Article Text

Abstract
Objective To assess the results of early homograft aortic root replacement in infants and children with an aortic root abscess.
Design Descriptive study of all patients with an aortic root abscess during 1987–97, identified by retrospective review of the echocardiographic and surgical registries.
Setting A tertiary referral centre.
Patients Five patients (age 0.6 to 13 years; two female) were identified with an aortic root abscess. Four had no known pre-existing congenital heart abnormality. Three had a misleading presentation and were referred to our hospital with non-cardiac diagnoses (fulminant hepatic failure; adult respiratory distress syndrome; cerebrovascular accident). The other two presented with septicaemia and a murmur, respectively. Blood cultures identified Staphylococcus aureus(n = 3) and Streptococcus pneumoniae(n = 2). Aortic root abscess was diagnosed by transthoracic echocardiography.
Interventions Homograft aortic root replacement with coronary reimplantation was performed urgently (median one day after diagnosis).
Results Four patients survived. The youngest died following multiorgan failure, multiple aortic fistulae, three valve involvement, and extensive tissue destruction preventing mitral valve replacement (S pneumoniae). Two of the four survivors have required further surgery: mitral valve replacement (0.3 years later), and pulmonary autograft replacement of the homograft (8.3 years later). All survivors remain in sinus rhythm and New York Heart Association functional class I.
Conclusions Infective endocarditis should be considered in any child with severe septicaemia or embolic phenomena. Echocardiographic diagnosis of an aortic root abscess indicates uncontrolled infection and impending haemodynamic collapse. Homograft aortic root replacement can be performed successfully in critically ill children with active infection.
- aortic root abscess
- homograft
- aortic root replacement
- endocarditis
Statistics from Altmetric.com
Aortic root abscess formation is a severe complication of aortic valve endocarditis. In our experience, the detection of aortic root abscess by echocardiography indicates uncontrolled infection and incipient or established haemodynamic compromise. We adopted a policy of urgent surgical intervention when this diagnosis was made, and we present what we believe to be the largest paediatric series describing this rare but potentially lethal problem.
Methods
PATIENTS
We identified five patients with aortic root abscess from the surgical and echocardiography registry between 1987 and 1997 (table 1), and reviewed their records retrospectively. All underwent urgent homograft aortic root replacement. Only patient 5 (bicuspid aortic valve and mild aortic stenosis) was previously known to have congenital heart disease. The remaining four patients had apparently normal hearts before their acute illness, and three were referred to our hospital with non-cardiac diagnoses: patient 1 with septicaemia and fulminant hepatic failure (liver biopsy was performed to exclude Reye’s syndrome); patient 3 with septicaemia and adult respiratory distress syndrome; and patient 4 with a depressed conscious level and right hemiplegia.
Characteristics of the patients
Echocardiography showed that patient 3 had a bicuspid aortic valve, but none of the other three patients had evidence of previous structural heart disease.
The source of septicaemia was not apparent in any of the patients. Blood cultures grew Staphylococcus aureus(n = 3) and Streptococcus pneumoniae(n = 2), but valve and aortic root tissues obtained at surgery were all sterile on culture. All patients were treated with at least two synergistic antibiotics based on bacterial sensitivities and measurement of minimal bactericidal concentrations, and all survivors received intravenous antibiotics for six weeks in total and at least four weeks postoperatively. At the time of surgery, all patients had active endocarditis with uncontrolled infection. Two patients (1 and 3) were ventilated, and three (1, 2, and 3) were receiving intravenous inotropic support at the time of diagnosis of aortic root abscess and subsequent surgery.
ECHOCARDIOGRAPHY
Diagnosis of aortic root abscess was by transthoracic echocardiography at a median of 10 days after hospital admission (combined time at referring hospital and our institution, range 4 to 15 days). Echocardiographic diagnosis required unequivocal localised increased echodensity in the tissue surrounding the aortic root, seen in at least two imaging planes (fig 1), or demonstration of an echo-free space adjacent to the aortic root (fig 2). In four patients there was no evidence of endocarditis or aortic root abscess on the first echocardiogram. Median time to surgery after diagnosis of aortic root abscess was one day (range 0–5 days). Surgery was delayed in patient 4 because of concern about exposing her to cardiopulmonary bypass soon (15 days) after a severe cerebrovascular accident. However, five days after the diagnosis of aortic root abscess, apparently acute aortic regurgitation developed and surgery was performed. She was the first patient in this series, and was investigated preoperatively without the availability of colour Doppler flow mapping. All the remaining patients also had aortic regurgitation before surgery and one had multiple fistulae from the aortic root (fig 3). No patient underwent cardiac catheterisation.
