospectively screened from the surgical database of an academic centre (Department of Cardiac Surgery, Leuven University Hospitals, Leuven, Belgium). Exclusion criteria were presence of: (1) organic mitral valve disease, (2) active endocarditis, (3) cardiac tumour, (4) hypertrophic cardiomyopathy with systolic anterior leaflet motion of the mitral valve and (5) congenital heart disease (online supplemental figure 1).
Supplemental material
The resulting study population comprised both ASMR and VSMR patients who underwent surgical MVA. ASMR was defined as MR caused by isolated annular dilation5 6 in absence of intrinsic leaflet and LV disease. Annular dilation was defined as a systolic anteroposterior diameter exceeding 35 mm or when the ratio of systolic annular diameter/diastolic anterior leaflet length was >1.3.8 9 Furthermore, in ASMR, LV volume and global/regional systolic function was invariably normal (ie, left ventricular ejection fraction (LVEF) ≥50%).
VSMR was defined according to current guidelines2 10 as secondary MR due to an imbalance between increased tethering forces and decreased closing forces in the context of LV dilatation or dysfunction. Accordingly, inclusion criteria for VSMR were: (1) absence of organic valve disease, (ii) reduced LVEF (<50%) and/or global or regional alterations in LV geometry, thereby hampering coaptation of structurally normal leaflets. Of note, relative annular dilation is often noticeable in VSMR as well, owing to longstanding LA volume overload.
Given its retrospective design, the need for a written informed consent was waived by the local Ethical Committee (S64979). The time of the index procedure marked the time point of entry in the analysis. Clinical data were collected for each participant at time of the index procedure and used to predict the risk of in-hospital mortality after cardiac surgery (European System for Cardiac Operative Risk Evaluation (EuroSCORE) II).
Patient and public involvement
In view of the observational retrospective study design, patients were not involved in the design nor conduct of this study. Nevertheless, all research questions and outcome measures in this study were developed in order to provide better patient care in the future. The overall results will be shared with the public through a dedicated website of our academic centre. Study results will be shared in layman’s language in a study newsletter for a non-specialist audience.
Surgical procedure
The majority of surgical procedures (87.5%, n=186) were performed through midline sternotomy under normothermic cardiopulmonary bypass with intermittent retrograde cold blood cardioplegia. In minimal access surgery, single-shot antegrade, cold crystalloid cardioplegia was used. Patients with an indication for revascularisation underwent coronary artery bypass grafting first. The mitral valve itself was exposed through a vertical transseptal approach along the right border of the foramen ovale, leaving the LA roof untouched or through a left atriotomy anterior to the right superior pulmonary vein and posterior to the interatrial sulcus (along the Waterston’s or Sondergaard’s groove).
In 12.5% (n=27), the mitral valve was repaired by means of a minimally invasive approach through a right lateral minithoracotomy under videoscopic) guidance (Port-Access endovascular cardiopulmonary bypass system, Heartport, Inc, Redwood City, California, USA).
Annuloplasty ring size was determined by reference to direct measurement of the anterior leaflet height using a flexible (Carbomedics ring, Sorin group, Saluggia, Italy), semirigid saddle-shaped (Carpentier-Edwards Physioring, Edwards Lifesciences, Irvine, California, USA or Memo3D ring, Sorin group) or rigid (Edwards Geoform ring, Edwards Lifesciences, n=1) ring design to achieve a leaflet coaptation height of at least 8 mm. Surgical ablation of AF was performed by the modified Coxs-Maze IV procedure (bipolar radiofrequency heat and cryoablation to create transmural lesions), when indicated according to consensus guidelines.
Concomitant tricuspid valve repair was performed by ring (Carpentier-Edwards Physio-ring, Edwards Lifesciences; Carbomedics ring, Sorin group; Contour 3D ring, Medtronic, Minnesota, USA) or suture (De Vega technique) annuloplasty when indicated using the height of the anterior leaflet as a reference.
The restored leaflet coaptation was confirmed at the time of surgery by filling the ventricle with saline through a bulb syringe. Additionally, after weaning from cardiopulmonary bypass, intraoperative transoesophageal echocardiography was used to assess the result of the valve reconstructions.
