Article Text

Abstract
Drug-induced valvular heart disease (DIVHD) was first described in the 1960s. Initially, associations with ergot derivatives used for migraine prevention, or with anorectic drugs, were described. Drugs used for the treatment of Parkinson’s disease and endocrine diseases, like hyperprolactinemia, may also induce VHD. More recently, the use of 3,4-methylendioxymetamphetamine (MDMA, ‘Ecstasy’) and benfluorexhave been found to be associated with DIVHD. Although some of these drugs were withdrawn from the market, several cases of patients requiring valve surgery even years after the cessation of therapy have been reported. DIVHD is not infrequent, may be severe, and has been described in association with several drugs. Even after drug cessation, long-term implications of this type of VHD may persist. The present review underlines the need for a careful evaluation of the associated clinical and echocardiographic risk factors to allow early recognition so as not to delay appropriate management.
- Drug-induced valvular disease
- benfluorex
- serotoninergic drugs
- carcinoid syndrome
- valvular disease
- imaging and diagnostics
- echocardiography
- three dimensional
- malignency
- chemotherapy
- transthoracic
- infection
- endocarditis
- metabolic medicine
- diabetic heart disease
- cardiomyopathy
- aortic valve disease
- aortic stenosis
- valvular heart disease
- valve disease
- myocardial disease
- cardiomyopathy restrictive
- diastolic function
- congestive heart failure
- heart failure
Statistics from Altmetric.com
- Drug-induced valvular disease
- benfluorex
- serotoninergic drugs
- carcinoid syndrome
- valvular disease
- imaging and diagnostics
- echocardiography
- three dimensional
- malignency
- chemotherapy
- transthoracic
- infection
- endocarditis
- metabolic medicine
- diabetic heart disease
- cardiomyopathy
- aortic valve disease
- aortic stenosis
- valvular heart disease
- valve disease
- myocardial disease
- cardiomyopathy restrictive
- diastolic function
- congestive heart failure
- heart failure
Introduction
Drug-induced valvular heart disease (DIVHD) was first described in the 1960s. Initially, both the association of DIVHD with either ergot derivatives (ergotamine and methylsergide) used for migraine prevention, or with anorectic drugs, was described.1 Subsequently, drugs used for the treatment of Parkinson's disease and endocrine disease like hyperprolactinemia were also shown to induce VHD2 More recently, the use of 3,4-methylendioxymetamphetamine (MDMA, ‘Ecstasy’) and benfluorex (as adjuvant therapy for dyslipidemia in diabetic patients) have also been found to be associated with DIVHD.3
The issue has received increasing attention as more new associations of DIVHD with several drugs have been reported. Although some of these drugs have subsequently been withdrawn from the market, several cases of patients requiring valve surgery late after the cessation of therapy have been reported, emphasising the long-term implications of DIVHD.4 ,5
Definition
DIVHD is a typical example of an exclusion diagnosis together with a positive history of valvulopathic drug use. Morphologically, DIHVD can be defined echocardiographically as abnormal thickening of valve leaflets, or cusps, resulting in a restrictive motion in the absence of carcinoid syndrome, left ventricular remodelling (ie, ischaemic valve involvement), rheumatic VHD, Libman-Sacks endocarditis and congenital abnormalities. In mitral and tricuspid valve disease, a prominent subvalvular disease with thickening and shortening of the chordae tendinae and leaflet tethering with malcoaptation may also contribute to the regurgitation. For the aortic valve, cusp thickening with doming and regurgitation is typically present without aortic root dilatation.
The evidence for DIVHD
The Fen-Phen anorexigen story has raised the question about the true incidence of fenfluramine-induced valvulopathy in the medical literature. A combination of methodological issues and observer bias led to an overestimation of the occurrence of fenfluramine-induced VHD in some of the reported studies. As echocardiography is the only diagnostic tool available, image quality and correct use of gain settings and filters is very important. Moreover, reporting of echocardiographically detected DIVHD was highest in the USA when funding became available for reimbursement in several damage claims, and has dramatically decreased after the suppression of this financial drive. This emphasises that blinding during echocardiographic acquisition and interpretation is paramount. Also, for many study patients, an echocardiogram prior to drug exposure was not available, and consequently, pre-existent VHD could not be ruled out. Furthermore, the prevalence of valvular regurgitations in obese patients not exposed to these drugs is not well known.
