Article Text

Abstract
The National Service Framework (NSF) established coronary heart disease as a priority area for the government and for the National Health Service (NHS). In the three and a half years since its launch, good progress has been made and the NSF is already delivering real improvements for patients, demonstrated by a near 25% reduction in the death rate from circulatory diseases. Prescribing of cardiovascular drugs for secondary prevention has increased, acute myocardial infarction is being treated more promptly, and there is improved access to revascularisation procedures. However, there is still a notable class differential in cardiovascular deaths. There has been exponential growth in use of statins but the drugs are still not being used to optimum effect. Heart failure has now been identified as a priority for action.
- cardiovascular care
- National Health Service
- National Service Framewor
- coronary heart disease
- CABG, coronary artery bypass graft surgery
- CHD, coronary heart disease
- MINAP, Myocardial Infarction National Audit Project
- NSF, National Service Framework
- NHS, National Health Service
- NICE, National Institute for Clinical Excellence
- PCT, primary care trust
- SMR, standardised mortality ratio
Statistics from Altmetric.com
- CABG, coronary artery bypass graft surgery
- CHD, coronary heart disease
- MINAP, Myocardial Infarction National Audit Project
- NSF, National Service Framework
- NHS, National Health Service
- NICE, National Institute for Clinical Excellence
- PCT, primary care trust
- SMR, standardised mortality ratio

The Department of Health collects data on developments in the management of cardiovascular disease from several sources. These include research evidence, examples of modernised practice, national audit and benchmarking data, and other health systems, such as the Kaiser Permanente in the USA, from which much can be learnt in terms of integrated care and systematic work.
At a macro level, departmental policy includes the National Service Framework (NSF) programme and defining priority areas, The NHS plan, Shifting the balance of power, and Building on the best: choice, responsiveness and equity in the NHS, which was piloted in the cardiac arena and essentially aims to make the National Health Service (NHS) a more patient focused organisation. Micro-level policy relates to action within clinical areas (including emerging treatments and approaches to treatment), working with the National Institute for Clinical Excellence (NICE) and ensuring that the NSF programme is up to date.
The NSF for coronary heart disease (CHD),1 which is now three and a half years old, set the agenda for the modernisation of CHD services in England over a 10 year period and defined milestones by which progress could be measured. The NSF set standards for improved prevention, diagnosis, treatment, and rehabilitation and goals to secure fair access to high quality services. It established CHD as a priority area for government and for the NHS. This meant that money was made available and, to date, around £800 million new money has been spent.
CHD has also been identified as a priority area for health improvement in Wales2 and Scotland.3
The NSF target, first set out in the White Paper Saving lives: our healthier nation, is to reduce the death rate from circulatory diseases in people under 75 years by 40% by 2010. The death rate has already been reduced by 23.4% from the 1995–7 baseline. This suggests that the target 40% reduction will be achieved by around 2006, four years earlier than expected.