Image acquisition and storage
Comprehensive two-dimensional echocardiography exams were performed with a commercially available system (GE Healthcare, Chicago, Illinois, USA or Philips Medical Systems, Andover, Massachusetts, USA). Standard two-dimensional and Doppler echocardiographic images were acquired in the left lateral decubitus position using a phased-array transducer in the parasternal and apical views by experienced cardiac sonographers. Four consecutive cardiac cycles were recorded and stored as DICOM files on a secured server. Echocardiographic parameters were measured according to the guidelines of the American Society of Echocardiography and the European Association of Cardiovascular Imaging.11
LV volumes and ejection fraction were calculated by use of Simpson’s biplane method. Left atrial end-systolic volume was measured using the modified Simpson’s rule from the apical four-chamber view. MR severity was graded by integrating multiple parameters per international guideline recommendations.12
Follow-up and clinical outcomes
Clinical endpoints were recurrence of ≥moderate MR and all-cause mortality, both evaluated as a time-dependent variable.
Echocardiographic follow-up was done at the discretion of the treating cardiologists. Heart failure readmissions were defined as unscheduled hospitalisations during which intravenous diuretic agents were administered because of signs and symptoms of congestion. Censoring occurred at time of the last visit in the outpatient cardiology clinic.
Statistical analysis
Continuous variables were expressed as mean±SD if normally distributed or median (IQR) if non-normally distributed. Normality was assessed by the Shapiro-Wilk test. Continuous variables were compared using the independent Student’s t-test or Mann-Whitney U test, according their distribution. Categorical data were expressed as numbers and percentages and compared using the χ2 test (or Fisher’s exact test in case of cell counts were <5).
Event rates were calculated according to the Kaplan-Meier method and compared using the log-rank test. Cox proportional hazard regression analysis was performed to evaluate the association between secondary MR aetiology and outcome events following MVA. Variables with a p value <0.10 in univariate Cox regression analysis were entered into the multivariable linear regression model. Collinearity was always verified. Next, a competing risk Fine and Gray’s analysis with MR recurrence as primary outcome and all-cause death as competing risk was compared with the initial Cox regression model. Outcome analyses were exclusively applied to patients who survived beyond 30 days following surgery.
Statistical significance was always set at a two-tailed probability of p<0.05. Statistical analyses were performed using STATA V.12.1 (StataCorp LLC, College Station, Texas USA). The manuscript was written in accordance with the recommendations given by the Strengthening the Reporting of Observational Studies in Epidemiology initiative.
Results
Between November 2010 and April 2018, 216 MVA procedures were performed at the Leuven University hospitals to treat secondary MR. Of these, 97 patients had evidence of ASMR, with isolated annular dilation being the culprit mechanism responsible for MR.
Baseline characteristics and preoperative echocardiographic data
Baseline patient characteristics are summarised in table 1 and baseline echocardiographic data in table 2. Patients with ASMR were predominantly female (p<0.001) and slightly older (p=0.039), as compared with VSMR. Cardiovascular risk factors were equally distributed, except for a higher prevalence of diabetes and dyslipidaemia in VSMR. The proportion of persistent and permanent AF was higher in ASMR, compared with VSMR (36.1% and 24.7%, respectively, p<0.001). This was reflected by a larger LA size in the former group (p=0.033, table 2). MR severity at baseline was comparable between groups, though the leading mechanism responsible for leaflet malcoaptation differed by definition. LV remodelling and/or dysfunction was present in VSMR with substantial subannular leaflet tethering (p<0.05 for all tethering parameters compared with ASMR, table 2). In addition, LA and annular dilation was often found in VSMR as a consequence of long-standing volume overload. This contrasted with ASMR, in which excessive annular dilation exhausted annular leaflet reserve (annular diameter >35 mm or ratio annular area/anterior mitral leaflet length >1.3) in absence of subannular tethering (table 2).
Baseline demographics
Echocardiographic parameters
Surgical data and postoperative course
Surgical data are summarised in table 3. Approximately one in two patients with ASMR received concomitant tricuspid valve repair (p<0.001, compared with VSMR), reflecting more severe TR at baseline in this group (p=0.004). Concomitant Cox-Maze IV and left atrial appendage closure was performed more often in ASMR (p<0.001 for both), paralleling the higher prevalence of AF in this group (p<0.001). MR was trace or mild (at the most) in all patients immediately postrepair.
Surgical data and postoperative course
One patient with ASMR died in the acute postoperative period, while six (5.0%) deaths occurred after repair of VSMR (p=0.098).
Recurrence of ≥moderate MR
Overall median follow-up was 3.3 (IQR 1.8–5.3) years and comparable between ASMR and VSMR (p=0.689). Table 4 lists the event rates for both groups during follow-up, which were consistently worse in VSMR (p<0.05 for all). MR recurrence was 25% within 2 years following VSMR repair, opposed to 7% in ASMR.