Although discussion persists about the exact incidence of drug-induced VHD, all the available clinical data, as well as in vitro and prospective small animal studies reproducing DIVHD, support its actual existence.6 ,7
Clinical prevalence and significance of DIVHD
The prevalence of DIVHD depends on the type of drug, the dose and duration of therapy, the valve affected by the process, the severity of pre-existing VHD, concomitant treatment with other drugs, and the potential reversibility of the disease. From a methodological perspective, the type and severity of the valve lesion that is sought has a direct implication on the sensitivity and specificity of disease detection. Moreover, the objective definition of the epidemiology of DIVHD is dependent on a number of factors: the performance and/or interpretation of the echocardiogram in a non-blinded fashion, and other potential co-determinants, including pre-existent VHD, age, obesity, diabetes and hypertension. Most studies that have reported on DIVHD have been retrospective and have frequently lacked a control group. In such settings, referral bias (ie, the presence of significant symptoms) will also be important (table 1).
Drugs associated with valvular heart disease
Methysergide and ergotamine
Based upon sporadic case-reporting of symptomatic patients, the estimated prevalence of DIVHD would appear to be low after methysergide and ergotamine exposure, but neither a case-control study for ergotamine or methysergide-induced VHD, nor a dose-dependent relation has been described so far.8
Fenfluramine
Regarding the association of anorexigens with VHD, 18 million prescriptions had been written in the USA for either fenfluramine or phentermine until the FDA asked the manufacturers to withdraw (dex)fenfluramine from the market in 1997. Although the initial description of DIVHD with these drugs did not include epidemiologic data, several retrospective case-control and follow-up studies confirmed the relation between (dex)fenfluramine exposure and VHD.9 ,10 Later, it became clear from a meta-analysis that anorexigen-induced VHD was less frequent than initially described, but was present in one out of eight patients treated for more than 90 days.11 In another meta-analysis, Hopkins et al found a high RR for aortic (RR 19,6) and mitral (RR 5,9) valve disease after (dex)fenfluramine use after they had corrected for several bias factors.12 The same group performed the largest observational study in 5743 ex-fenfluramine users and showed the prevalence of aortic regurgitation (AR) and/or mitral regurgitation (MR) to be 19.6% in women and 11.8% in men.4 After valve surgery in a subset of 25 patients, there was clear histological evidence of fenfluramine-induced VHD. Phentermine alone has never been associated with DIVHD.
Pergolide and cabergoline
Patients treated with ergot-derived dopamine agonists' pergolide or cabergoline for Parkinson's disease have been shown to have a significant risk of VHD, with a similar spectrum and incidence of valve lesions, as seen after fenfluramine exposure.13 This risk is increased relative to the cumulative dose received. In a recent review, Antonini et al reported moderate to severe regurgitation of at least one heart valve in 22% and 34% of patients with Parkinson's disease exposed to pergolide and cabergoline, respectively.14 Corvol et al reported a similar prevalence in their meta-analysis: moderate to severe VHD was found in 22% of pergolide users compared with 7% in controls.15 In another meta-analysis, moderate to severe VHD was found in 26% out of 477 patients treated with pergolide or cabergoline compared with 10% in the control group.16 Pergolide has been withdrawn from the market in the USA, and more recently in some (but not all) European countries.
Low-dose cabergoline, prescribed for hyperprolactinemia, has rarely been associated with DIVHD.17 Of the seven cross-sectional studies that have been published so far, six did not find a clinically relevant prevalence of regurgitation.18 Gu et al showed that also for these patients, blinding to the treatment identity is of the uppermost importance in order to avoid over-reporting of DIVHD.22
Bromocriptine
Only one case report and one case-control study have suggested an increased risk for DIVHD with bromocriptine use, while a recent meta-analyis including other negative case-control studies could not confirm this association.19 Thus, further studies with bromocriptine are needed to completely rule out a toxic valvular effect.
