Article Text

Abstract
Transcatheter aortic valve implantation (TAVI) for isolated aortic regurgitation (AR) comprises <1.0% of all TAVI procedures performed in the USA. In this manuscript, we review the challenges, evidence and future directions of TAVI for isolated AR. There are no randomised clinical trials or mid-term data evaluating TAVI for isolated AR, and no commercially available devices are approved for this indication. Challenges in performing TAVI for isolated AR as opposed to aortic stenosis (AS) include: lack of a calcified anchoring zone for valve deployment, large and dynamic size of the aortic annulus and high stroke volume (during systole) and regurgitant volume (during diastole) across the aortic annulus during each cardiac cycle. Observational studies have shown that outcomes of TAVI for AR are worse than outcomes of TAVI for AS. However, newer generation TAVI devices may perform better than older generation devices in patients with AR. Two emerging valves (the JenaValve and the J-Valve) are designed with mechanisms to anchor in a non-calcified annulus, and these valves have shown promise for AR. Data on these devices are limited, and clinical investigation is ongoing. Randomised clinical trials are needed to establish TAVI as a safe and effective treatment for isolated AR.
- heart valve prosthesis implantation
- transcatheter aortic valve replacement
- aortic valve insufficiency
Statistics from Altmetric.com
Introduction
Transcatheter aortic valve implantation (TAVI) is now performed in over 700 hospitals in the USA as an approved and well-established treatment for aortic stenosis (AS). Between 2018 and 2019, the volume of TAVI procedures in the USA eclipsed the volume of surgical aortic valve replacement procedures.1 However, since the approval of commercial TAVI in late 2011 through 2019, only 1864 of all 276 316 (0.7%) TAVI procedures in the USA were performed for isolated aortic regurgitation (AR).1 In this manuscript, we review the challenges, evidence and future directions of TAVI for isolated AR.