Event rates after mitral valve annuloplasty in ASMR and VSMR
The rate of recurrent ≥moderate MR was significantly lower in ASMR (log-rank p=0.001, figure 1A) corresponding to a HR of 0.39 (95% CI 0.22 to 0.71). Results remained valid even when handling all-cause death as competing risk (Fine & Gray’s analysis, subdistribution HR 0.50, 95% CI 0.29 to 0.88, p=0.016).

Outcomes after surgical annuloplasty for VSMR versys ASMR. Panel A: Kaplan-Meier estimate showing significantly less MR recurrence after annuloplasty to treat ASMR. Panel B: Kaplan-Meier curve showing significantly higher all-cause mortality in VSMR. ASMR was independently linked to improved survival following MVA (adjusted HR 0.43, 95% CI 0.22 to 0.82, p=0.011). ASMR, atrial secondary mitral regurgitation; MR, mitral regurgitation; MVA, mitral valve annuloplasty; VSMR, ventricular secondary mitral regurgitation.
All-cause mortality
All-cause mortality was significantly higher in VSMR (log-rank, p=0.002) (figure 1B). In Cox proportional hazard analysis, ASMR was associated with better overall survival (adjusted HR 0.43 95% CI 0.22 to 0.82, p=0.011), independent from age, hypertension and baseline EuroSCORE II risk score (table 5). Long-term postoperative moderate or worse TR was linked to poor prognosis, although the overall rates were comparable between VSMR and ASMR. Moreover, ASMR remained independently linked to superior survival following MVA, even in spite the degree of postoperative TR.
Predictors for all-cause mortality after mitral valve annuloplasty
Discussion
This study investigated clinical and echocardiographic outcome of MVA in atrial versus ventricular MR. The key finding of this study is that MVA results in more durable MR reduction and better outcome when excessive isolated annular dilation is the predominant mechanism responsible for leaflet malcoaptation (figure 2). An early distinction of MR towards underlying ‘ventricular’ (VSMR) versus ‘atrial’ disease (ASMR) could therefore have important therapeutic implications.

Mitral valve annuloplasty to treat VSMR versus ASMR schematic illustration showing persistent subannular leaflet tethering after annuloplasty to treat VSMR, opposed to improved leaflet coaptation in ASMR. ASMR, atrial secondary mitral regurgitation; LV, left ventricular; MR, mitral regurgitation; MVA, mitral valve annuloplasty; VSMR, ventricular secondary mitral regurgitation.
VSMR—defined as secondary MR in current guidelines—results from an imbalance between increased tethering forces (due to global/focal LV dilation and outward papillary muscle displacement/dysfunction) and decreased closing forces (reduced LV contractility or dyssynchrony) in the presence of a structurally normal valve. Eventually, annular dilation owing to long-standing LA volume overload may aggravate MR, although the latter is not the main driver for regurgitation in this pathophysiology.4 In other words, increased annular dimensions may contribute to the imbalance, though concomitant subvalvular tethering typically sets the stage for leaflet malcoaptation in VSMR.
Surgical interventions targeting at the mitral valve have yielded disappointing results in VSMR. Originally, restrictive MVA had been favoured in this setting based on good short-term and midterm data from observational studies demonstrating significant reverse LV remodelling13 and improvements in LV systolic function.14 However, persisting subannular tethering15 leading to high MR recurrence rates (up to 33% and 59% within 116 and 217 years, respectively, following MVA) and potential mitral stenosis,18 19 together with the lack of survival benefit,20–22 have led to a shift towards a less common use of MVA to treat VSMR.
On the other end of the secondary MR spectrum, regurgitation caused by excessive LA and mitral annular dilation is increasingly recognised as a clinically distinct aetiology, named ASMR in which LV size and function are inherently normal. Both long-standing AF6 23 24 and/or chronic LA pressure overload in the setting of heart failure with preserved ejection fraction7 give rise to excessive LA stretch, followed by annular dilatation and ASMR. In our study, AF was found in over 76% of patients with ASMR preoperatively. Recently, insufficient compensatory leaflet growth (ie, failure to match annular dilation resulting in annular leaflet mismatch) has been considered equally important in the pathophysiology of ASMR.25 26
The newly published 2020 American College of Cardiology/American Heart Association guidelines1 do acknowledge this distinct form of Carpentier I MR and highlight the paucity on data regarding mitral valve repair in this context. Few studies addressed the question whether an approach targeting the annulus only is beneficial in this setting. Vohra et al 27 have reported persistent MR reduction after annuloplasty±surgical ablation in 20 cases of Carpentier type I secondary MR. However, preoperative LVEF was depressed in 35% of cases which conflicted their data.28 Kihara et al 24 and Takahasi et al 29 have noted good short-term outcomes after mitral annuloplasty in respectively 12 and 10 cases of ASMR (no MR recurrence and significant improvements in left atrial volume index and New York Heart Association class, respectively). Long-term outcomes were superior after endoscopic mitral valve repair for ASMR as opposed to standard of care in ASMR in one recent retrospective analysis,30 though both groups were not propensity matched for ASMR severity at baseline.