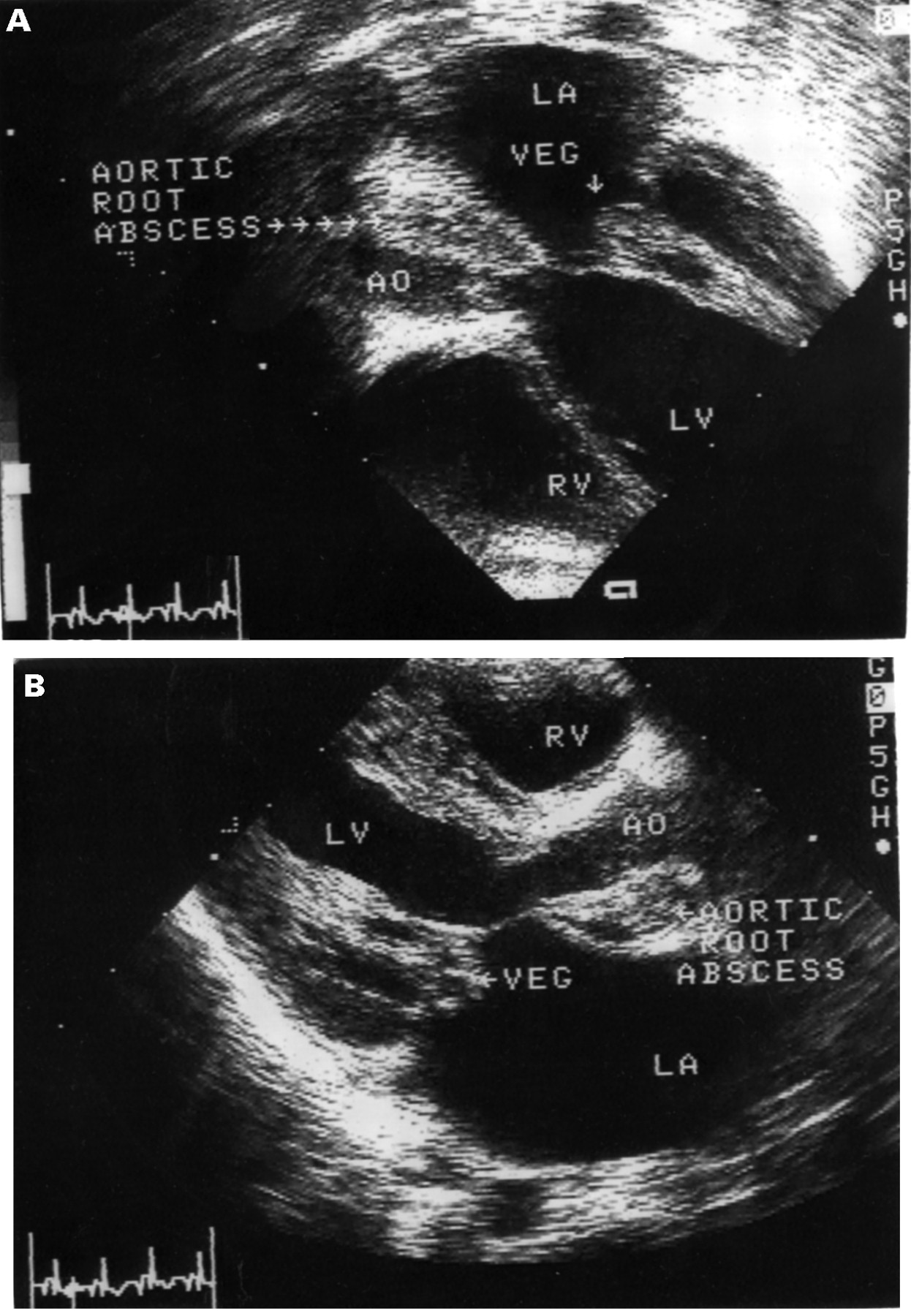
Aortic root abscess seen as an increased echo density in the apical four chamber (A) and parasternal long axis planes (B). An anterior mitral valve leaflet vegetation is also present (patient 3).

Aortic root abscess seen as zones of echo lucency (arrowed) around the aortic root in the parasternal long axis and short axis planes (patient 4).

{kind=link}
{kind=link}
{kind=link}
Fistulae from the aorta to left atrium and right ventricle (patient 1).