Case example
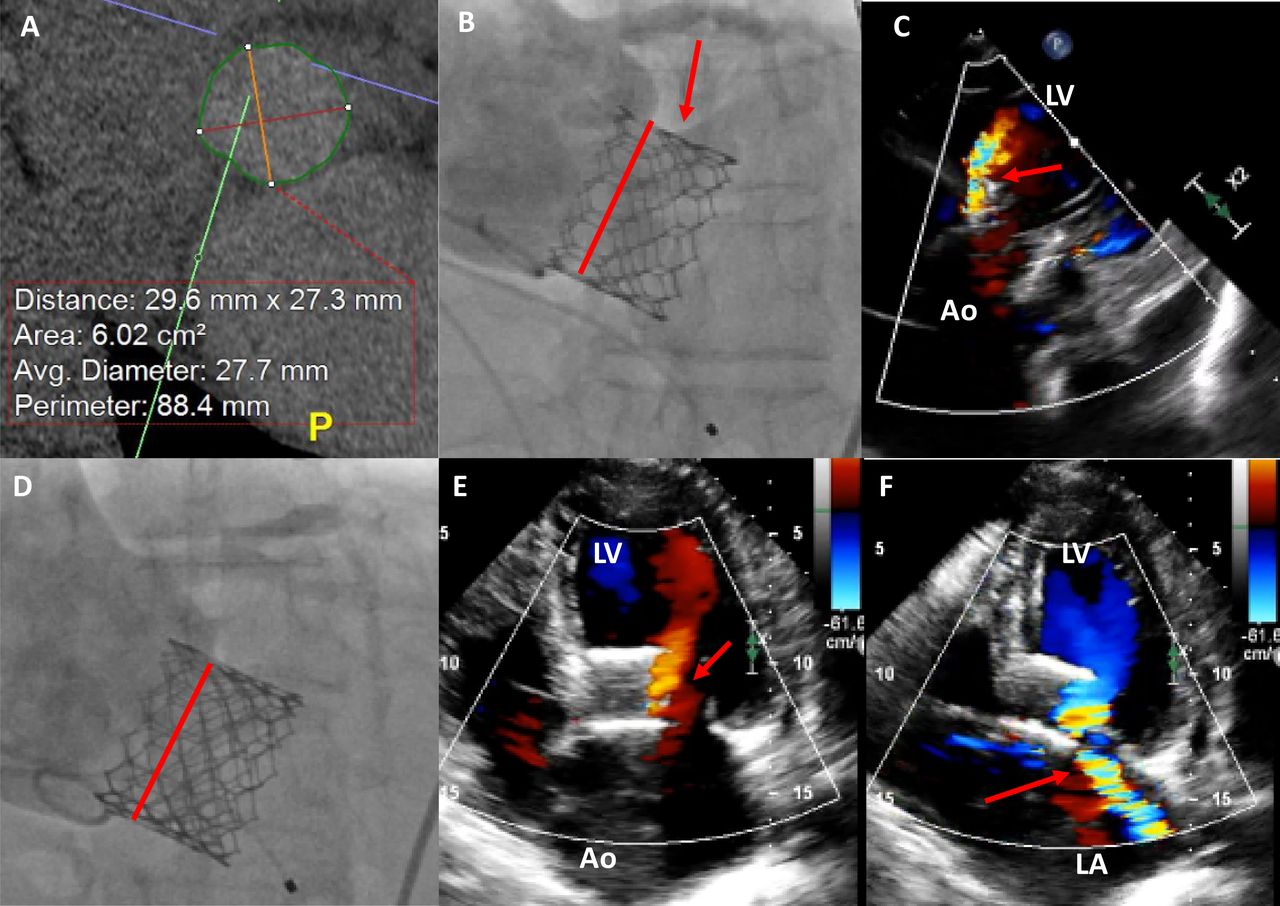
A 77-year-old man with severe AR due to aortic dilatation was referred to our Multidisciplinary Valve Clinic. His left ventricular ejection fraction was 48%. He was a high-risk surgical candidate due to chronic kidney disease and frailty. TAVI was recommended with a plan to ‘oversize’ an Edwards Sapien 3 valve. The aortic annulus cross-sectional area measured 602 mm2 with a perimeter of 88.4 mm (figure 1). He was treated with transfemoral TAVI using a 29 mm Sapien 3 valve with 5 cc over nominal fill volume (total 38 cc) to achieve a prosthesis area of ~740 mm2 (23% ‘oversizing’). Due to lack of a suitable anchoring zone for the transcatheter heart valve (THV), the valve migrated lower into the left ventricular outflow tract than intended during deployment, resulting in severe paravalvular regurgitation (online supplemental video files 1–3 and 8). A second 29 mm Sapien 3 valve was then deployed within the first valve to treat the paravalvular regurgitation. The second valve was also deployed lower into the left ventricular outflow tract than intended, but the valve-in-valve deployment resolved the paravalvular leak (online supplemental video files 4–6 and 8). The patient developed complete heart block requiring a permanent pacemaker, likely due to the over-sized and malpositioned THV. He was discharged on postoperative day #1. At 1-month follow-up, the patient reported continued shortness of breath. The transthoracic echo demonstrated moderate paravalvular regurgitation and new severe mitral regurgitation (online supplemental video files 7 and 8). CT demonstrated posterior rotation and migration of the THVs further into the left ventricular outflow tract resulting in perforation of the anterior mitral leaflet by the THV struts. The patient ultimately was treated with surgical aortic valve replacement and mitral valve repair.