To the best of our knowledge, no head-to-head comparison has been performed between MVA to treat VSMR and ASMR yet (figures 2 and 3). This study, therefore, may add several valuable nuances. Although only hypothesis generating due to the retrospective study design, timely phenotyping of ASMR seems of paramount importance. Annuloplasty may in fact change disease course in ASMR opposed to VSMR in which until now no survival benefit has been shown following surgical annuloplasty. ASMR patients are known to have a different risk profile as compared with VSMR (with LV disease, heart failure with reduced ejection fraction and more extensive risk factors). This is reflected by a lower EuroSCORE II, and, hence also in the observed difference in perioperative and postoperative mortality. Indeed, all-cause mortality was significantly higher in VSMR, even after adjusting for obvious differences in EuroSCORE II.
{kind=link}
{kind=link}
{kind=link}
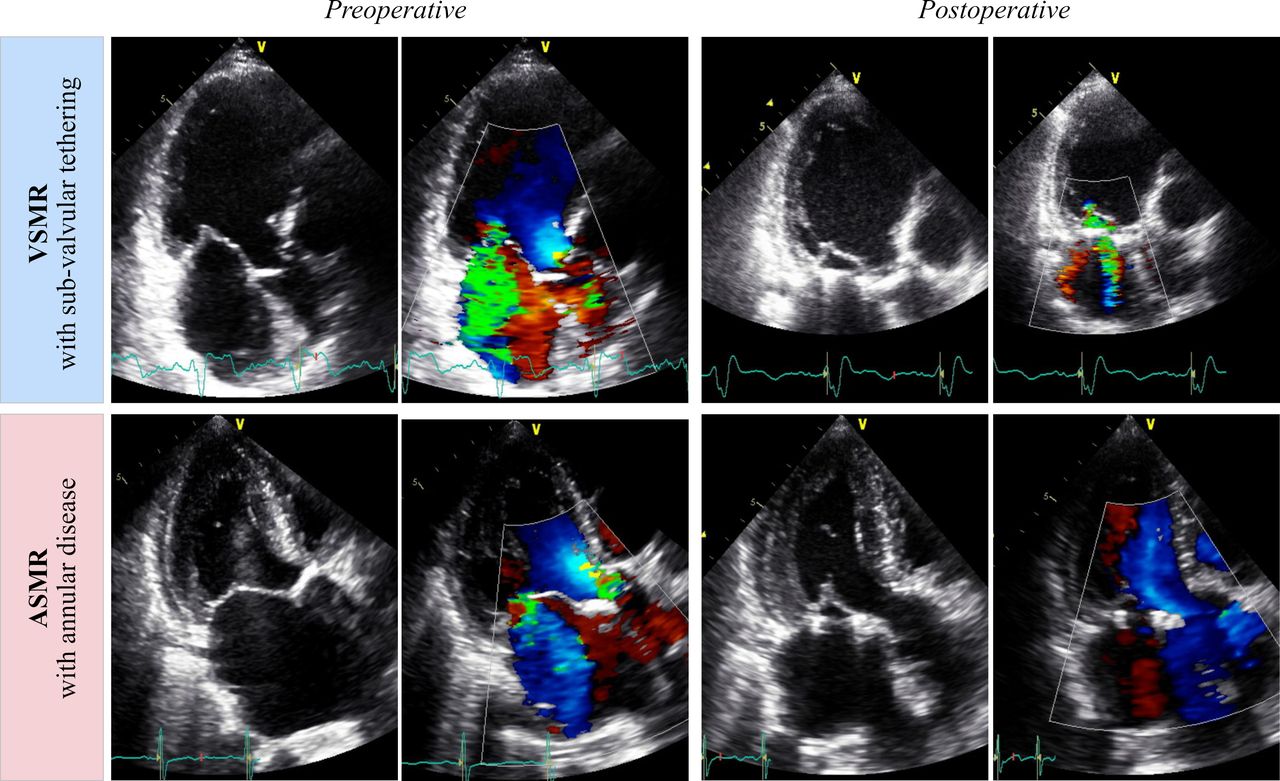
Preoperative and postoperative echocardiographic appearance of ASMR versus VSMR substantial subvalvular leaflet tethering is found in VSMR, which persists even after surgical restrictive annuloplasty. Annular disease is targeted after surgical annuloplasty in ASMR with beneficial effect on MR severity. ASMR, atrial secondary mitral regurgitation; MR, mitral regurgitation; MVA, mitral valve annuloplasty; VSMR, ventricular secondary mitral regurgitation.