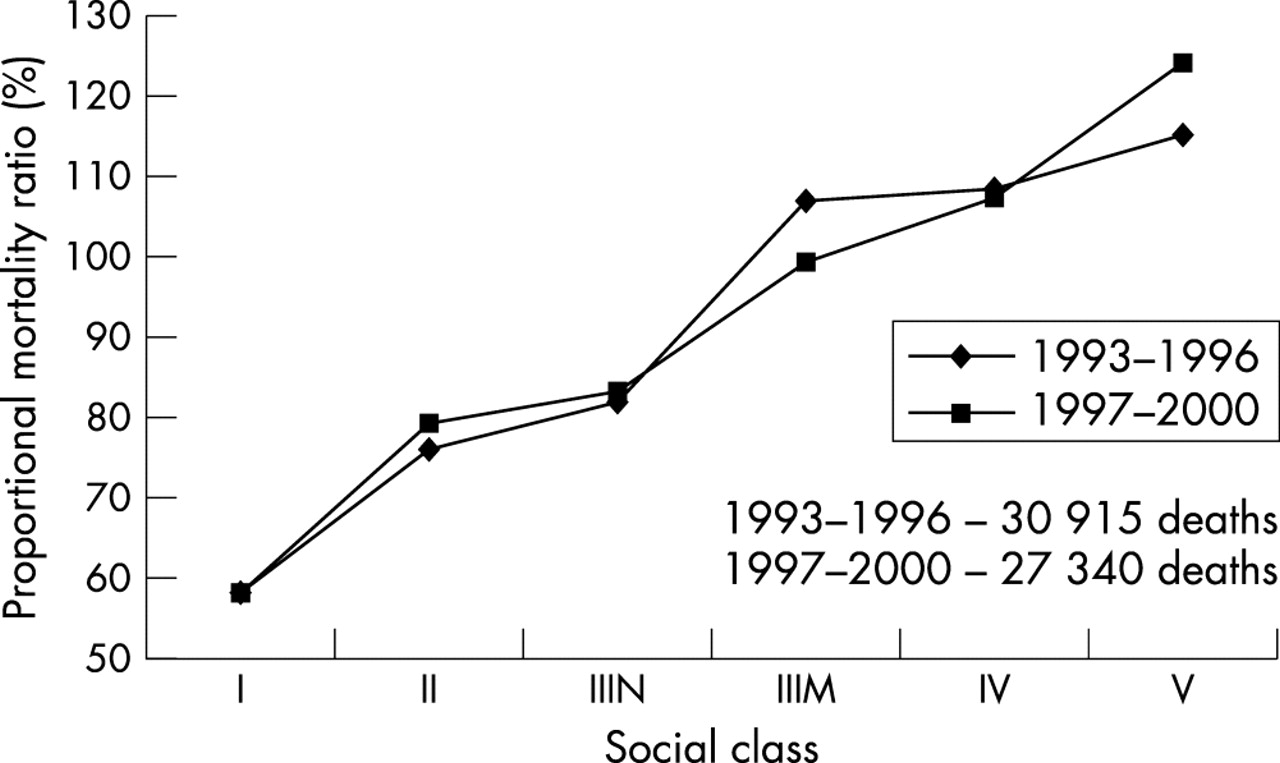
However, although there is a 6.5% annual reduction in cardiovascular deaths, there is still a notable class differential (figs 1 and 2). Recent data from the Office of National Statistics show how the proportional mortality ratio in men increases from social class I to social classes IV and V, although there has recently been an improvement in social class V. In women, the class differential is even greater.

Proportional mortality ratio for cardiovascular deaths in England by social class in males aged 35–64. I, professional occupations; II, managerial and technical occupations; III, skilled occupations; N, non-manual; M, manual; IV, partly-skilled occupations; V, unskilled occupations.
Proportional mortality ratio for cardiovascular deaths in England by social class in females aged 35–64. See fig 1 caption for explanation of social classes.
Smoking cessation is a key plank of the Department of Health’s public health programme. Tobacco advertising has been banned and there is a major programme of smoking cessation services; to date, 250 000 people have been helped to quit for at least four weeks. A new component of the public health programme is the school fruit scheme in which a free piece of fruit is given each school day to children aged 4–6 years. The scheme currently reaches nearly one million children in around 7000 schools.
SECONDARY PREVENTION
In addition to these broad based public health programmes, there has been a drive to improve secondary prevention. The primary care collaborative concentrates about one third of its time on secondary prevention. In addition, the CHD collaborative has been influential in helping primary care to establish CHD registers, which now exist in some 90% of practices, and general practitioners and nurses with special interest are contributing in a major way to the secondary prevention programme. There has been significant investment in equipment from the Treasury Capital Modernisation Fund.
Data from practices in the Wirral demonstrate how these approaches to cardiovascular prevention can make a difference. There are three primary care trusts (PCTs) in the Wirral: Wallasey and Birkenhead PCTs are in relatively deprived areas with initially high standardised mortality ratios (SMRs), while Bebington & West Wirral PCT covers a more prosperous area. In all three communities there has been a decline in SMR, but the most dramatic fall has been in the most deprived area, Wallasey, where the SMR is now 94 compared with around 120 in 1981–5. Similar data are available from other local communities demonstrating the difference that can be achieved (A Cummins, personal communication).
STATIN PRESCRIBING
It is too early to say how much of the improvement is related to use of statins, but there has been exponential growth in prescribing of these drugs in primary care. When the NSF was published in 2000, the quarterly net ingredient cost for statins in England was around £65 million; the figure is now £174 million. That is £13 million a week— or £1.9 million a day. If, as expected, growth in statin prescribing continues at the current rate, it is likely to reach the £2.1 billion cost per year predicted in the 2002 Wanless report on long term funding of the NHS. That would mean general practitioners in England writing 66 million prescriptions a year, leaving little time to do anything else. New ways will therefore have to be found to deliver the agenda.
