Article Text

Abstract
Background: It has been suggested that patients undergoing acute intervention for coronary syndromes may not receive adequate secondary prevention.
Objective: To analyse the impact of availability and use of coronary interventions on the prescription of secondary prevention after acute coronary syndromes.
Design: Analysis of a prospective multicentre register of patients admitted to hospital for acute coronary syndromes.
Setting: A 1999 pan-European survey in 390 hospitals.
Patients: 3092 patients admitted to hospital with acute coronary syndromes (including 777 for ST elevation myocardial infarction within 12 hours of onset).
Main outcome measures: Rates of prescription of aspirin and lipid lowering agents.
Results: Performance of coronary angiography and percutaneous coronary interventions (PCI) during the hospital stay were independent predictors of prescription of aspirin at discharge (odds ratio (OR) 1.29 and 1.89, p = 0.053 and p < 0.0001, respectively). Lipid lowering agents were prescribed more often on discharge in patients admitted to hospitals with catheterisation laboratories than without (for infarction with ST elevation, 45% v 40% (NS); for other acute coronary syndromes, 46% v 36%; p < 0.05). Prescription rates were higher among patients undergoing coronary angiography or PCI than in those treated conservatively (for infarction with ST elevation, 49%, 53%, and 39%, p < 0.05; for other acute coronary syndromes, 50%, 54%, and 34%, p < 0.05). Logistic regression analysis showed that PCI was an independent predictor of prescription of lipid lowering agents at discharge (OR 1.48, p < 0.0002).
Conclusions: Contrary to expectations, invasive procedures for acute coronary syndromes are associated with higher rates of prescription of pharmacological secondary prevention.
- acute coronary syndromes
- aspirin
- lipid lowering treatment
- myocardial infarction
- ACE, angiotensin converting enzyme
- ENACT, European network for acute coronary treatment
- HOPE, heart outcomes prevention trial
- PCI, percutaneous coronary intervention
Statistics from Altmetric.com
- ACE, angiotensin converting enzyme
- ENACT, European network for acute coronary treatment
- HOPE, heart outcomes prevention trial
- PCI, percutaneous coronary intervention
There is solid evidence that secondary prevention measures are effective in reducing morbidity and mortality after acute coronary syndromes. For example, the antiplatelet trialist collaboration showed that prescription of aspirin after myocardial infarction results in a reduction in cardiovascular events by approximately 25%.1 Because few patients have contraindications to aspirin treatment, prescription of this drug is appropriate for nearly all survivors of myocardial infarction. Likewise, several trials have shown the benefit of aspirin after unstable angina.2,3
Lipid lowering treatment has been found to be effective in reducing morbidity and mortality after acute coronary syndromes in patients with raised or even “average” cholesterol concentrations.4,5 Recently, observational data have suggested remarkable short term benefits among survivors of acute coronary syndromes discharged on statin treatment as opposed to patients not receiving statins,6,7 and lipid lowering treatment appears to be particularly beneficial after an unstable angina event.8 A recent trial has suggested a major benefit of early introduction of statins following acute coronary syndromes.9
β Blockers are also effective at reducing mortality and reinfarction in survivors of acute myocardial infarction,10 and angiotensin converting enzyme (ACE) inhibitors have been shown to be effective in all patients with clinical or objective evidence of heart failure or left ventricular dysfunction.10 More recently, the HOPE (heart outcomes prevention evaluation) trial showed that the benefit of ACE inhibitors might be expanded to larger groups of patients.11
Thus effective treatments are currently available for secondary prevention in patients admitted to hospital with acute coronary syndromes. However, both US and European registries suggest that there is a general underperformance in implementing secondary prevention,12–14 and recent data show only modest improvement in the rates of prescription of effective agents, with substantial numbers of patients not receiving treatment.14,15
While the underuse of secondary prevention measures is clearly documented, the reasons for such underperformance are still unclear. There is concern that part of this failure to implement secondary prevention effectively is because of an excessive focus on the early management of acute coronary syndromes, and specifically coronary interventions (for example, coronary angiography and percutaneous coronary interventions (PCI)).16 In this study we analyse the impact of the availability and use of coronary interventions on the prescription of pharmacological secondary prevention measures.