Supplementary video
Supplementary video
Supplementary video
Supplemental material
Supplementary video
Supplementary video
Supplementary video
Supplementary video
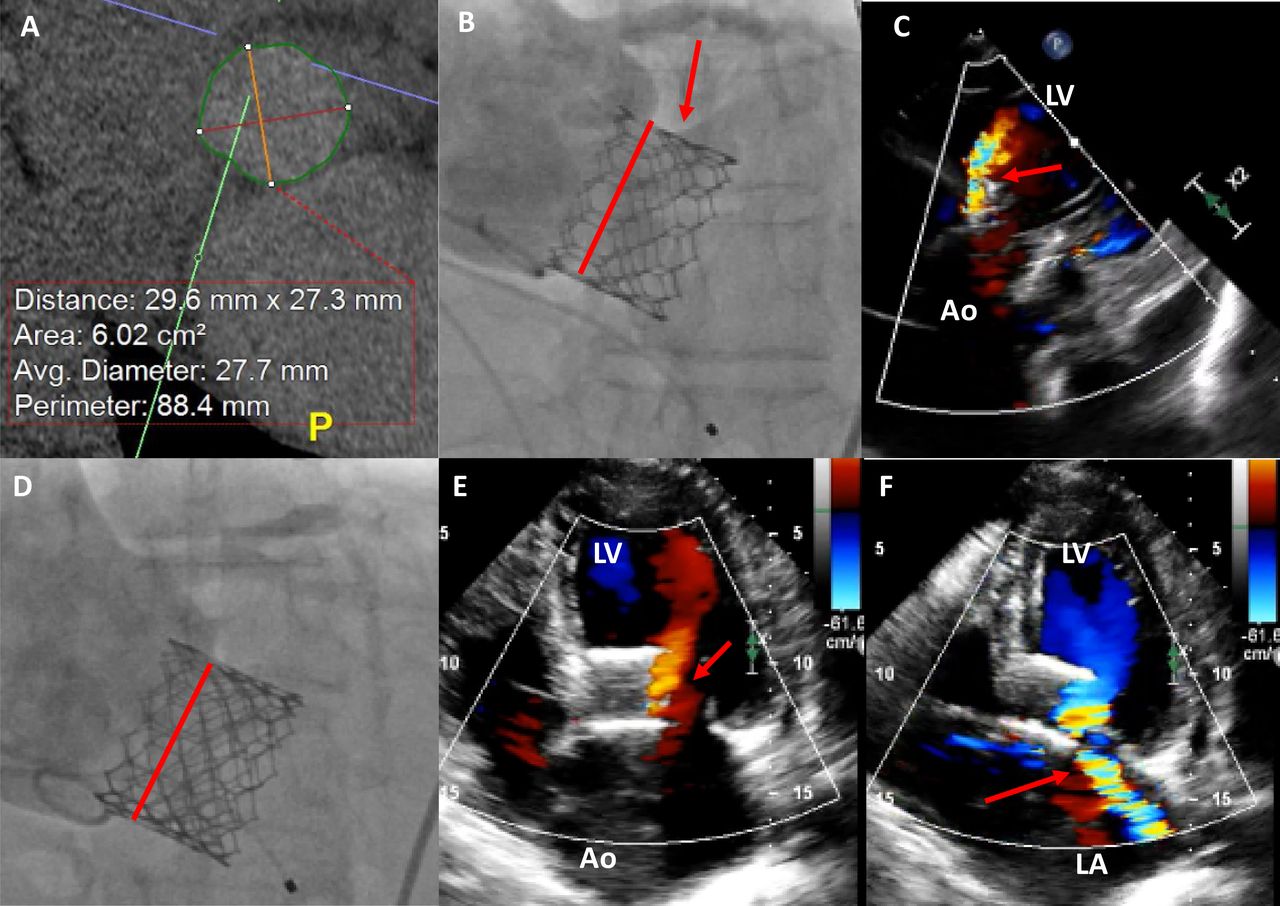
Case example of isolated severe AR treated with a Sapien 3 valve. Images for a case of a 77-year-old man with severe AR treated with an Edwards Sapien 3 THV. (A) Preprocedure four-dimensional CT showing annular dimensions and lack of significant annular calcification. (B) Cinefluoroscopy after first 29 mm Sapien 3 valve deployment showing an inadvertently deep deployment with the majority of the THV below the plane of the native annulus (red dashed line) resulting in significant paravalvular regurgitation (red arrow). (C) Transoesophageal echo after first valve deployment showing severe paravalvular regurgitation. (D) A second 29 mm Sapien 3 valve was deployed, but again landed deeper into the left ventricular outflow tract than intended (red dashed line marking native annulus), but there was no remaining paravalvular leak. (E) One month follow-up transthoracic echo shows moderate paravalvular leak and (F) severe mitral regurgitation due to ventricular migration and rotation of the THVs resulting in perforation of the anterior mitral valve leaflet. AR, aortic regurgitation; Ao, aorta; LA, left atrium; LV, left ventricle;THV, transcatheter heart valve.