Second, from a pathophysiological point of view, the likelihood of MR recurrence after MVA seems lower, considering disease progress is halted by MVA in ASMR, whereas in VSMR, subannular tethering continues. As such, MVA may serve as a bail-out therapy when rhythm-control strategies and optimal medical therapy fail to reverse severe ASMR. In the present era, in which the prevalence of AF and/or heart failure with preserved ejection fraction is growing to epidemic proportions, further research is warranted to improve our therapeutic efficiency in this patient population. Furthermore, additional prospective study comparing a surgical cohort of ASMR with ASMR without mitral valve surgery is needed to explore whether surgical mitral valve repair does alter prognosis in this disease state.
Study limitations
This is a retrospective single-centre observational study. Patients with LV dysfunction had a higher operative risk at baseline, which translates to worse overall prognosis in survival analyses. Nevertheless, ASMR remained independently associated with improved survival in this study. These findings further stress the need for a separate definition of these two patient groups that currently are both contained within the term ‘secondary’ MR. Future trials might unravel the enigma if worse outcome is attributable to more advanced disease at baseline, higher rates of MR recurrence or both. Finally, due to the retrospective study design long-term data on blood pressure management, LV compliance and HFpEF phenotyping were lacking.
Conclusion
Atrial secondary MR is a distinct of form of Carpentier I MR at the other end of the secondary MR spectrum. Prognosis after MVA to treat ASMR opposed to VSMR is better, as reflected by lower all-cause mortality and MR recurrence independent from baseline differences. Early distinction of secondary MR towards underlying ventricular versus atrial disease is important for therapeutic considerations.
Key messages
What is already known on this subject?
Atrial secondary mitral regurgitation (ASMR) is a relatively new entity, rooted in excessive left atrial and annular dilation. Currently, ASMR is under-recognised as a separate entity in daily clinical practice, as ASMR and ventricular secondary mitral regurgitation (VSMR) are both classified under the umbrella term ‘secondary MR’. The newly published 2020 American College of Cardiology/American Heart Association guidelines do acknowledge this distinct form of Carpentier I mitral regurgitation (MR) and highlight the paucity on data regarding mitral valve repair in this context.
What might this study add?
Surgical mitral valve annuloplasty to treat VSMR has been matter of controversy in the past decade due to the lack of survival benefit and high MR recurrence rates. This retrospective cohort study shows that mitral valve annuloplasty is followed by a more durable MR reduction and better outcomes when excessive isolated annular dilation is the predominant mechanism responsible for leaflet malcoaptation (ie, ASMR), as opposed to VSMR with subvalvular leaflet tethering. Importantly, the superiority of mitral valve annuloplasty in ASMR is observed, even when corrected for differences in baseline EuroSCORE II between both cohorts and when handling all-cause mortality as competing risk.
How might this impact on clinical practice?
Early distinction of secondary MR towards underlying ventricular (VSMR) versus atrial disease (ASMR) is important for therapeutic considerations. Hence, mitral valve annuloplasty provides more durable results and better outcomes when the valvular disease process is situated at annular level as compared with subannular disease in VSMR. Future studies comparing a surgical cohort of ASMR with a propensity-matched ASMR cohort without mitral valve surgery are needed to explore whether surgical mitral valve repair does alter prognosis in this disease state.
Data availability statement
Individual deidentified participant data are not available. The study protocol and delineation of study cohorts can be shared on reasonable request.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
PMV and FR are joint senior authors.
Twitter @S_Deferm, @Ph_Bertrand, @JeroenDauw, @alexvdbruaene, @pietvandervoort, @RegaFilip
Contributors All authors have made substantial contributions to the conception of this work, data analysis and content revision. The manuscript has been finally approved by all authors, who agree to be accountable for all aspects of the current work, in line with current ICMJE recommendations.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.