METHODS
The ENACT (European network for acute coronary treatment) registry collected prospectively pan-European information on relative frequency, diagnosis, and management of patients with acute coronary syndromes. Data were collected in 1999 from 3092 patients from 390 sites in 29 European countries. The methods and main results of the ENACT survey were published earlier.17,18 The data from ENACT were used to compare the rates of prescription of aspirin or lipid lowering agents at discharge according to the type of hospital (teaching v community, with and without a catheterisation laboratory), as well as the invasive procedures performed during the index hospital stay (coronary angiography, PCI, or neither). Similar analyses were done for in-hospital prescription of β blockers and ACE inhibitors. Data were not censored for death: in patients who died in hospital, the last treatment used was recorded and used as “discharge” treatment in the analysis. A hospital with a catheterisation laboratory was defined as one where the investigator undertook angiography on site. The data were analysed separately for the 770 patients with myocardial infarction associated with ST segment elevation within 12 hours of the onset of symptoms, and the 2322 patients with all other acute coronary syndromes.
Statistical methods
Quantitative variables are expressed as mean (SD). When included in a logistic model, they are divided into subgroups following the results of univariate analysis.
In a univariate analysis we used the unpaired Student's t test for quantitative variables and the χ2 test for qualitative variables. Univariate analysis included 18 variables: two were related to the type of hospital (teaching or community hospital, with or without catheterisation laboratory); six were related to the patients' baseline characteristics (age, sex, smoking, hypertension, dyslipidaemia, diabetes); six were related to patient management (thrombolysis, any reperfusion, coronary angiography, percutaneous transluminal coronary angioplasty, stenting, coronary artery bypass graft surgery); and four were related to outcome during the hospital admission (peak creatine kinase, heart failure, final diagnosis cardiac/non-cardiac, and final diagnosis ST elevation during the first 12 hours/other acute coronary syndromes).
Variables for which the probability value was p < 0.10 were entered in a logistic model without interactions and were selected by a backwards procedure with a significance level of p = 0.05. Adjusted odds ratios were derived from the coefficients of the final multivariate logistic model.
All analyses were performed using the SAS statistical software (SAS Institute, Cary, North Carolina, USA; release 6.11), and estimation of the coefficients of the logistic model used the logistic procedure.
RESULTS
The baseline characteristics of the patients are described in table 1 as a function of the type of hospital. When patients were examined on the basis of use of procedures (table 2), those undergoing invasive procedures were younger, less often female, more likely to have had previous revascularisation, and more likely to have received lipid lowering treatment before admission. They were also more often smokers.
Baseline characteristics of the patients as a function of hospital type
Baseline characteristics as a function of performance of invasive procedures
Prescription of aspirin at discharge
Prescription of aspirin at discharge was common across all patient subsets (table 3). There was no difference in rates of prescription of aspirin based upon the type of hospital setting (teaching v community), and rates were similar in hospitals with and without catheterisation laboratories. When rates of prescription were examined as a function of the use of invasive procedures (angiography and/or PCI), there was a consistent trend towards a higher rate of aspirin prescription among patients treated invasively (for infarction with ST elevation, 85% v 79%; for other acute coronary syndromes, 83% v 76%; NS for both comparisons). Multivariate analysis using logistic regression analysis showed that performance of PCI or coronary angiography during hospital stay were among the independent predictors of the prescription of aspirin at discharge from the hospital (odds ratio (OR) 1.89 and 1.29, respectively) (table 4).