SURGERY
Surgical procedures are summarised in table 1. The operations were performed under hypothermic cardiopulmonary bypass with crystalloid cold cardioplegia infused directly into the coronary ostia. The aorta was transected above the commissures and the whole aortic root was excised, together with removal of all necrotic and purulent material. This was found to be impossible in patient 1, where there was complete destruction of the fibrous body and multiple fistulae to the right and left atria. Cryopreserved aortic homografts were used for root replacement in all patients. The aortic homograft was implanted in the anatomical position in patient 1, but in all subsequent patients the homograft was rotated, allowing the fibrous margin to be secured to the muscular portion of the left ventricular outflow tract. The homograft was anchored below the necrotic area resulting in the abscess being exteriorised. The coronary arteries were transferred to the homograft with a large cuff of sinus wall and the repair completed by formation of the distal anastomosis with the aorta.
Results
The youngest patient died (patient 1). He was moribund at the time of surgery, with multiorgan failure. Echocardiography had shown multiple fistulae from the aortic root to the right and left atria and right ventricle (fig 3). These were confirmed at surgery, together with destruction of the central fibrous body and mitral annulus. He died at operation because there was no tissue to support a mitral valve prosthesis.
Two patients have required reoperation. Mitral valve repair was performed in patient 4 in addition to aortic root replacement at the original operation, but four months later he developed severe mitral regurgitation without evidence of recurrent endocarditis, and required mitral valve replacement (21 mm St Jude prosthesis). Patient 4 outgrew her homograft, and 8.3 years later underwent pulmonary autograft replacement of the aortic homograft. She still has a partial right hemiparesis, but has normal cognitive development and good exercise tolerance. All surviving patients are in sinus rhythm and New York Heart Association class I at follow up of 1.5 to 9 years.
Discussion
The diagnosis of infective endocarditis may be difficult, as may be decisions regarding the nature and timing of surgical intervention. Endocarditis should be considered in all children with severe septicaemia or embolic phenomena. An important feature of this series was the misleading presentation of three of the five patients, reflected in their initial referral to our hospital, but not to the cardiothoracic Unit, with non-cardiac diagnoses.
Death from unrecognised endocarditis may be more common than realised. In a recent paediatric series from North America, seven of 13 deaths were in patients with infective endocarditis which was not diagnosed before death.1 Six of these seven patients had not had echocardiography. Aortic root abscess was not diagnosed in any patient without previous cardiac surgery in a study of 42 infants and children with infective endocarditis seen in our Unit in the pre-echocardiography era, 1965–83.2
In the present series, the diagnosis was made using transthoracic echocardiography. However, there was no evidence of aortic root abscess, nor of aortic valve vegetations or valve dysfunction, on the first echocardiogram in four of the five patients. This shows that serial echocardiography may be required to establish the diagnosis. It is possible that transoesophageal echocardiography might have led to an earlier diagnosis. However, all but one of our patients was aged 3 years or less, and excellent transthoracic echocardiographic images were available. Transoesophageal echocardiography was available only in the last patient in the series and was not required for diagnosis or preoperative assessment. However, transoesophageal echocardiography may be the optimal diagnostic technique in older children and adults, and the recent availability of small probes has made the technique increasingly attractive in infants when transthoracic echocardiographic images are suboptimal, especially to demonstrate the subtle early appearances of aortic root abscess.
The evolution of the echocardiographic appearance of aortic root abscess involves a localised increase in echodensity in the tissue surrounding the aortic root (fig 1) before cavity formation with echolucency occurs in the perivalvar tissue (fig 2).3 ,4The evolution from an apparently normal aortic root appearance to cavity formation occurred within two days in two of our patients (3 and 4).
