Article Text

Abstract
Acute pulmonary hypertension (PH) complicates the course of several cardiovascular, pulmonary and other systemic diseases in children. An acute rise of RV afterload, either as exacerbating chronic PH of different aetiologies (eg, idiopathic pulmonary arterial hypertension (PAH), chronic lung or congenital heart disease), or pulmonary hypertensive crisis after corrective surgery for congenital heart disease, may lead to severe circulatory compromise. Only few clinical studies provide evidence on how to best treat children with acute severe PH and decompensated RV function, that is, acute RV failure. The specific treatment in the intensive care unit should be based on the underlying pathophysiology and not only be focused on so-called ‘specific’ or ‘tailored’ drug therapy to lower RV afterload. In addition therapeutic efforts should aim to optimise RV preload, and to achieve adequate myocardial perfusion, and cardiac output. Early recognition of patients at high risk and timely initiation of appropriate therapeutic measures may prevent the development of severe cardiac dysfunction and low cardiac output. In patients not responding adequately to pharmacotherapy, (1) novel surgical and interventional techniques, temporary mechanical circulatory support with extracorporeal membrane oxygenation, (2) pumpless lung assist devices (3) and/or lung or heart-lung transplantation should be timely considered. The invasive therapeutic measures can be applied in a bridge-to-recovery or bridge-to-lung transplant strategy. This consensus statement focuses on the management of acute severe PH in the paediatric intensive care unit and provides an according treatment algorithm for clinical practice.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Despite recent advances in the specific treatment of pulmonary hypertension (PH), RV failure following or in the context of severe rise of pulmonary vascular resistance (PVR) is a challenging complication of PH and is associated with substantial morbidity and mortality.
PH leading to a decompensation of the cardiovascular system can be considered a syndrome with non-specific signs and symptoms presenting late in the disease process and may be strongly associated with, or directly caused by several, very heterogeneous underlying conditions.1 Distinction between precapillary and postcapillary aetiologies (or establishment of a combination of the two) is important to initiate specific individual therapy.
Pathophysiology of acute PH and RV failure
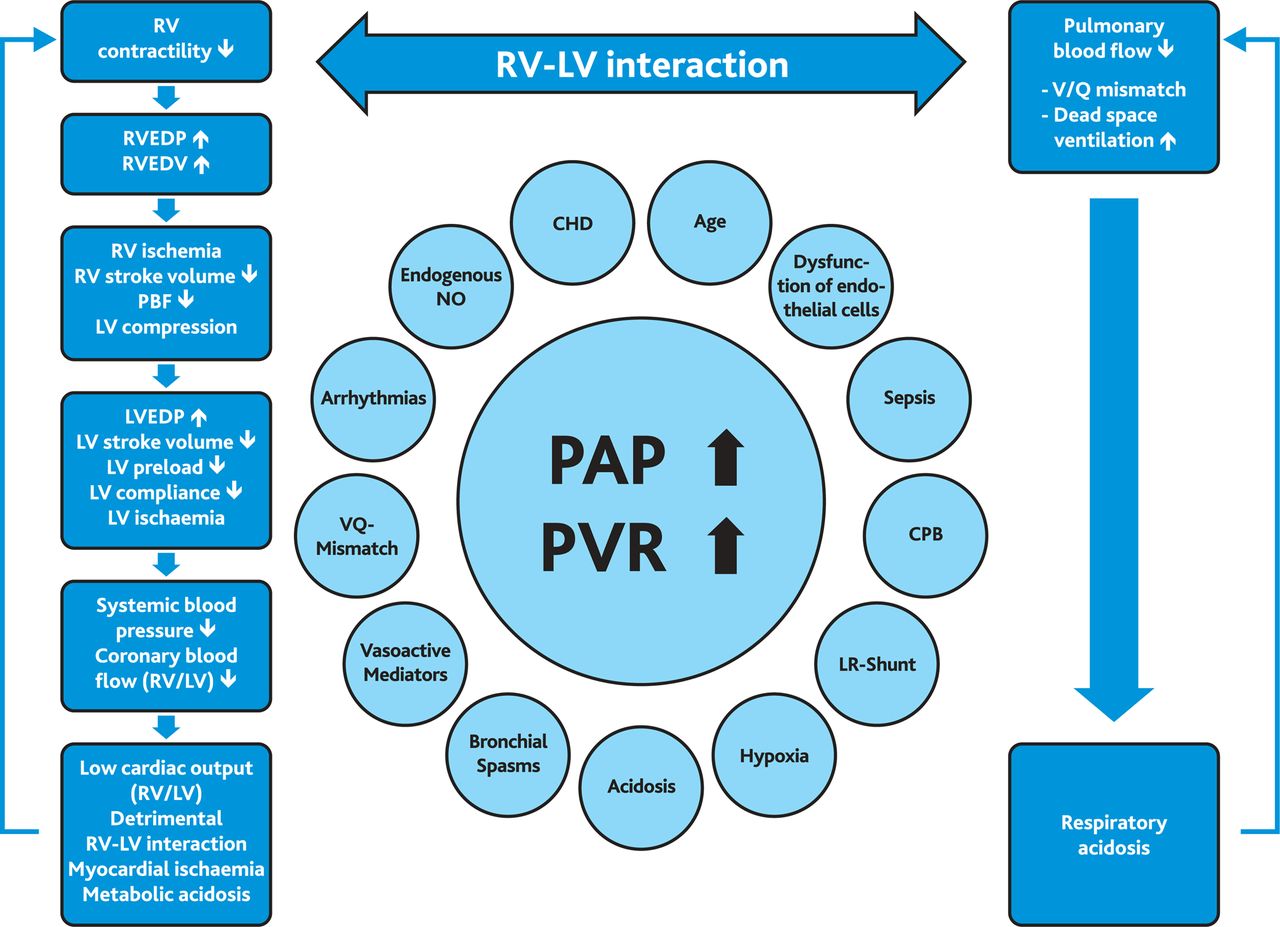