Challenges with transcatheter aortic valve implantation for aortic regurgitation
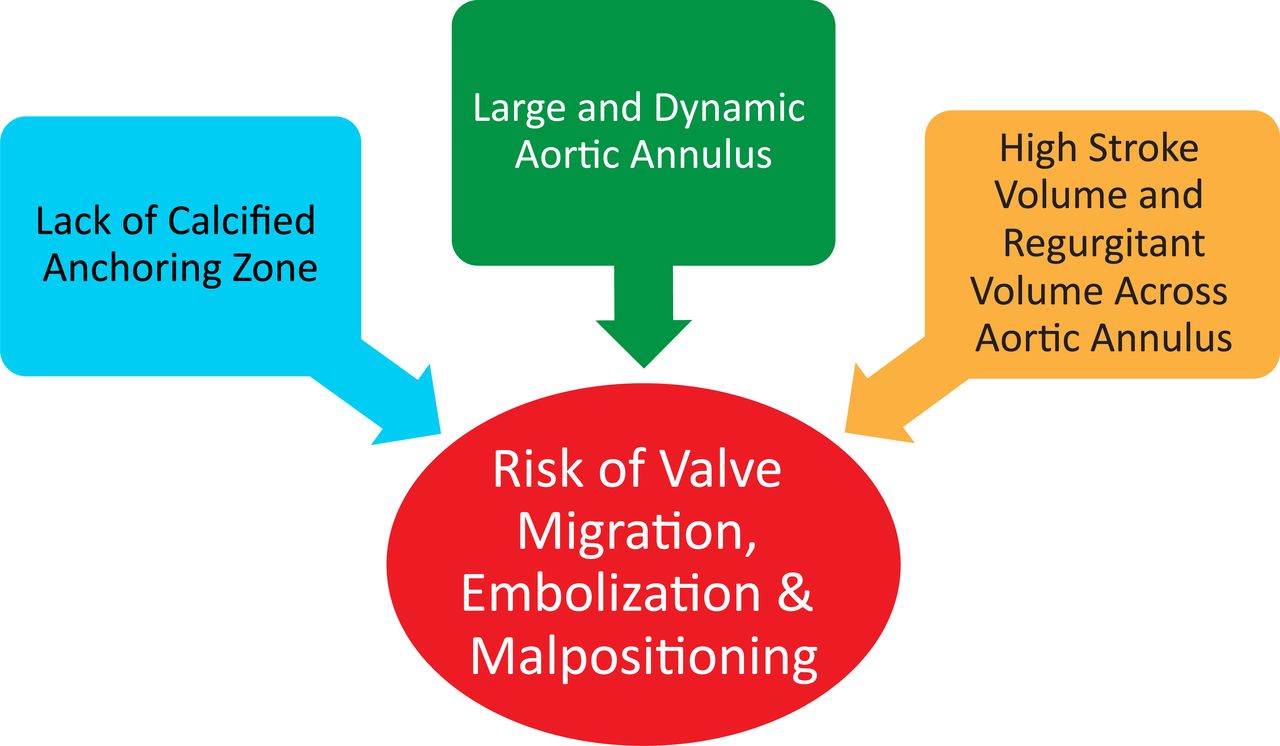
The aortic valve differs in both anatomic and physiological parameters in patients with AR compared with AS. These differences limit the safety and efficacy of TAVI with currently available devices (figure 2). The hallmark of calcific degenerative AS is leaflet calcification associated with restricted valve opening.2 In fact, the calcium score of the aortic valve as measured by CT is associated with the severity of AS and clinical outcomes, an observation which supports the pathophysiological link between calcium burden and AS severity.3 In patients with AS, the calcified and restricted leaflets provide a suitable anchoring zone for a THV, which is needed to avoid valve migration or embolisation. AR results from a variety of different