The timing and nature of surgery for aortic root abscess is controversial. From experience in the pre-echocardiographic era, some have considered that immediate surgical intervention is not required, because in most patients the abscess cavity will diminish in size and eventually resolve with antibiotic treatment alone.5However, experience in children has been especially limited. In a large series of 98 infants and children with infective endocarditis seen over a 13 year period, 30 underwent acute surgery, only two of whom had an aortic root abscess.6 One of these underwent debridement and aortic valve repair but required subsequent aortic root replacement, whereas the other had aortic root replacement followed by aortic valve replacement and then repeat aortic root replacement after a false aneurysm developed. The authors suggested that it is vastly preferable to complete antibiotic treatment before surgery if satisfactory control of systemic sepsis and haemodynamic status can be maintained. Our experience suggests that this is rarely possible in the presence of genuine aortic root abscess—all of our patients had aortic regurgitation with haemodynamic compromise and evidence of uncontrolled infection at the time of surgery. The rate of haemodynamic deterioration which we observed was especially alarming. There has been no known case of false positive or false negative diagnosis of aortic root abscess in our unit during this study, and no patient with aortic root abscess has been treated without surgery. Medical treatment of aortic root abscess may be theoretically attractive, but successful non-surgical management was considered sufficiently rare as recently as 1993 to justify a case report of an elderly woman who declined further surgery for prosthetic valve endocarditis and aortic root abscess.7
The development of aortic root abscess was considered a rare complication of aortic valve endocarditis in the pre-echocardiography era, but demonstration of aortic root abscess in 24 of 59 adults (41%) with fatal aortic valve endocarditis8 suggests that it was considerably underdiagnosed. In that necropsy study, risk factors for aortic root abscess were recent onset aortic regurgitation, development of atrioventricular block or pericarditis, and, importantly, a short duration of symptoms before major disability or death. This latter risk factor suggests the need for urgent surgical intervention, which remains our preference. If initial medical management is chosen, rigorous echocardiographic assessment on at least a daily basis is advisable, with recourse to urgent surgery in the presence of expanding tissue involvement, increasing severity of aortic regurgitation, or other signs of uncontrolled infection.
In this series, the median time to surgery after detection of aortic root abscess was one day. Surgery was deferred in the patient with recent cerebrovascular accident because of concern about the risk of cerebral haemorrhage during cardiopulmonary bypass in a child with extensive left temporo-parietal cerebral infarction on computed tomography. This may have been excessively cautious. In adult patients with left heart endocarditis, the only risk factor that correlated with perioperative stroke was haemorrhagic infarction on preoperative scans, whereas the timing of valve replacement, ischaemic cerebral infarction, and the size and number of cerebral infarcts were not risk factors.9
The only death occurred in the youngest patient with multiorgan failure, who was moribund by the time endocarditis and aortic root abscess with multiple fistulae and extensive tissue destruction was detected on his first echocardiogram, and this delay in diagnosis precluded successful surgery. Another patient required mitral valve replacement four months after the first operation because of failure of his mitral valve repair, although there was no evidence of persistent infection. Mitral valve repair in active endocarditis can be successful and should be attempted unless there is destruction of the subvalvar apparatus.10 All four survivors in the study remain in sinus rhythm, and avoidance of heart block may be a benefit of early intervention.
Homograft aortic valve or root replacement has been performed successfully in adult patients with active native aortic valve endocarditis complicated by aortic root abscess.11 The use of alternative prostheses may be determined by non-availability of homograft tissue.12 However, the use of mechanical bioprostheses does not preclude a good surgical result. Of 110 mainly young adult patients undergoing early surgery for aortic valve endocarditis complicated by heart failure, 35% of whom had aortic root abscess, in-hospital mortality was only 5%.13 In another series of 21 adults with native or prosthetic aortic valve endocarditis complicated by aortic root abscess, diagnosed preoperatively by echocardiography in seven, successful acute surgical repair was achieved in 20 (95%) by debridement of infected tissue and reconstruction of the left ventricular outflow tract with autologous pericardium, together with mechanical or porcine aortic valve replacement.14
The other alternative to homograft aortic root replacement for aortic root abscess is pulmonary autograft aortic root replacement (Ross operation). The patients in this series presented in an era before the widespread use of pulmonary autograft aortic root placement in children. In favour of the Ross operation, it could be argued that autologous tissue implanted to the aortic root in the presence of active infection might be less susceptible to progressive sepsis. However, infection of the homograft tissue was not a problem in this series of patients. Our preference for homograft aortic root replacement was also dictated by the fact that the Ross operation is a long and technically demanding procedure, and that expeditious surgery was required in the presence of active infection. Small children will outgrow homograft aortic root replacement. Consequently, our preference to date has been to reserve pulmonary autograft aortic root replacement for subsequent replacement of the homograft aortic root in patients presenting with aortic root abscess. However, increasing surgical experience with the Ross operation in children and accumulating evidence of good long term outcome following this procedure could mean that this will become the procedure of choice in the future, as has been advocated in adults,15 but we believe that it would be premature to make this conclusion at present.
CONCLUSION
Endocarditis can have various clinical presentations, and should be considered in any child with severe septicaemia or embolic phenomena. Echocardiographic detection of aortic root abscess is an indicator of uncontrolled infection and incipient or established haemodynamic compromise. It should be regarded as an indication for urgent aortic root replacement, which can be performed successfully in the presence of active infection. Small children will outgrow a homograft aortic root replacement. It may be preferable to perform pulmonary autograft aortic root replacement at that time, rather than as a primary procedure during acute infection.