Article Text

Abstract
Objective: To determine the prognostic and therapeutic implications of stress perfusion cardiovascular magnetic resonance (CMR) on the basis of the ischaemic cascade.
Setting: Single centre study in a teaching hospital in Spain.
Patients: Dipyridamole stress CMR was performed on 601 patients with ischaemic chest pain and known or suspected coronary artery disease. On the basis of the ischaemic cascade, patients were categorised in C1 (no evidence of ischaemia, n = 354), C2 (isolated perfusion deficit at stress first-pass perfusion imaging, n = 181) and C3 (simultaneous perfusion deficit and inducible wall motion abnormalities, n = 66). CMR-related revascularisation (n = 102, 17%) was defined as the procedure prompted by the CMR results and carried out within the next three months.
Results: During a median follow-up of 553 days, 69 major adverse cardiac events (MACE), including 21 cardiac deaths, 14 non-fatal myocardial infarctions and 34 admissions for unstable angina with documented abnormal angiography were detected. In non-revascularised patients (n = 499), the MACE rate was 4% (14/340) in C1, 20% (26/128) in C2 and 39% (12/31) in C3 (adjusted p value = 0.004 vs C2 and <0.001 vs C1). CMR-related revascularisation had neutral effects in C2 (20% vs 19%, 1.1 (0.5 to 2.4), p = 0.7) but independently reduced the risk of MACE in C3 (39% vs 11%, 0.2 (0.1 to 0.7), p = 0.01).
Conclusions: Dypiridamole stress CMR is able to stratify risk on the basis of the ischaemic cascade. A small group of patients with severe ischaemia—simultaneous perfusion deficit and inducible wall motion abnormalities—are at the highest risk and benefit most from MACE reduction due to revascularisation.
Statistics from Altmetric.com
In patients with ischaemic heart disease, stress perfusion cardiovascular magnetic resonance (CMR) has been incorporated into daily practice for diagnostic purposes.1–3 Data regarding the prognostic value of CMR are scarce.4 5 The therapeutic implications of CMR and its usefulness to guide revascularisation is still unknown.
Two decades ago, the ischaemic cascade was described as a sequence of steps occurring in each ischaemic episode.6 Stress perfusion CMR is now used for routine clinical application and allows accurate assessment of two important steps in the ischaemic cascade—perfusion deficit and inducible wall motion abnormalities (WMA)—the most commonly used indices to identify non-invasively the presence of physiologically significant coronary lesions.1–5 7 8
The purpose of this study was to determine the prognostic and therapeutic implications of dipyridamole stress CMR in patients with ischaemic chest pain and known or suspected ischaemic heart disease on the basis of the ischaemic cascade.
METHODS
Study group
This is an ongoing registry. The inclusion criteria and the study protocol have been described elsewhere.4
The study group was made up of 601 consecutive patients with chest pain of possible coronary origin and known or suspected coronary artery disease who were submitted from the outpatient clinic, between January 2003 and January 2007, to undergo dipyridamole stress CMR. Reasons for stress CMR were: an inconclusive exercise test (20%), an altered ECG (20%), inability to exercise (26%), evaluation of the severity of intermediate lesions (10%) and as first choice in the investigation of patients (24%).
Exclusion criteria were a history of myocardial infarction or coronary revascularisation within the previous three months, clinical instability, asthma, any contraindications to CMR and a follow-up of less than 6 months.
All data were prospectively recorded and follow-up was periodically updated. The CMR results were available to the cardiologists in charge of patients.
CMR study
All patients were examined with a 1.5-T system (Sonata Magnetom, Siemens, Erlangen, Germany). All images were acquired by a phased-array body surface coil during breath-holds and were electrocardiogram-triggered.
Left ventricular volumes, ejection fraction and mass were assessed using cine images in two-chamber, three-chamber, four-chamber views and in short-axis views using a steady-state free precession sequence (SSFP, repetition time/echo time: 2.8/1.2 ms, flip angle: 58°, matrix: 256×256, field of view: 320×270 mm, slice thickness: 6 mm).
Segmental systolic function at rest was also assessed using a fast acquisition multislice SSFP cine image sequence (repetition time/echo time: 35/1.1 ms, flip angle: 65°, matrix: 192×159, field of view: 350×304 mm, slice thickness: 8 mm). Over a 14-second period, four slices in the short-axis view were acquired. Afterwards, over a 7-second period, two sections in the two-chamber and four-chamber long-axis views were acquired.
Vasodilatation was induced with dipyridamole (0.56 mg/kg body weight over 4 minutes and, if well tolerated, 0.84 mg/kg body weight was delivered intravenously over 6 minutes). After finishing dipyridamole infusion, 0.1 mmol/kg gadopentate dimeglumine (Magnograf, Schering AG, Berlin, Germany) was injected intravenously at a speed of 5 ml/s. Then, five sections equally separated in the short-axis view and two in the two-chamber and four-chamber long-axis views were acquired every other beat for first-pass perfusion imaging (SSFP with a notched saturation pulse, inversion time: 125 ms, repetition time/echo time: 202 ms/1 ms, flip angle: 50°, matrix: 192×96, field of view: 350×220 mm, slice thickness: 8 mm).