Benchmarking data show a wide variation in statin prescribing rates by strategic health authorities. Encouragingly, prescribing tends to be highest in the areas where there is the highest level of coronary disease, such as Cheshire & Merseyside, Northumberland, Cumbria & Lancashire, Kent & Medway, County Durham, and Greater Manchester. Kent & Medway is interesting because the high level of prescribing is related to a prescribing incentive scheme. The scheme is similar to the new general practitioner contract, and so the results are probably a measure of things to come.
In 2002/3 an estimated 6700 lives were saved in England as a result of statin prescribing. However, the “rule of halves” has been found now to apply to statin usage. A study carried out by the informatics group at St George’s Hospital, London, collected data from 25 PCTs around the country and identified some 76 000 patients with CHD: only half of the patients had a valid cholesterol measurement; only half of those were being prescribed statins; and only half of those were achieving target cholesterol values.4 This demonstrates that there is still work to do. The issue of lipid management has now been referred to NICE for development of a guideline.
Prescribing of other cardiovascular drugs has also increased. Prescription Pricing Authority data show that, comparing the quarter to March 2000 (before the NSF) and the quarter to December 2002, there has been a 54% increase in net ingredient cost of cardiovascular drugs, rising from £300 million to £460 million. That equates to 12 million more prescriptions per quarter, which can be taken as a surrogate marker of how much work has been going on in primary care.
ACUTE CARE
In acute care, one of the key challenges was treatment of acute myocardial infarction. The Myocardial Infarction National Audit Project (MINAP), to which all trusts are enrolled, now has data on 150 000 episodes of care. Ambulances are being equipped with ECGs and with telemetry facilities so that acute myocardial infarction patients can be diagnosed before arrival at the hospital. There are also moves towards a national training programme to allow paramedics to administer pre-hospital thrombolysis. This will pave the way for paramedics to triage patients, so that with a gradual move to a system of primary angioplasty as the main treatment of choice, they can make sure that the patient is taken to an appropriate hospital.
A public access defibrillation programme has been set up. So far there are 680 automated external defibrillators at 110 sites, 4000 people have been trained to use them, and an estimated 21 lives have been saved.5
Ambulance response times have improved. The average now is 75% response to acute calls within eight minutes. In addition, hospitals have substantially improved their performance in treating myocardial infarction: MINAP data show that 79% of patients are now treated within 30 minutes of hospital arrival5 (fig 3) and the median “door to needle” time is just over 20 minutes — in the USA, the equivalent figure is 46 minutes.6

Proportion of patients receiving thrombolytic treatment in England within 30 minutes of hospital arrival.
Use of secondary prevention in acute myocardial infarction patients has increased. Prescribing is on target for aspirin (given to 96% of discharged patients), angiotensin converting enzyme inhibitors (about 80%) and β blockers (nearly 90%), and statins are given to almost all patients eligible under current guidelines.5
DIAGNOSIS AND ACCESS
One of the building blocks for improving diagnosis and access was the setting up of rapid access chest pain clinics. The target was to have 100 clinics by April 2002; in the event there were 182. Roll out across the country is now complete and 82% of patients with new onset angina are seen within two weeks. The target is 100%.
Over £380 million has been invested in capital schemes across the country to improve access to coronary revascularisation procedures. As a result, the NHS plan for 6000 extra heart operations by 2003 was achieved one year early and there has been a substantial improvement in waiting time for surgery. Since March 2003, no patients have waited more than nine months for coronary artery bypass graft surgery (CABG). The number of patients waiting six months was reducing steadily until April, since when it has levelled out due to revascularisation money going into the general allocation. However, in September there were only 373 patients waiting more than six months for CABG, which is a remarkable turnaround in the three years since the NSF was launched.
The number of angioplasty procedures carried out has grown exponentially and the ratio will soon be around 2:1 for angioplasty to CAGB. Two strategic health authorities (North West London and South West Peninsular) have already achieved the 2008 NSF target of 1500 revascularisation procedures per million population. They have largely done this through increased angioplasties. In some strategic health authorities, particularly in the north, CABG is still more common than angioplasty, but the department is looking to expand angioplasty activity in these areas.