MDMA (‘Ecstasy’)
In one small observational study, mild valve regurgitation was found in 28% of subjects younger than 30 years of age taking MDMA on a regular and recreational basis as compared with 0% for age- and sex-matched controls. As MDMA is not only a frequently used illicit party drug but is also used in several studies for the treatment of post-traumatic stress disorders, it is essential to clarify further if there is any relationship between MDMA and DIVHD.3
Benfluorex
In 2009, benfluorex was withdrawn from the French drug market because of its association with DIVHD. Meanwhile, some 300 000 French patients have been exposed to the therapy (which had been approved for the treatment of overweight in diabetic patients with dyslipidemia). Published data suggest an adjusted RR of 3.1 (2.4–4) for all valvular regurgitations with a predominance of aortic valve involvement: 4.4 (3–6.6).20 Furthermore, a dose relationship has been demonstrated. In a recent single-centre study, a retrospective analysis of patients with unexplained restrictive VHD showed an exposure to benfluorex in 72% of the cases. About 60% of them were treated in combination with other anorectic drugs.21
Mechanisms of DIVHD: role of the serotonin 2B receptor
There are obvious histopathological similarities between DIVHD and carcinoid heart disease, which occurs in 10% of patients with carcinoid tumours. In the latter, elevated blood levels of serotonin (5-HT) may lead to right-sided VHD. The presence of left-sided VHD is less frequent as 5-HT is degraded by the monoamine oxidase enzymes in the lungs. In contrast, DIVHD most frequently affects the aortic and the mitral valves.
Fibrotic valvular lesions similar to those seen in carcinoid heart disease have been observed with the use of ergot alkaloids ergotamine and methysergide. After the Fen-Phen anorexigen story, two groups independently demonstrated that the serotonin 2B (5-HT2B) receptor acts as culprit receptor.23–25
Stimulation of this receptor leads to the upregulation of target genes involved in the proliferation and stimulation of valvular interstitial cells through different intracellular pathways. These involve G-protein-mediated activation of protein kinase C, Src-protein and extracellular-regulated kinases 1 and 2 (ERK 1/2). Transforming growth factor-β (TGF-β) receptor activation is also involved in this process (figure 1).26

Schematic representation of the anatomic and pathophysiologic mechanisms involved in drug-induced valvulopathy. Valvulopathic drugs lead to 5HT2B receptor activation. Protein kinase C activation results from dissociation of guanine nucleotide regulatory proteins (G-proteins) and activated phospholipase C-β (PLC-β) via diacylglycerol (DAG) release. G-proteins may also cause activation of extracellular-regulated kinases 1 and 2 (ERK1/2) through β-arrestin (βarr) binding. 5-HT and Src protein may also activate the TGF-β receptors. Both 5-HT2B and TGF-β pathways ultimately lead to upregulation of specific target genes responsible for valvular interstitial cell proliferation and glycosaminoglycan production.
Although both fenfluramine and phentermine lack 5-HT2B agonistic properties, the primary metabolite of fenfluramine, norfenfluramine, is a potent 5-HT2B agonist; Norfenfluramine is also a known metabolite of benfluorex. Such a 5-HT2B agonist effect was also found for pergolide, cabergoline, MDMA, ergotamine and methylergonovine, a metabolite of methysergide. By consequence, the ‘net’ valvulopathic effect is dependent on the 5-HT2B activity of the parent drug, and also on the pharmacodynamic effects of their metabolites. This makes it more difficult to predict the toxic valvular effects of any new drugs that are developed. Other frequently prescribed anti-Parkinson drugs (apomorphine, pramipexole, lisuride, terguride and ropinirole) do not share the 5-HT2B agonist effect, and have not been associated with VHD, further confirming the central role of 5-HT2B in DIVHD. Bromocriptine has a weak partial 5-HT2B agonist effect and is, therefore—theoretically—less likely to be associated with DIVHD. Moreover, in a recent study, we found that cyproheptadine, a potent 5-HT2B antagonist, could prevent pergolide-induced VHD in Wistar rats.27 This study showed that 5-HT2B receptor antagonists might have prophylactic and/or therapeutic potential.