Chronic PH causes adaptation and remodelling of the RV to increased loading conditions. Pulmonary hypertensive crisis (PHC) occurs when compensatory mechanisms fail, RV systolic function decompensates and LV preload acutely decreases resulting in abolished cardiac output and coronary perfusion.2 ,3 Acute elevation of afterload (pulmonary artery pressure (PAP)) is poorly tolerated by the unprepared RV. In healthy adult individuals, the RV cannot acutely generate a mean PAP >40 mm Hg.4 Adaptive changes of the RV microstructure and function do not work in the setting of acute rise of RV afterload. Thus, although myocardial contractility may initially rise with RV concentric hypertrophy and preserved systolic and diastolic function, excessive pressure overload results in maladaptive remodelling with RV dilatation and failure.5 Among many others, arrhythmia, myocardial ischaemia and/or pulmonary disease such as infections or pulmonary arterial embolism may trigger an acute rise of PAP and PVR (figure 1). With subsequent RV dilatation, the contractile sarcomere apparatus is damaged, resulting in RV failure. The combination of right-to-left septal shift with subsequent LV compression, related to limited space within the pericardial sac, results in low LV output, systemic arterial hypotension and elevated LV and RV end-diastolic pressure. With or without RV hypertrophy, these factors decrease coronary perfusion leading to myocardial ischaemia that perpetuates RV failure.6 The resulting metabolic acidosis further increases PVR and PAP. Moreover, a sudden increase in PAP causes airway obstruction due to arterial distension of the smaller intrapulmonary arteries and lung oedema. The resulting dead space ventilation and ventilation/perfusion mismatch causes hypoxia and respiratory acidosis, eventually resulting in even more elevated PAP and PVR (figure 1).2 ,3 ,7
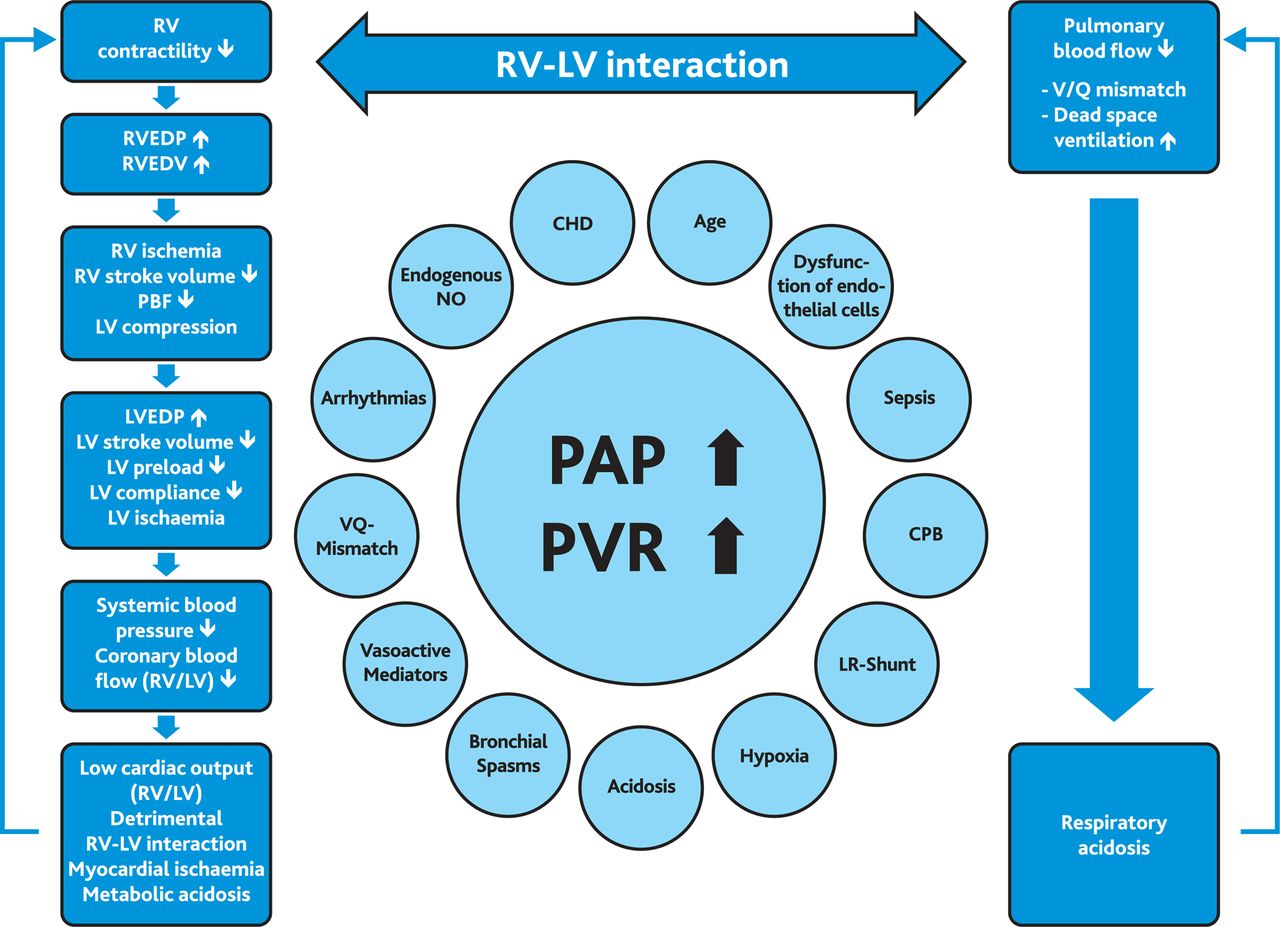
Schematic drawing of PAH crisis and contributing factors. Pulmonary hypertensive crisis develops with an acute increase of PAP. This leads to an increase in RV pressure and volume causing a shift of the interventricular septum towards the left side and reducing LV volume. Filling pressures of ventricles rise, compensatory tachycardia and the drop in systemic blood pressure compromise coronary perfusion pressure and flow, leading to low cardiac output and metabolic acidosis. Furthermore, the increase in PAP causes decreased pulmonary blood flow and airway obstruction related to arterial distension of the smaller intrapulmonary arteries and lung oedema. Consequently dead space ventilation increases; together with a mismatch of pulmonary ventilation and perfusion this causes hypoxia and respiratory acidosis. PAH, pulmonary arterial hypertension; RVEDV, RV end-diastolic volume; RVEDP, RV end-diastolic pressure; LVEDP, LV end-diastolic pressure; V/Q, pulmonary ventilation and perfusion; PAH, pulmonary arterial hypertension; PAP, pulmonary artery pressure; PVR, pulmonary vascular resistance; CHD, congenital heart disease; NO, nitric oxide; CPB, cardiopulmonary bypass; LR-Shunt, left-to-right shunt; PBF, pulmonary blood flow.