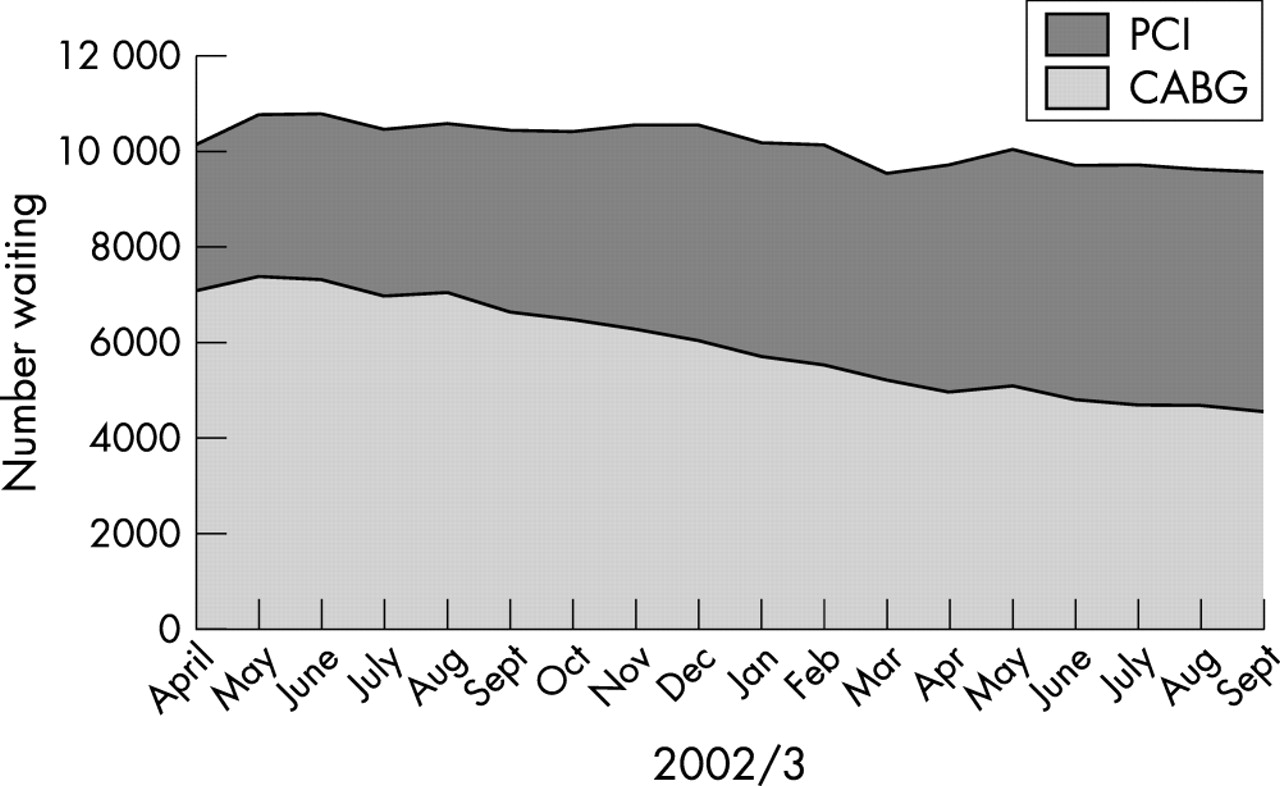
Waiting pressure now relates to angioplasty rather than to CABG (fig 4). To ease this pressure, the Department of Health and the New Opportunities Fund have a £125 m national catheter laboratory investment scheme to fund 86 new laboratories, many in District General Hospitals, which will provide a 54% increase in capacity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patients waiting for revascularisation procedures in England. CABG, coronary artery bypass graft surgery; PCI percutaneous coronary intervention.
HEART FAILURE
Heart failure has also now been identified as a priority area. Action to date includes commissioning the NICE heart failure guideline, purchase of 60 new echocardiography machines, and a workforce project aimed at developing the capacity of clinical physiologists.
Over the past few years, there has been a decline in the number of patients admitted to hospital with heart failure, which is probably a measure of more effective treatment. However, with the aging population and the increased number of survivors of myocardial infarction, the country could be facing an epidemic of heart failure.
The current target is to improve management in line with the NICE guideline and to set local targets for the reduction in patients admitted to hospital with a diagnosis of heart failure. This requires primary and secondary care services to work together to make sure that their skill base is used as efficiently as possible. A resource, Developing services for heart failure,7 has been produced to help with implementation of the guideline.
CONCLUSION
The strategies for CHD are beginning to make a difference. This shows that national policy, if properly resourced and supported, empowers clinicians to carry out the work.