Morphological characteristics
Histopathology
Overstimulation of the valvular 5-HT2B receptor leads to fibroblast activation with the production of collagen and glycosaminoglycans. In this manner, thickening of the valvular surface and subvalvular apparatus occurs by formation of fibromyxoid plaques. Calcifications is not usually part of this process. Macroscopically, the valves and tendinous chords are both thickened and shortened, and may have a shiny white appearance (figures 1 and 2).1 ,2

Echocardiographic and histopathological characteristics in a case of severe pergolide-induced aortic (A) and mitral (B) valvulopathy requiring double valve replacement. Thickened, restrictive valve with doming (A1) and tenting (B2) when maximally closed. Associated severe aortic (A2) and mitral (B2) regurgitation. Histopathology shows a clearly thickened aortic (A3) and mitral (B3) cusp/leaflet due to myxoid fibrotic plaques on the external surface with preserved valve architecture. No signs of calcification, inflammation or neovascularisation are present.
Echocardiography
Echocardiography, with is high spatial and temporal resolution, is the standard approach used in the diagnosis of DIVHD. In mitral disease, both the leaflets and the subvalvular apparatus may be affected. The leaflets are thickened, show reduced mobility, and are more retracted towards the apex during systole (leaflet tenting) resulting in valve regurgitation. An affected aortic valve is characterised by systolic doming of the thickened leaflets with reduced mobility and incomplete diastolic coaptation. This causes regurgitation.2 In patients exposed to MDMA, a higher prevalence of valvular strands have also been noted.3
In younger patients under the age of 50 years with a low background prevalence of AR and MR, such abnormalities can be more easily identified. The presence of trivial to moderate AR, or moderate to severe MR, was the criterion proposed by the FDA to confirm DIVHD in the late nineties.28 Conversely, in older patients with Parkinson's disease, pre-existing valvular sclerosis and calcifications are relatively common and are often associated with some degree of AR or MR. Consequently, a scoring system was used.2 In this scoring, restrictive tricuspid valve leaflet involvement was considered more important in defining ergot-like abnormalities compared with restrictive mitral and aortic valve motion (Score 1–4: from very likely to unlikely).
-
Proven restrictive VHD (confirmed with histopathology and/or regression after interruption of ergot treatment);
-
Important restrictive valve disease (regurgitation >2/4) or restrictive tricuspid disease, even with regurgitation less than 2/4;
-
Mild to moderate (regurgitation <2/4) restrictive valve disease;
-
No restrictive valve dysfunction.
Another potential approach to quantify the restrictive tricuspid and/or mitral valve motion is to determine the tenting area and tethering distance as described in ischaemic heart disease.29
Differential diagnosis
As mentioned above, other causes of restrictive valve motion need to be ruled out when diagnosing DIVHD: left ventricle remodelling (ie, ischaemic MR), rheumatic VHD, carcinoid VHD, and Libman-Sacks (antiphospholipid syndrome) endocarditis and congenital abnormalities. Absence of commissural fusion and calcifications are helpful in differentiating with rheumatic disease when concomitant valve obstruction is absent (table 2).