In children with congenital heart disease (CHD) and systemic-to-pulmonary shunt, PH crisis may occur following corrective surgery. Factors that promote the development of postoperative PH are not yet completely understood, however, endothelial cell dysfunction was found to be a contributing factor preoperatively and postoperatively.8–10 Inflammatory response to cardiopulmonary bypass, and ischaemia-reperfusion injury and its impact on heart-lung function contribute to the rise in PVR.11 Pain, awakening reactions in mechanically ventilated children, tracheal secretions or tracheal suctioning may trigger acute severe elevation of PVR presenting as PHC and potentially leading to cardiocirculatory collapse and death (figure 1).
In this consensus statement, we distinguish between and elaborate on three common scenarios: (1) acute PH crisis after cardiac surgery for CHD, with different management strategies subdivided for patients with univentricular and biventricular physiology (2) acute deterioration in a child with previously known chronic PH (eg, a child with chronic parenchymal lung disease and acute viral chest infection and acute deterioration in a child with new diagnosis of group 1 PH (pulmonary arterial hypertension (PAH), eg, idiopathic PAH), and (3) secondary PH.12 We finally focus on the rapid assessment and efficient management of acute severe PH in the paediatric intensive care unit (PICU), including concise recommendations and a treatment algorithm for clinical practice.⇓
Recommendations on the therapy of acute pulmonary hypertension in the paediatric ICU
Methods
The recommendations given in table 2 relate to the grading system currently suggested by the European Society of Cardiology (ESC) and the American Heart Association (AHA), and was based on paediatric data only (class of recommendation, level of evidence). The grading and voting process within the writing group is outlined in the executive summary13 of this online supplement. Computerised searches of the PubMed/MEDLINE bibliographical database were conducted between 1990 and June 2015. Clinical trials, guidelines and reviews limited to paediatric data were searched using the terms ‘pulmonary hypertension’ and ‘intensive care’, ‘heart failure’, ‘congenital heart’, ‘postoperative’, ‘surgery’, ‘ECMO’, ‘lung assist’, ‘ventricular assist’, ‘mechanical circulatory support’, ‘cardiopulmonary bypass’, and ‘pulmonary hypertensive crisis’. The primary focus of this manuscript is on group 1 PH according to the World Symposium on Pulmonary Hypertension (WSPH) Nice classification.12 Group 2 PH requires a separate discussion that is beyond the scope of this article.
Medications used for treatment of pulmonary hypertension in the intensive care unit
Initial assessment and monitoring of children with acute PH
Acute elevation of PVR is a life-threatening event that may rapidly lead to cardiorespiratory collapse. During the initial assessment, the following questions have to be addressed:
Is the PH associated with systemic hypotension and/or hypoxaemia, low AVDO2, and thus most likely low cardiac output and tissue hypoxia?
Are there any precipitating factors that might be responsible for elevated PVR and RV dysfunction (eg, infection, acidosis, arrhythmia, pericardial effusion)?
Are there any other causes that could explain the symptoms of PHC and RV failure (eg, pneumothorax, pulmonary embolism)?
After the initial clinical assessment of vital signs, chest X-ray and transthoracic echocardiography are mandatory to guide therapy. Monitoring of haemodynamics and organ function (brain, liver, kidney, coagulation system, etc) is an essential part of the routine set-up and procedures in the PICU.1
ECG
Signs of right atrial dilatation, right axis deviation, right bundle branch block or RV hypertrophy are typically seen in patients with chronic PH.14 ,15 In patients who have undergone surgery for CHD, the ECG may still display changes that occur with the underlying heart defect, but sometimes it may be normal. Loss of sinus rhythm (eg, in atrial flutter or junctional tachycardia) is an important diagnosis as it aggravates RV failure.