processes: bicuspid aortic valve disease, rheumatic heart disease, prior endocarditis, connective tissue disorders and aortic root enlargement are several common reasons.4 However, unlike in AS, calcification is not a hallmark of the disease. In isolated AR, there is often no stable anchoring zone for a THV. One study of 42 inoperable patients with AR treated with TAVI at 14 centres demonstrated that 90.7% had no or mild aortic valve calcification, and all of the 19.0% who required an immediate second THV deployment had no aortic valve calcification.5
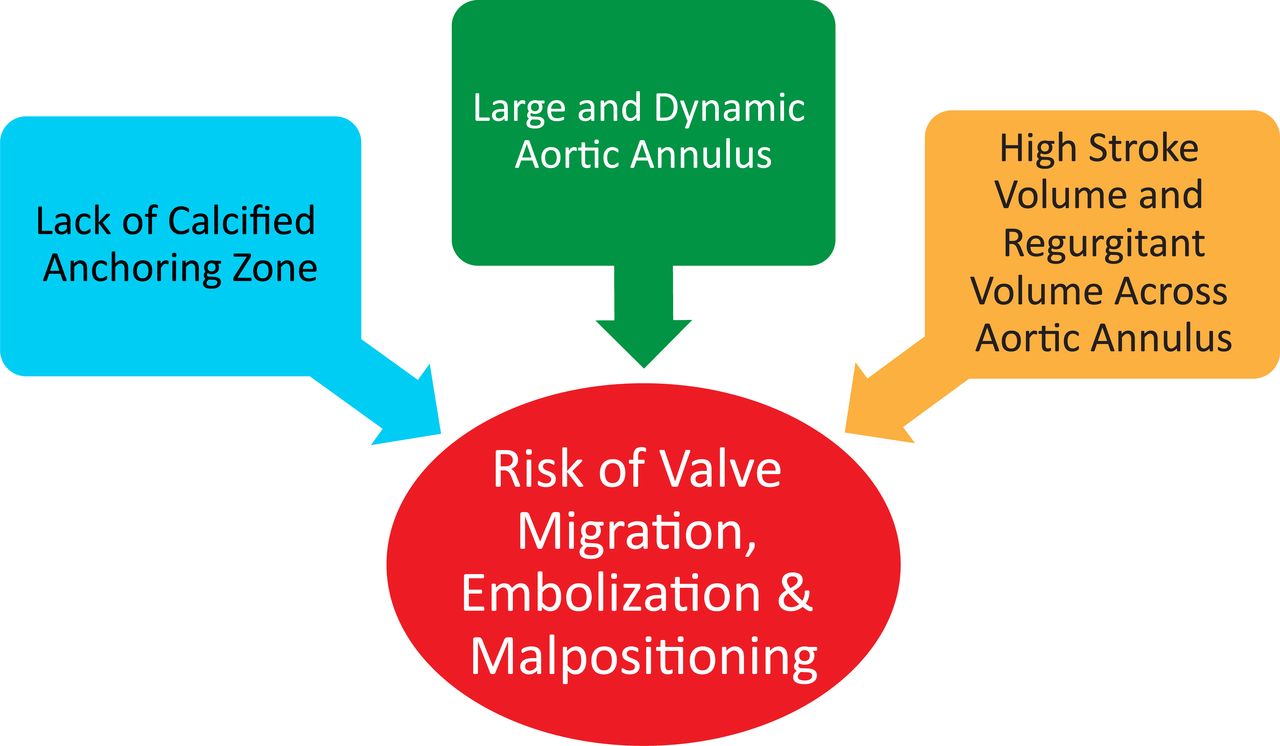
Challenges of performing transcatheter aortic valve implantation in isolated aortic regurgitation. Key anatomic and physiological aspects of isolated aortic regurgitation which contribute to technical challenges during transcatheter aortic valve implantation are shown.