Prescription of aspirin at time of discharge
Logistic regression analysis off predictors of aspirin at time of discharge
Prescription of lipid lowering agents
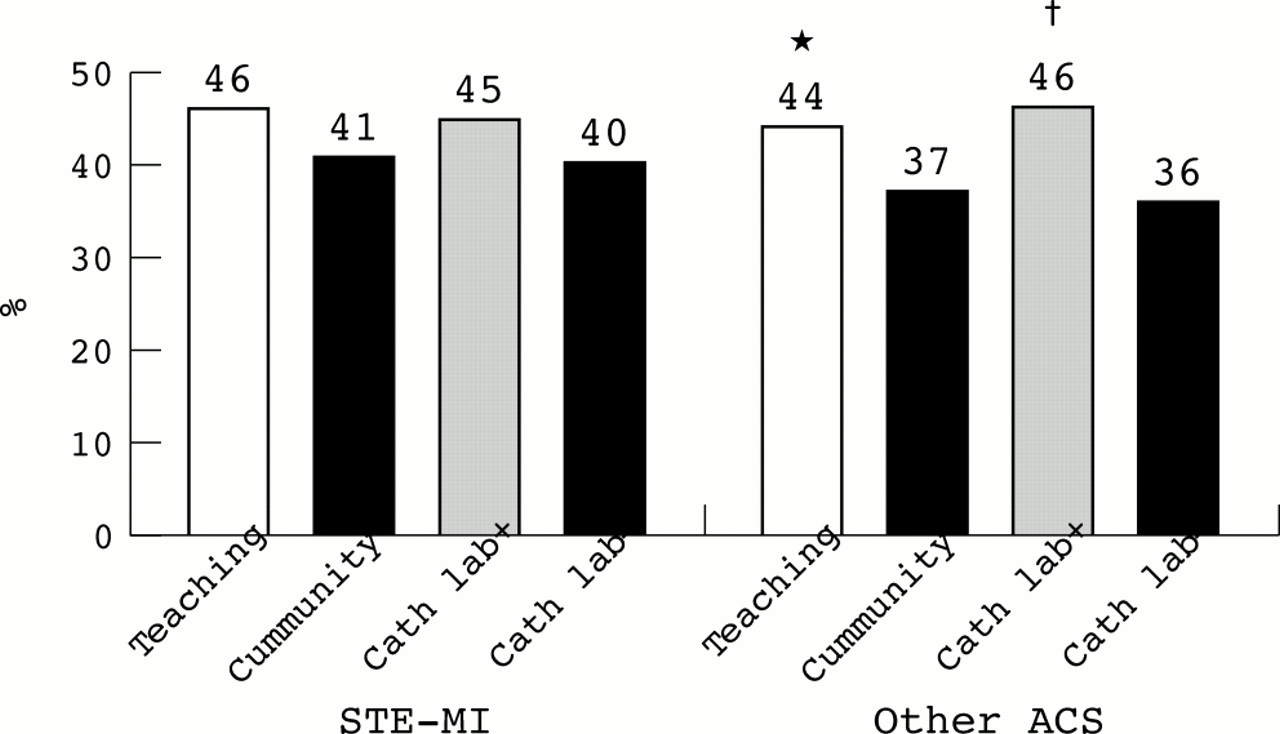
On discharge, only a minority of patients were prescribed a lipid lowering agent. There were higher prescription rates in teaching hospitals than in community hospitals (for infarction with ST elevation, 46% v 41% (NS); for other acute coronary syndromes, 44% v 37%; p < 0.05). Likewise, there were more frequent prescriptions in hospitals with catheterisation laboratories than in those without (for infarction with ST elevation, 45% v 40% (NS); for other acute coronary syndromes, 46% v 36%; p < 0.05) (fig 1). Patients undergoing angiography or PCI were more often prescribed lipid lowering agents than patients who were managed conservatively (fig 2) (for infarction with ST elevation, 49%, 53%, and 39%, p < 0.05; for other acute coronary syndromes, 50%, 54%, and 34%, p < 0.05).

Prescription of lipid lowering treatment at discharge as a function of hospital type. Cath lab+/−, hospitals with or without a catheterisation laboratory; STE-MI, ST elevation myocardial infarction; ACS, acute coronary syndromes. *p<0.05 versus community; †p<0.05 versus cath lab.

{kind=link}
{kind=link}
Prescription of lipid lowering treatment at discharge as a function of invasive procedures performed during the index hospital stay. p<0.05 versus neither; †p<0.05 versus angio and neither.
Multivariate analysis showed that, apart from being dyslipidaemic, undergoing PCI was an independent predictor of prescription of lipid lowering agents at discharge (OR 1.48, p < 0.0002) (table 5).
Multivariate analysis of predictors of prescription of lipid lowering agents at time of discharge
Prescription of β blockers and ACE inhibitors
β Blockers were prescribed to more than 60% of patients in the registry, with a higher rate of prescription in patients admitted for acute coronary syndromes other than ST elevation infarction to hospitals equipped with catheterisation laboratories (68% v 63% in hospitals without catheterisation laboratories, p < 0.05) (table 6). Likewise, when the use of these agents was analysed on the basis of procedures performed, there was more frequent use of β blockers in patients who underwent angiography or PCI for acute coronary syndromes than in patients who did not (77% and 78% v 57%, p < 0.05).
In-hospital prescription rates of β blockers and ACE inhibitors
ACE inhibitors were prescribed in more than half the patients with ST elevation infarction, with similar rates across hospital types and patient subsets (table 6). In patients with other forms of acute coronary syndromes, prescription was less frequent—generally below 50% and quite comparable across groups—although fewer patients received ACE inhibitors in hospitals with catheterisation facilities than in those without (43% v 47%, p < 0.05).