Chest X-ray
Chest X-ray helps to differentiate between PH with and without ventilation-perfusion mismatch and may show involvement of one or both lungs. In addition, in patients with chronic or newly diagnosed PH, signs of enlargement of the right heart and central pulmonary arteries are typically present. In more severe cases, one may recognise peripheral rarefication of the pulmonary vasculature (increased radiotranslucency of the lung fields). However, right heart enlargement may be best seen in the lateral plane (radiopaque retrosternal space that is filled by the dilated RV). In patients with underlying CHD, changes on the chest X-ray can be related to the cardiac lesion itself.15 ,16
Echocardiography
Echocardiography is the most important tool for the assessment of ventricular function and RV-LV interaction.17 Doppler analysis of tricuspid valve and pulmonary valve regurgitation to estimate PAP and diastolic inflow characteristics of both ventricles may help in guiding therapy in the ICU. The estimated PAP and right ventricular systolic pressure (RVSP) need to be interpreted in the context of the degree of RV dysfunction. Low pressure gradients across the tricuspid and pulmonary valves may be due to RV failure; they should be seen in relation to other variables (eg, tricuspid annular plane systolic excursion (TAPSE), and in light of the presence or absence of pericardial and pleural effusions, or ascites. If pulmonary vein obstruction is excluded, in most cases, the enlarged left atrial dimension defines the postcapillary component of PH and may indicate the need for decompression of the left atrial pressure through atrial septum stenting. Especially after cardiac surgery, the patient's anatomic and haemodynamic status must be determined and taken into consideration.
Invasive monitoring
Invasive monitoring with an arterial and a central venous line should be established in all patients with cardiopulmonary compromise in whom vasopressor or inotropic therapy may be necessary. Insertion of invasive lines should be done with sufficient local anaesthesia and adequate analgosedation. Additional general anaesthesia might be hazardous (see anaesthesia and ventilation). Invasive monitoring is also indicated in patients at risk for systemic hypotension secondary to PH targeted therapy, even if this does not include vasopressor/inotropic therapy. There is a broad controversy on the most useful way to haemodynamically monitor a child with PH, in particular, we cannot make a clear recommendation for or against invasive PAP monitoring/Swan-Ganz catheters, in the PICU. Measurement of filling pressures of both ventricles may be of value to guide fluid management and escalation of therapy in distinct scenarios.
Therapy of acute PH in the ICU
Basic measures in the ICU
Oxygen
As a potent pulmonary vasodilator and a weak systemic vasoconstrictor, oxygen is indicated in children with ventilation-perfusion mismatch based on arterial oxygen saturations of less than 95% (figure 2). Sufficient supply prevents anaerobic metabolism in peripheral organs.2 In children with systemic-to-pulmonary shunts, supplemental oxygen augments pulmonary overcirculation with the risk of worsening cardiac and pulmonary function. In cyanotic heart disease with pulmonary-to-systemic (right-to-left) shunt flow, a higher haemoglobin level and shunt flow guarantees adequate systemic oxygen delivery. In these patients, oxygen is indicated in concomitant parenchymal lung disease or in deep cyanosis; arterial oxygen saturations of 75–85% are generally accepted as sufficient.

Algorithm for management of acute pulmonary hypertension in the ICU. CPP, coronary perfusion pressure; CPR, cardiopulmonary resuscitation; CVP, central venous pressure; FBC, full blood count; ICU, intensive care unit; LFT, lung function test; /(slash) indicates “or”; SBP, systemic blood pressure; SvO2, systemic venous oxygen saturation, Lact: lactate, SVR, systemic vascular resistance; TR, tricuspid regurgitation; VA-ECMO, venoarterial extracorporeal membrane oxygenation.
Alkalisation
Alkalisation is effective for immediate treatment of PH crisis.18 ,19 Acidosis elevates PVR and impairs the effect of inotropic and vasopressor drugs.18 Therefore, acidosis, as measured by negative base excess, should be abolished. Alkalisation with sodium bicarbonate to achieve a pH of 7.44 resulted in significantly reduced PVR.18 Of note, neurodevelopmental outcome might be negatively affected after prolonged hypocapnic alkalosis in newborns.20
Sedation
Anxiety and agitation increase PVR and oxygen consumption and should be avoided. Sedation of a critically ill child has to be done with caution: in spontaneously breathing patients, hypoventilation and apnoea have to be avoided. In ventilated patients, loss of sufficient LV preload together with substantial decrease of systemic vascular resistance (SVR) can lead to circulatory arrest due to loss of coronary perfusion pressure.
Anaesthesia and ventilation
Anaesthesia, intubation and insertion of invasive lines are among the most crucial steps in the management of a child with imminent deterioration. Mechanical ventilation is indicated in severe PH with profound cyanosis, respiratory or metabolic acidosis not responding to initial therapy, respiratory failure or in cardiocirculatory arrest. In patients responding to medical therapy mechanical ventilation should be avoided. Anaesthesia should be performed by the most experienced person available. Induction is usually started with a rapidly acting sedative and muscle relaxant and may be followed by an opioid. Data regarding ketamine are ambigous because its effect on PVR depends on comedication.21 Induction of anaesthesia for intubation may cause a pronounced fall in SVR, and circulatory collapse. To overcome the fall in SVR vasopressor support may become necessary. Nursing care and respiratory therapy of ventilated patients requires awareness of cardiopulmonary interactions. Manoeuvres triggering pulmonary hypertensive crises such as insufficient sedation, rise of pCO2 or suctioning should be avoided. Moreover, positive pressure ventilation impairs cardiac filling and output22 especially in the failing RV. Normoventilation (pCO2-levels 35–40 mm Hg) and long expiratory times are recommended. Hyperventilation reduces cardiac output, increases SVR19 and induces lung injury. In patients with failing RV or in univentricular circulation, the pulmonary perfusion pressure (flow) in relation to mean airway pressure has to be monitored to guarantee sufficient pulmonary flow.
Fluid management
RV function in neonates and patients with significant PH is preload dependent. Volume loss is poorly tolerated and in an acute PH crisis, volume challenge may be useful, but haemodynamic monitoring is mandatory. On the other hand, chronic RV failure is associated with fluid overload and systemic venous congestion. Nevertheless, rapid fluid removal with diuretic therapy or haemofiltration has to be used with caution because RV unloading can induce low cardiac output.