One strategy which has been used to promote THV anchoring in the absence of a calcified anchoring zone has been to use an ‘oversized’ THV. A THV is typically ‘oversized’ modestly (by 10%–20% depending on valve type) for treatment of AS.5 Oversizing a THV >20% has been used as a method to reduce valve migration or embolisation in patients with AR without a suitable anchoring zone.5–7
Normally, the aortic annulus is larger and less elliptical during systole. However, these changes are somewhat blunted in patients with AS.8 While patients without AS demonstrate an 11.2%±5.4% increase in aortic annular cross-sectional area during systole, those with AS had only a 6.2%±4.8% increase in cross-sectional area during systole (p<0.001).8 A study of six patients with isolated AR who underwent four-dimensional CT angiography of the chest demonstrated more dramatic changes in aortic annular size and shape throughout the cardiac cycle than would be typical for patients with AS.9 In that study, the average aortic annular cross-sectional area increased from 4.06 cm2 to 4.99 cm2 (a 22.9% change) during systole, and the annulus took on irregular, non-circular conformations during diastole.
Patients with severe AR have high stroke volume (during systole) and high regurgitant volume (during diastole) across the aortic annulus during each cardiac cycle. In the absence of a suitable anchoring zone, this ‘to and fro’ high flow state can reduce the stability of the THV during deployment, resulting in malpositioning.
Evidence for transcatheter aortic valve implantation in aortic regurgitation
There are no randomised clinical trials and no mid-term data to support TAVI for isolated AR and medium or longer-term durability of TAVI for AR has not been established. The early postprocedural outcomes for TAVI in AR are summarised in table 1.
Summary of outcomes for TAVI in AR
When compared with outcomes of TAVI for AS,1 10 the outcomes of TAVI in patients with AR remain worse. The expected device success for TAVI in AS in real-world practice is 93%. By comparison, TAVI for AR has a device success as low as 81% even when performed with newer generation devices. Similarly, the rates of second THV deployment, moderate or greater AR or paravalvular leak, and 30-day mortality are generally worse in studies of TAVI for AR (figure 3). A recent retrospective analysis of 81 542 patients treated with TAVI (1222 or 1.5% for isolated AR, 72 690 or 89.1% for isolated AS) in the Nationwide Readmissions Database from 2016 to 217 demonstrated a higher rate of acute kidney injury (16.8% vs 9.8, p<0.001), surgical bailout (1.4% vs 0.4%, p<0.001) and death (2.4% vs 1.4%, p<0.01) in the AR procedures versus the AS procedures.11 A similar analysis of TAVI for AR in a combined cohort from the Nationwide Inpatient Sample and the National Readmissions Database reported promising outcomes with low rates of mortality, disabling stroke and open heart surgery. However, the rate of moderate or severe paravalvular leak at 30 days in that study was 7.4%, which is considerably higher than would be expected with TAVI for AS.12

{kind=link}
{kind=link}
{kind=link}
Newer vs older generation THVs for aortic regurgitation. Summary of published literature on older vs newer generation THV when performing TAVI for isolated AR.13–18 A comparison with published real world outcomes of TAVI for AS is shown with yellow bars and dotted references lines.1 10 AR, aortic regurgitation; AS, aortic stenosis; PVL, paravalvular leak; TAVI, transcatheter aortic valve implantation; THV, transcatheter heart valve.