For both β blockers and ACE inhibitors, prescription is likely to be affected by important variables—such as measures of left ventricular function—which were not collected in the registry. In addition, the data collected represent in-hospital use but not prescription on discharge. Thus no sound adjustment for baseline characteristics was possible and logistic regression analysis of prescription rates was not performed.
DISCUSSION
There is a strong rationale for the widespread prescription of pharmacological secondary prevention using aspirin, lipid lowering agents, and β blockers after acute coronary syndromes, and growing evidence of the benefit of ACE inhibitors. The disappointingly low rates of prescription of these agents observed in large registries has several hypothetical explanations, such as lack of belief by physicians in their effectiveness, lag in the diffusion of guidelines, excessive attention focused on acute care,16 and so on. Understanding the factors resulting in such underperformance is critical for improving patient care and outcomes.
We addressed the concern that the current increasing use of interventional procedures may detract from paying proper attention to secondary prevention. The present data, gathered from a recent international patient cohort—similar in size and methods to the EUROASPIRE registries—suggest otherwise: in fact, invasive procedures for acute coronary syndromes are associated with a modest but significant increase in the rates of prescription of pharmacological secondary prevention, both in patients with ST elevation infarction and in those with other acute coronary syndromes. In this registry, multivariate analysis adjusting for patients and hospital characteristics showed that performance of PCI was an independent predictor of the prescription of aspirin or lipid lowering agents. Our results are in agreement with the recent findings by Fonarow and colleagues that in patients with acute myocardial infarction, performance of cardiac catheterisation or PCI during the hospital stay was independently associated with the prescription of lipid lowering agents.12 It is important to stress that, at the time of the survey (in 1999), there was less evidence of the benefit of introducing lipid lowering treatment immediately after an acute coronary syndrome,6–8 and this issue may have influenced the prescription of lipid lowering agents.
Limitations
There are certain limitations to this analysis.
Firstly, participation in the registry was voluntary; therefore the data reported here are not necessarily representative of European or national practices, as there may have been bias in the type of centres participating. It is, however, worth pointing out that a high proportion of patients enrolled into the ENACT study were recruited in community hospitals and in institutions without an on-site catheterisation laboratory.
Secondly, the data were provided by the participating centres and therefore there may have been some over declaration of secondary prevention measures in certain types of hospital.
Thirdly, our adjusted analyses rely on a relatively limited number of patient and hospital characteristics collected within the scope of ENACT and should be interpreted with caution, as a residual confounding effect from unmeasured factors cannot be excluded.19
Finally, the treatments studied are by no means the only effective methods of secondary prevention, and dietary advice, smoking cessation, and other non-pharmacological and pharmacological interventions to reduce weight, implement exercise, and control other risk factors for coronary artery disease are also crucial to the ultimate prognosis of patients with acute coronary syndromes. However, the treatments examined have been proved clearly effective, and indeed their prescription represents processes of care directly and sensitively linked to outcome.20,21 Non-pharmacological secondary prevention measures (for example, dietary advice and advice on smoking cessation) are very important and their implementation was not assessed in ENACT. However, it is likely that non-pharmacological measures tend to “track” the prescription of drugs for secondary prevention. In addition, only a minority of patients treated for raised cholesterol in secondary prevention achieve target concentrations,22 and the use of pharmacological agents to lower cholesterol is a predictor of success in achieving target concentrations of cholesterol.22
Conclusions
In this analysis of the ENACT registry, it appears that invasive procedures for acute coronary syndromes are associated with higher rates of prescription of aspirin and lipid lowering agents at discharge, both in patients with myocardial infarction associated with ST elevation and in patients with other acute coronary syndromes. Performance of PCI is an independent predictor of prescription of aspirin or lipid lowering agents. In addition, admission to hospitals with catheterisation laboratories was associated with a higher rate of prescription of lipid lowering agents. These data suggest that the current trend towards increased use of invasive procedures is not responsible for the insufficient rates of prescription of secondary prevention agents.
Acknowledgments
We are indebted to the participants in the ENACT survey. A complete list of the ENACT investigators is included in reference 16. In addition, we are grateful for logistical support from Medical Action Communications UK, and specifically Christine Drewienkiewicz. ENACT was supported by an educational grant from Schering-Plough pharmaceuticals.