‘Specific’ pharmacotherapy to decrease RV afterload
Prostanoids and nitric oxide
PH targeted therapy improves pulmonary blood flow and decreases RV afterload. Intravenous prostanoids (epoprostenol, iloprost, treprostinil) should be considered in the critically ill patient, if a severe ventilation-perfusion mismatch has been excluded.3 Since prostanoids lower SVR, concomitant systemic vasopressor therapy may become necessary.
Inhalative therapy with prostanoids or inhaled nitric oxide (iNO) has less impact on SVR and should be considered early, especially if the systemic blood pressure is low. In addition, inhaled or aerosolised application does not worsen the ventilation-perfusion mismatch in the same way as the intravenous route may do.23 INO is the first choice in mechanically ventilated patients. After cardiopulmonary bypass, iNO reduces PVR and may lower the risk of PH crisis and shorten the postoperative course.24 However, in a recent meta-analysis of iNO in patients with CHD, its effect on survival and several haemodynamic secondary end points has been questioned.7 Inhaled iloprost has been proposed as an alternative to iNO with comparable effects on PVR, but well designed prospective clinical trials are lacking.25–28 Acute haemodynamic effects of other inhaled drugs, such as nitroglycerine or milrinone, have been described in small case series,29 but their usefulness is not well established.
PDE5-inhibitors (sildenafil)
Oral sildenafil is reasonable to facilitate weaning from iNO. However, in the intensive care setting oral medications have the disadvantage of unpredictable absorption. Prophylactic use of sildenafil before surgical correction of CHD has been proven to be useful.30 The administration of intravenous sildenafil has been described31 ,32 but its effectiveness has not been clearly determined. Systemic arterial hypotension and impairment of oxygenation have been described as adverse events.33
Pharmacotherapy to increase myocardial perfusion and/or counteract right-to-left interventricular septal shift (LV compression and low LV output)
Inotropes
In the case of severe RV failure in PH, inotropic support may be necessary. Milrinone and levosimendan can be useful as positive inotropic drugs since they have little or no effect on heart rate but lower PVR. Single centre studies have shown positive effects of levosimendan on PVR in children after cardiac surgery.34 Levosimendan's major effect is thought to be improvement of myocardial contractility. Additionally, there is a vasodilator effect due to inhibition of PDE3 activity.34 Dobutamine and epinephrine improve RV contractility but may induce tachycardia which impairs diastolic filling and coronary perfusion subsequently lowering cardiac output.
Vasopressors
Vasopressor therapy with norepinephrine, vasopressin or terlipressin may be indicated to induce reshifting of the interventricular septum from left to right, to improve tissue perfusion in patients with systemic hypotension, and to treat low SVR caused by PH targeted therapy. Elevation of systemic blood pressure may become necessary to maintain coronary perfusion pressure and to reduce leftward septal shift. Vasopressin and terlipressin have been shown in small case series to lower PVR while increasing SVR.35 ,36 Patients on vasopressor therapy should be monitored closely for adequacy of cardiac output.
Non-pharmacological therapy
Surgical or interventional intra-atrial communication
On the basis of clinical experience in adult patients, atrial balloon septostomy should be avoided in patients with acute cardiac decompensation and in end stage RV failure (central venous pressure >20 mm Hg). However, in selected patients, the creation of an intra-atrial communication, decompressing the RA and RV, may be life-saving.
Potts shunt
As an alternative to lung transplantation, creation of an aortopulmonary shunt (Potts shunt) in children with suprasystemic idiopathic PH has been described in a small case series.37 Although these first long-term results are promising, no recommendation can be made because of the limited experience at this stage.
Extracorporeal membrane oxygenation
Depending on RV function venovenous (VV) or venoarterial (VA) extracorporeal membrane oxygenation (ECMO) may be considered as a bridge to recovery or bridge to transplantation.38 In patients with large atrial communications, circulatory support with VV-ECMO may be feasible even in the failing RV by providing oxygenated blood shunting right-to-left through the defect.38 The indication for mechanical support with ECMO depends on aetiology of RV or lung failure. Its short-term use in post cardiac surgery PH is generally accepted. However, longer support times had been described with new therapeutic strategies (e.g. awake-ECMO) making it feasible as bridge to transplantation in selected patients with other aetiologies. Timing of mechanical support in children is less well established compared with adults. The Interagency Registry for Mechanically Assisted Circulatory Support has defined clinical profiles of patients failing on optimal therapy for heart failure. Levels 1 and 2 are generally accepted indications for mechanical support in acute heart failure.39 In children after cardiac surgery, implantation of ECMO with metabolic acidosis or during cardiopulmonary resuscitation (CPR) is a risk factor for increased mortality and brain injury.40
PH crisis after cardiac surgery may cause circulatory collapse requiring CPR. If spontaneous return of circulation cannot be achieved by conventional CPR measures, VA-ECMO implanted during CPR is an option (reversibility of disease).41 Overall survival in VA-ECMO implanted during CPR is 38%, with better outcome in the absence of severe metabolic acidosis before support;40 11% of survivors suffered from cerebral seizures and 6% had evidence of brain injury in a CT scan.40
In patients with idiopathic PH who deteriorate rapidly due to progressive RV failure, eligibility for transplantation has to be evaluated. If lung transplantation is deemed feasible, ECMO should be considered as bridging treatment. Acute decompensation in chronically ill children due to reversible disease (eg, in chronic lung disease and pneumonia) or in patients in whom targeted therapy for PH is suboptimal may require a bridge to recovery strategy.42 Although described in the literature, implantation of ECMO in children with idiopathic PH is controversial due to its irreversible nature and in consideration of the shortage of donor organs. If cannulated peripherally, patients can be awake and extubated,43 which allows longer support times and reduces the risks of ventilator associated complications. In severe RV compromise, VA-ECMO is needed to guarantee adequate cardiac output. Alternatively, a pumpless paracorporeal lung assist that is connected to the pulmonary artery and left atrium after sternotomy may be indicated in patients with hypoxaemia but sustained RV and LV functions.44–46 This device decompresses the RV sufficiently, provides oxygenation and removes carbon dioxide.