Differential diagnosis of drug-induced valvular heart disease (DIVHD): key features of distinct causes of valvular heart disease that might resemble DIVHD
Clinical implications
Screening of new medications potentially causing VHD
In view of the important socioeconomic consequences of Fen-Phen, and the recent withdrawal of benfluorex, vigilance for DIVHD still remains at a position of uppermost importance. As well as the known drugs causing VHD, several other drugs have been tested for 5-HT2B agonist activities. In a recent report by Huang et al, five new potent agonists out of a database of 2200 drugs were identified: guanfacine, oxymetazoline, quinidine, xylometazoline and fenoldapam. The authors especially draw attention to quanfacine (antihypertensive) and quinidine (antiarrhythmic and Malaria prophylaxis/treatment) as potentially causing VHD, as they may be prescribed for sustained periods.31 The other drugs are typically prescribed for shorter periods and might be of lesser concern. As mentioned above, the 5-HT2B agonist activity of the parent drug, and also its metabolites need to be considered. As a result, DIVHD might be more difficult to predict on the basis of in vitro essays only. Animal models of DIVHD might therefore be of additional value for the preclinical screening for toxic valvulopathy.6
Evolution of DIVHD: influence of treatment duration, dose and reversibility
From several retrospective case-control trials and meta-analyses, it is clear that there is a correlation between drug dosage, duration and the severity of valvular abnormalities. Clinical follow-up data are available for fenfluramine, pergolide and cabergoline only. The principle of dose-dependency and reversibility has also been described prospectively for serotonin in rats.32
In the largest observational study of 5743 patients, the duration of fenfluramine use was strongly predictive of AR, MR and tricuspid regurgitation.4 In the meta-analysis by Corvol et al, the severity of VHD correlated with the cumulative dose of pergolide.15 Also, a positive correlation with treatment duration and cumulative dose has been found for cabergoline.13 ,33 Besides daily drug dose and duration of exposure, other attenuating factors may be involved in the development of drug-induced VHD. One case report describes the presence of severe VHD even with the use of low-dose pergolide.34 Moreover, two-thirds of patients will not develop VHD, despite several years' exposure, suggesting that receptors' susceptibility is a key factor. Thus, some patients may be at a higher risk when exposed to valvulopathic drugs. In a study with more than 400 patients exposed to fenfluramine, older age and higher diastolic blood pressure were independently related to aortic valvulopathy, as defined according to the FDA criteria.35