Valve selection for transcatheter aortic valve implantation in aortic regurgitation
Selection of a specific THV device varies based on heart team discussion, anatomic considerations (annular size, aortic root size), clinical factors (age, anticipated survival) and local expertise. However, there are no head to head randomised trials of commercially available THV devices for TAVI in AR.
Newer generation THV devices have generally shown better performance for AR compared with older generation devices (figure 3). Several studies evaluated the outcomes of patients with newer generation THVs versus older generation THVs for TAVI in isolated severe AR.13–18 Older generation valves included the CoreValve (Medtronic, Minneapolis, Minnesota, USA) or Sapien/Sapien XT valves (Edwards Lifesciences, Irvine, California, USA). Newer generation valves included the Evolut R (Medtronic), Sapien 3 (Edwards Lifesciences), JenaValve (JenaValve Technology, Munich, Germany), J-Valve (JieCheng Medical Technology, Suzhou, China), Direct Flow (Direct Flow Medical, Santa Rosa, California, USA), Acurate (Boston Scientific, Natick, Massachusetts, USA), Lotus (Boston Scientific), Portico (St. Jude Medical, Saint Paul, Minnesota, USA) and Engager (Medtronic) valves. These studies (multicentre registries, systematic reviews and meta-analyses) reported substantially lower rates of second THV deployment, residual AR and mortality with higher procedural success among patients treated with newer generation THVs compared with older generation THVs. However, most new generation THVs described are not commercially available in the USA (only the Sapien 3 and Evolut series are available).
Future directions
There are encouraging early data to support on-going device development and clinical trials. The Accurate neo valve is a newer-generation self-expanding THV with supra-annular stabilisation arches which was designed for use in patients with AS. In small series, the Accurate neo valve has shown mixed results in AR.19 20 The JenaValve and J-Valve are two devices which do not require a calcified anchoring zone. These devices carry the CE mark for ‘on-label’ treatment of AR. Based on its promise as a potential therapy for patients with AR, the JenaValve has been designated as part of the US Food and Drug Administration’s Breakthrough Device Program. The trans-apical J-Valve system has also shown impressive early results with low rates of significant AR and high rates of device success.21 22
Conclusion
TAVI for AR is becoming increasingly feasible with newer generation devices, but outcomes still lag behind the high benchmark established for TAVI in patients with AS. There are no randomised controlled trials and no mid-term data to support the routine application of TAVI for isolated AR. Emerging devices which do not require a calcified anchoring zone show promise, but data on these devices are limited and clinical investigation is ongoing. Randomised clinical trials are needed to establish TAVI as a safe and effective treatment for isolated AR.
Based on the available evidence, the practice at our centre is to offer TAVI for native AR only for inoperable patients. Features which may improve the success of TAVI for native AR include calcified aortic annulus, calcified aortic valve leaflets or mixed AS/AR. Exclusions for TAVI in native AR are patients with acceptable surgical risk, active infective endocarditis, concomitant ascending aortic aneurysm which requires surgical treatment and those with very large aortic annular size which cannot be treated with commercially available THVs.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @akcmahi
Contributors CPH contributed to the planning, drafting and revision of this review article. KBA contributed to the planning, drafting and revision of this review article. AC contributed to the planning, drafting and revision of this review article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KBA: Abbott Vascular: Consultant, Research Support, Speakers Bureau; Edwards Lifesciences: Consultant, Research Support, Speakers Bureau; Medtronic Inc: Consultant, Research Support, Speakers Bureau. AC: Abbott Vascular: Speakers Bureau; Boston Scientific: Consultant, Research Grant; Edwards Lifesciences: Proctor, Speakers Bureau; Medtronic Inc: Proctor, Speakers Bureau.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; externally peer reviewed.