With normalisation of cardiac output after lung transplantation the chronically unloaded LV may develop substantially elevated filling pressures leading to pulmonary oedema and lung failure. Successful, scheduled postoperative VA-ECMO as a bridging strategy to LV reverse remodelling and recovery has been described in adults and children.47
Ventricular assist device
Ventricular assist device treatment has not been proven to be effective in children with RV failure due to PH with preserved LV function. Pulsatile devices may lead to pulmonary haemorrhage due to high pulse pressures; while afterload dependent continuous flow devices may not provide sufficient pump flow in patients with high PVR. Therefore ventricular assist device implantation in RV failure due to PH with normal LV filling pressures is not recommended.48
Lung transplantation
Bilateral lung transplantation should be considered in children with inadequate clinical response on maximal combination therapy who remain in functional class III or IV. Due to long waiting times and influence on outcome, transplantation should be considered before cardiopulmonary decompensation has occurred. Mortality of children who are mechanically ventilated before transplantation is significantly increased (HR 2.6, CI 1.72 to 4.07). The median survival rate after lung transplantation in children is between 5.6 years and 6.1 years.49
Therapeutic strategies in different clinical scenarios
CPR of children with acute PH crisis and cardiopulmonary arrest
Resuscitating a patient with severely elevated PVR, acute heart failure and cardiopulmonary arrest is particularly difficult (figures 2 and 3). Resuscitation is initiated and conducted following published guidelines.50 ,51 From a pathophysiological perspective, it is important to proceed with tailored, imminent treatment as mentioned above. Special attention should be given to coronary perfusion (pressure, flow), especially in the setting of severe RV hypertrophy, elevated RV filling pressures and/or tachycardia. RV hypertrophy, decreased aortic to RV end diastolic pressure gradient, and shortening of diastole contribute to RV myocardial ischaemia, RV dilation and subsequent LV compression, causing a rise in LV filling pressures and—together with low cardiac output and coronary perfusion pressure—to additional LV myocardial ischaemia. Studies comparing outcome of standard CPR and CPR plus targeted therapy are lacking. In appropriate patients with acute PH crisis, early implementation of mechanical support (VA-ECMO) should be considered. Clinical data on the neurological outcome of children with pulmonary hypertension, who acutely arrested, are lacking.
{kind=link}
{kind=link}
{kind=link}
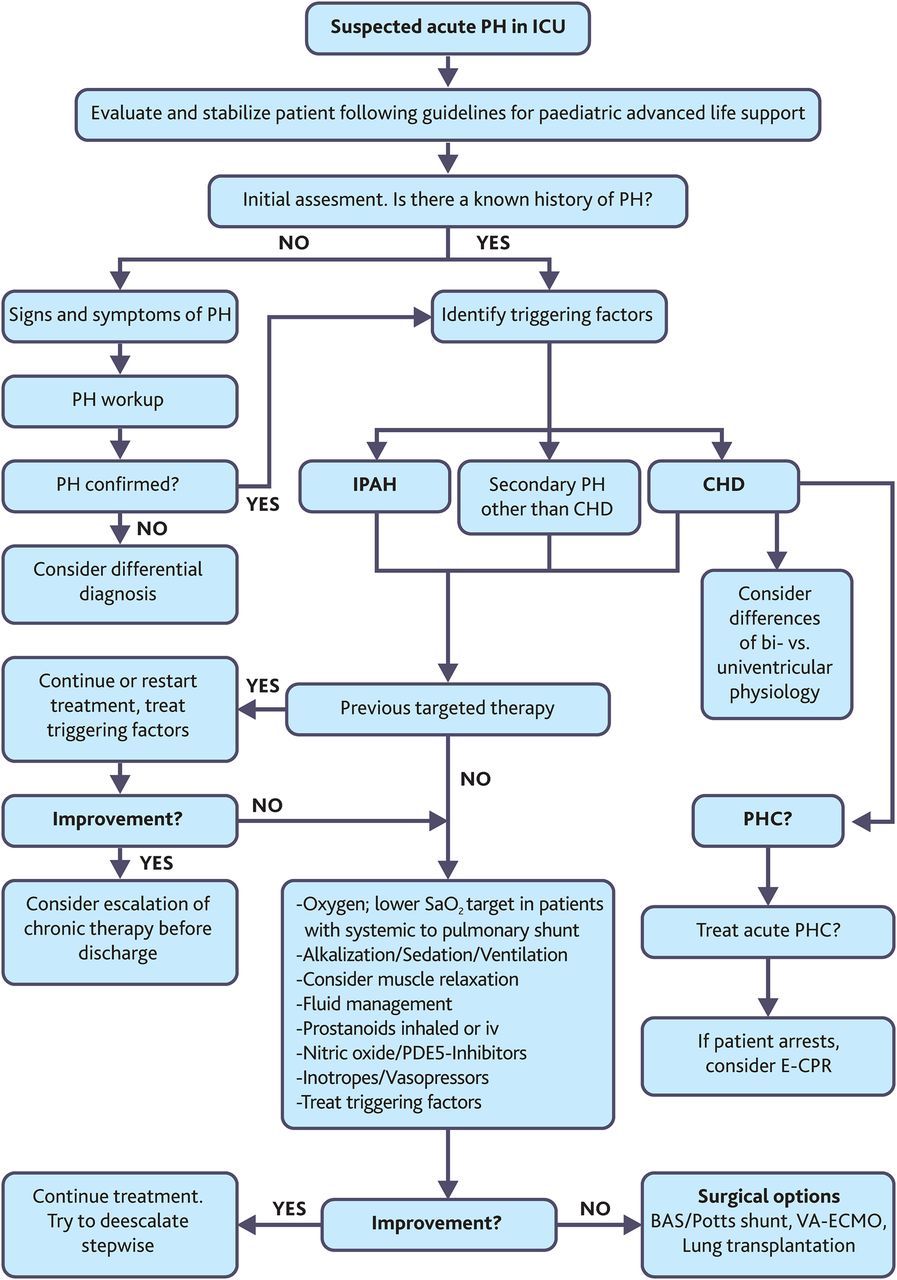
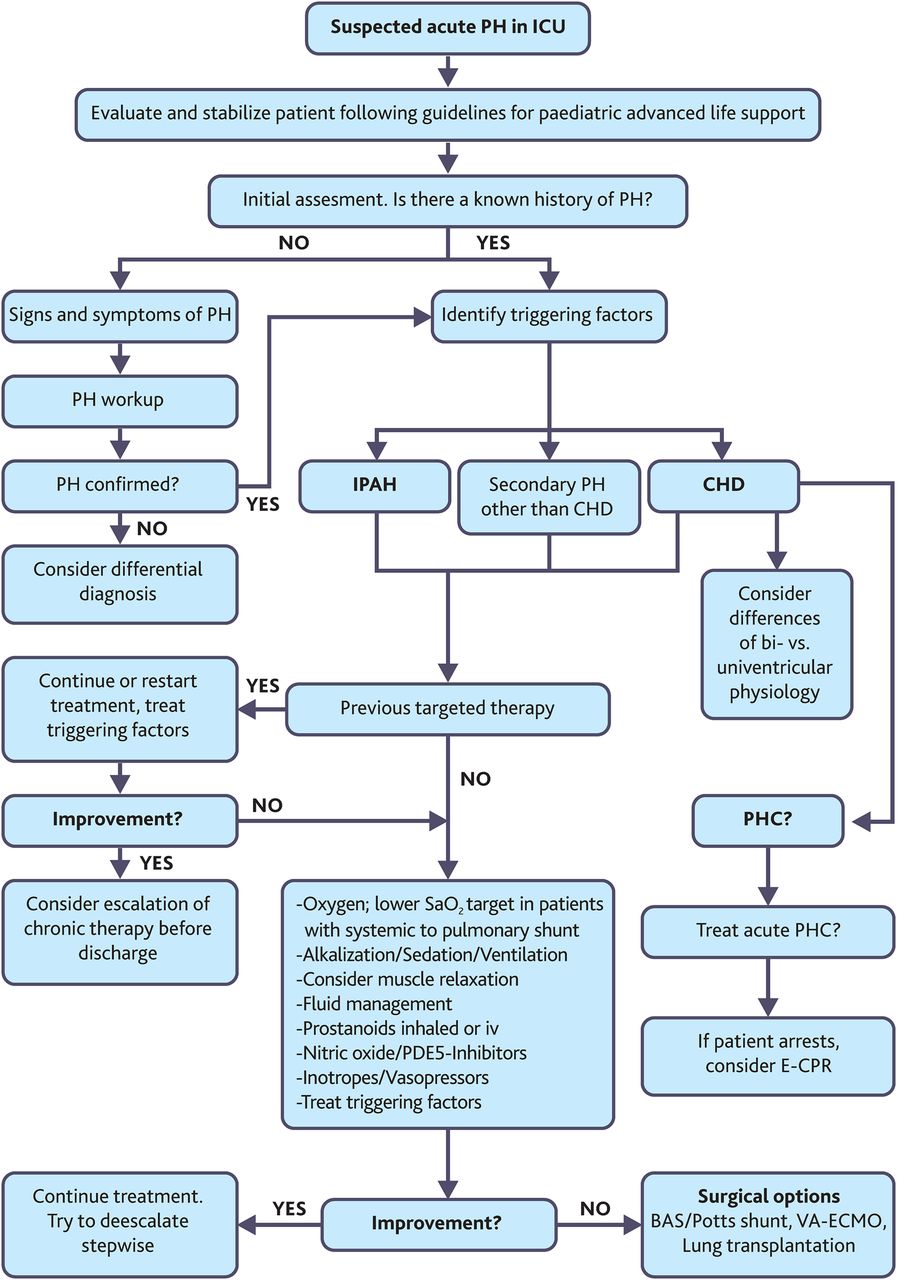
BAS, balloon atrioseptostomy; Clinical algorithm for the management of the scenarios for acute PH in the ICU. CHD, congenital heart disease; E-CPR, extracorporeal membrane oxygenation with cardiopulmonary resuscitation; ICU, intensive care unit; IPAH, idiopathic pulmonary arterial hypertension; PDE5, phosphodiesterase 5; PH, pulmonary hypertension; PHC, pulmonary hypertensive crisis; SaO2, arterial oxygen saturation; VA-ECMO, venoarterial extracorporeal membrane oxygenation; VAD, ventricular assist device.