Several echocardiographic follow-up studies have shown that some regression of DIVHD may occur after withdrawal of fenfluramine. For the other drugs, less follow-up data are available. In the study by Dahl et al, follow-up data was obtained in 1020 fenfluramine patients.4 After a mean follow-up duration of 30 months, the severity of valve regurgitation remained mostly unchanged, while 25% improved and 17% deteriorated. This is the only study to report disease progression after drug withdrawal in some patients, while this was rare in the other follow-up studies. Fortunately, functional valvular improvement was observed in up to one-third of patients even after 6 months. It remains unclear from these studies whether more damaged valves are less likely to show disease regression.
Practical recommendations
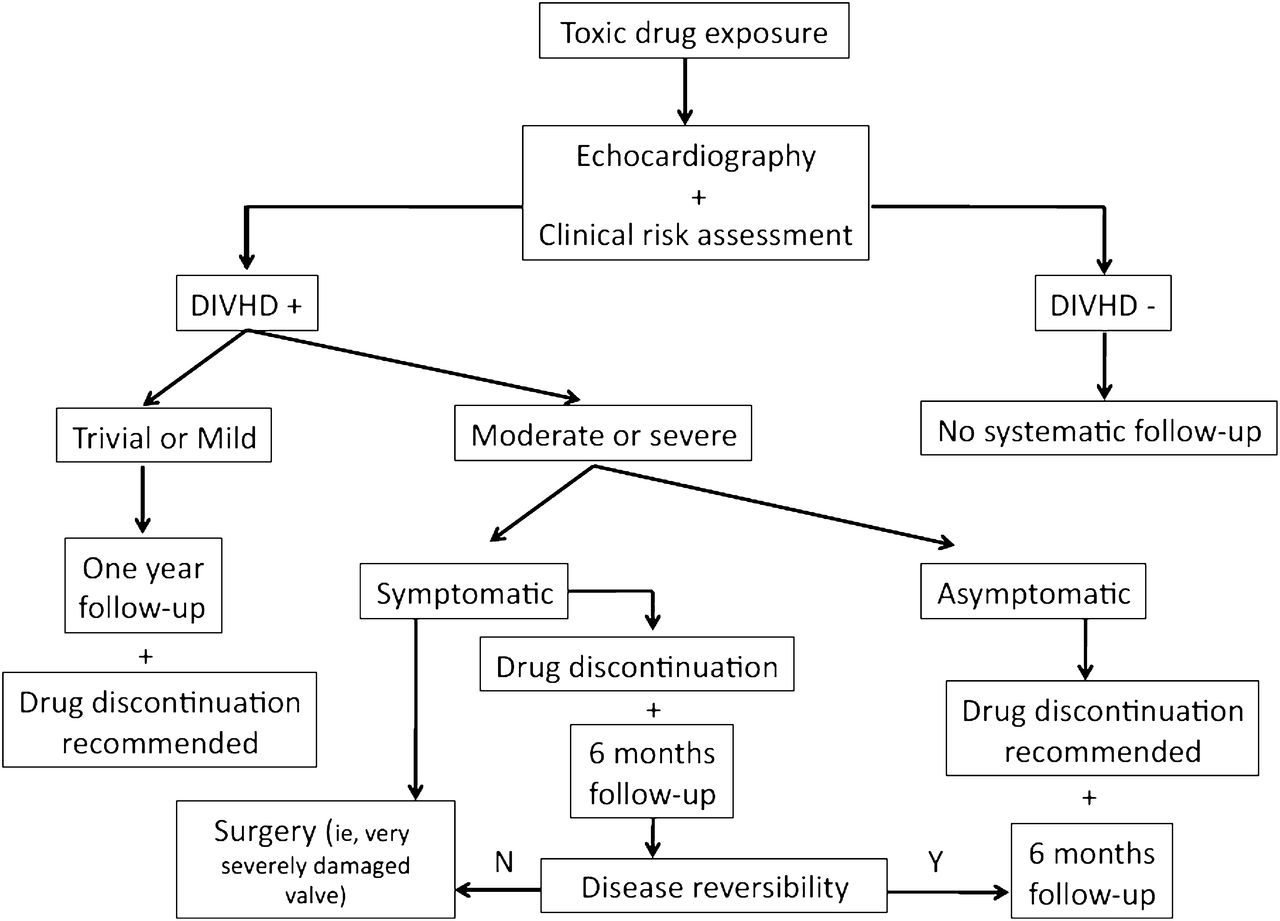
1. DIVHD must be considered when there are otherwise unexplained typical echocardiographic features of thickened heart valves with reduced mobility and restrictive motion in the absence of commissural fusion, with also no evidence of valve calcification or left ventricular dysfunction. The likelihood of DIVHD increases if more than one heart valve is affected and the patient is young. The history of exposure to drugs potentially causing valve disease is fundamental to the diagnosis (figure 3).
{kind=link}
{kind=link}
{kind=link}
Algorithm for the management of drug-induced valve heart disease.
2. In patients exposed to drugs potentially causing valve disease, the first step should combine the assessment of symptoms, clinical risk (including the duration and dose of exposure, and the time from discontinuation), as well as an assessment of concomitant drug ingestion and associated risk factors. Second a complete and comprehensive echocardiographic exam should be performed. In the absence of DIVHD, no systematic follow-up is required. In the presence of abnormalities, in patients with trivial or mild regurgitation, a yearly follow-up is recommended. In asymptomatic patients with moderate to severe regurgitation, a control exam every 6 months is advisable.
3. In symptomatic patients with moderate to severe VHD, surgery is the first-line option. However, in selected patients, a watchful waiting strategy should be considered, since reversibility of one grade of regurgitation severity may occur in 50% of patients within 6 months.
Conclusions
DIVHD is not infrequent, may be severe, and has been described in association with several drugs. Even after drug cessation, long-term sequelae of this type of VHD may persist. A careful evaluation of the associated clinical and echocardiographic risk factors is mandatory. Since the phenotypic expression of the disease is specific, it should be recognised early so as not to delay appropriate management.
Acknowledgments
The authors are indebted to Professor George R Sutherland for his critical review and helpful editorial assistance in revising this manuscript.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.