Therapy of acute postoperative pulmonary hypertensive crisis (PHC)
Acute PHC is a life-threatening emergency and has to be treated aggressively since the risk of cardiocirculatory collapse necessitating cardiopulmonary resuscitation is high. Providing normal ventilation and normalising pCO2 (if necessary with a manual ventilation bag), boluses of norepinephrine, sedative drugs and muscle relaxants restore circulation in the majority of cases. Medication lowering RV afterload, augmenting RV preload and contractility and maintaining adequate coronary perfusion pressure (as described above) preserve LV function and oxygen delivery in patients at risk. Adequate postoperative analgesia and sedation, minimal handling and minimising tracheal suctioning help to prevent acute PHC. Preoperative administration of PDE5 inhibitors such as sildenafil has been tried, but due to the paucity of clinical data, no corresponding recommendation can be made. VA-ECMO should be considered early on when pharmacological and ventilator strategies fail.
Patients with univentricular heart and partial (‘Glenn)’ or total cavopulmonary anastomosis/ ‘Fontan-like’ circulation (ie, no subpulmonary ventricle).
Pulmonary vessels of newborns are highly reactive to stimuli which elevate PVR. In children with univentricular heart after Glenn operation, an increase of PVR may provoke deep cyanosis, stasis of blood in the shunt and shunt thrombosis. Management of suspected shunt thrombosis must be aggressive. No clinical studies comparing different treatment strategies of acute shunt thrombosis are available. Management generally includes: optimisation of ventilation, sedation, muscle relaxation if necessary, iNO, bolus of heparin and prompt treatment of arterial hypotension (bolus of volume if filling pressures are low; norepinephrine to increase afterload, epinephrine if systolic function is impaired). If immediate recovery of arterial oxygen saturations fails to occur, opening of the chest to massage the shunt or implantation of VA-ECMO may become necessary.
In patients with univentricular physiology and total cavopulmonary connection, a low PVR is a prerequisite for adequate ventricular filling and output. iNO,52 milrinone53 and ventilation with low mean airway pressure or better spontaneous breathing54 all contribute to improved outcomes in the early postoperative course. Negative pressure ventilation has been described in the failing Fontan circulation.55 In children who are mechanically ventilated long term, mild permissive hypercapnia may allow lower ventilator settings without elevation of PVR as long as there is no respiratory acidosis (figure 3).
Therapy of PH in a child with acute deterioration of previously known chronic PH
Initial assessment, oxygen supplementation and establishment of monitoring are the first steps in a child with acute deterioration of chronic PH. Decisions on how to treat the child are based on an individualised strategy since scientific evidence is insufficient. As long as the child's condition is not substantially improved (ie, normalisation of lactate, blood gases, vital parameters, urine output) frequent re-evaluations are mandatory. Elevated or increasing lactate levels, development of metabolic or respiratory acidosis, hypotension or other signs of low cardiac output should prompt escalation of therapy including anaesthesia and mechanical ventilation (see Anaesthesia and ventilation) or—if indicated—mechanical support (see Extracorporeal membrane oxygenation). Usually, escalation of specific medical treatment to decrease RV afterload in a child that is not responding to current drugs, means adding a second or third drug rather than exchanging the substances.59 Choice of treatment options is guided by the clinical condition. Initiation of therapy in a spontaneously breathing child with an inhaled drug has the advantage that no venous access is needed and it does not increase ventilation-perfusion mismatch. With respiratory fatigue or in small children, inhalation may become impossible. Intravenous prostanoids should be considered in the critically ill child; blood pressure monitoring is mandatory. If a child is mechanically ventilated iNO may be strongly considered. Clinicians may decide to add sildenafil orally or intravenously, especially in the child who is not responding to therapy; due to the paucity of data, no recommendation can be made in this regard. Inotropic and vasopressor therapy is adapted to haemodynamic parameters. Chronic specific therapy should be continued. If liver function tests are above three times the upper limits, bosentan must be withheld.
Therapy of PH in a child with acute deterioration due to new diagnosis of PH
The principles of treatment are comparable to those described above (see Therapy of PH in a child with acute deterioration due to previously known chronic PH). The clinical condition of a critically ill child initially often precludes a complete diagnostic workup. However, diagnoses and conditions which change the therapeutic regimen such as acute pulmonary embolism must not be missed.
Conclusions
Acute PH is a serious complication in children at risk, including those after surgery for CHD, and has major impact on clinical outcome in patients with and without chronic PH. Treatment in the ICU should be based on the underlying pathophysiology but ultimately needs to focus on the basic goals of lowering RV afterload and augmenting RV preload and contractility. Furthermore, maintaining adequate coronary perfusion pressure and flow will help to preserve myocardial oxygen and energy supply, and thus RV and LV systolic function and oxygen delivery. Early recognition of patients at particular risk, and timely establishment of efficient therapeutic actions may prevent the development of severe cardiac dysfunction, low cardiac output and death.
References
Footnotes
This manuscript is a product of the writing group of the European Paediatric Pulmonary Vascular Disease (PVD) Network (Writing Group Chair: G. Hansmann, Writing Group Co-Chair: C. Apitz). ISHLT, International Society of Heart and Lung Transplantation; DGPK, German Society of Paediatric Cardiology.
Correction notice In table 2 the Sildenafil intravenous dosage has been updated from 0.4mg to 0.4mg/kg since this paper was first published online.
Funding CA currently receives grant funding from Stiftung KinderHerz. GW currently receives grant support from the German Research Foundation (DFG; SFB 738). GH currently receives grant support from the German Research Foundation (DFG; HA 4348/2-1), Fördergemeinschaft deutsche Kinderherzzentren (W-H-001-2014) and Stiftung KinderHerz (2511-6-13).
This Heart supplement was produced with support from an unrestricted educational grant from Actelion Pharmaceuticals Germany GmbH, Bayer Pharma AG, and Pfizer Inc. None of these organisations had any influence on the composition of the writing group or the content of the articles published in this supplement. Open Access publication of this article was sponsored by Actelion Pharmaceuticals Germany GmbH.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.