Perfusion imaging was visually evaluated in real time by an experienced operator. Once the peak myocardial enhancement was reached, in order to assess segmental systolic function within the peak dipyridamole-induced vasodilatation (approximately 2–3 minutes after infusion), we used the same fast acquisition sequence and reference locations used for assessing segmental systolic function at rest. In general, only short-axis views (over 14 seconds) were acquired. Analysis of long-axis views at peak stress was left to the discretion of operators. In all those patients in whom, during first-pass perfusion imaging, a perfusion defect in segment 17 was suspected, two long-axis views (over an additional 7-second period) were acquired to evaluate apical systolic function at peak stress.
Late enhancement imaging was performed 10 minutes after contrast injection in the same locations evaluated for cine images at rest (segmented inversion recovery SSFP, repetition time/echo time: 700/1.26 ms, flip angle: 45°, matrix: 256×184, field of view: 340×235 mm, slice thickness: 8 mm). The inversion time was adjusted to null normal myocardium.
CMR data analysis
CMR studies were analysed offline by an experienced observer blinded to all patient data and using customised software (Syngo, Siemens, Erlangen, Germany).
Ejection fraction, end-diastolic volume and end-systolic volume (Simpson’s method) were calculated by manual planimetry of all short-axis views.
The 17-segment model was applied.9 We visually evaluated five indices:
WMA at rest. Number of segments showing hypokinesis, akinesis or dyskinesis at baseline.
WMA with dipyridamole. Number of segments showing hypokinesis, akinesis or dyskinesis at stress.
Inducible WMA. Number of segments in which wall motion worsened with dipyridamole from normokinesis to hypokinesis or from hypokinesis to akinesis.
Perfusion deficit with dipyridamole. Number of segments showing persistent delay (in at least three consecutive temporal images in comparison with other segments in the same slice) in the visual analysis of the enhancement pattern during the first pass of contrast through the myocardium.10
Delayed enhancement. Number of segments showing enhancement in delayed enhancement imaging.
CMR indexes were categorised according to the best cut-off value in receiver-operating characteristic curves (0–1 segment vs >1) to predict major adverse cardiac events (MACE) during follow-up.4 In our laboratory, interobserver agreement concerning all CMR indices is >90%.4
On the basis of the ischaemic cascade,6 7 and following the established rationale to consider that dipyridamole stress CMR suggests the presence of physiologically significant coronary lesions,1–5 8 10 we categorised the study group into:
C1: No evidence of ischaemia. Normal perfusion without inducible WMA (fig 1, see video 1 on Heart website).
C2: Perfusion deficit (>1 segment) without inducible WMA (fig 1, see video 2 on Heart website).
C3: Simultaneous perfusion deficit (>1 segment) and inducible WMA (>1 segment) (fig 1, see video 3 on Heart website).

CMR-related revascularisation
CMR-related revascularisation was defined as percutaneous coronary interventions (PCI) and coronary artery bypass grafting (CABG) prompted by the CMR results and carried out within the next 3 months. In our health system this is a reasonable period of time to consider that the CMR results exerted a decisive influence on patient management.
CMR-related cardiac catheterisation was performed in 192 patients (32%): 39 in C1 (11%), 99 in C2 (55%) and 54 in C3 (82%).
CMR-related revascularisation was performed in 102 patients (17%): 14 in C1 (4%, all PCI), 53 in C2 (29%, 45 PCI and 8 CABG) and 35 in C3 (53%, 26 PCI and 9 CABG).
End point and follow-up
The follow-up data were obtained from at least one of four sources: (1) a cardiologist visiting the patient in the outpatient clinic; (2) a telephone interview with the patient conducted by a cardiologist; (3) personal communication with the patient’s physician and review of the patient’s chart; or (4) review of the patient’s hospital record.
The end point was major adverse cardiac events (MACE) and included cardiac death, non-fatal myocardial infarction and admission for unstable angina (whichever occurred first). Admission for unstable angina required the presence of chest pain with unstable characteristics leading to hospital admission and evidence of abnormal coronary angiogram. All MACE were reviewed and consensus between two cardiologists was required to finally designate a MACE.
For prognostic purposes, in order to avoid the effect of revascularisation on the spontaneous evolution of patients, we excluded those 102 patients who had undergone a CMR-related revascularisation procedure.
Taking into account the low MACE rate (17/354, 5%) and the low revascularisation rate (14/354, 4%) in group C1, the effects of revascularisation on patient outcome in the multivariate analyses was evaluated only in groups C2 and C3.
Statistical analysis
Continuous data were expressed as the mean (SD), and were compared by the unpaired t test. Proportions were compared by the χ2 statistic; the Fisher exact test was used when appropriate. Survival distributions for the time to event were estimated using the Kaplan-Meier method and the log-rank test.
The association of groups C1, C2 and C3 with the MACE rate in non-revascularised patients (n = 499) was estimated by calculating the hazard ratios with the corresponding 95% confidence intervals (HR (95% CI)) adjusted for variables shown in tables 1 and 2 associated with the presence of MACE (with a p value <0.2 in the univariate analyses).
This was not a randomised study. In order to correct the inherent referral bias, we created a propensity score for revascularisation—this representing the probability of each patient undergoing CMR-related revascularisation. We tested all variables included in tables 1 and 2 in a stepwise logistic regression model. The accuracy of the propensity score was evaluated by means of the C-statistic of the final model.11
The effects of revascularisation on patient outcome in groups C2 and C3 were then estimated calculating the HR (95% CI) adjusted for the propensity score and for variables shown in tables 1 and 2 associated to the presence of MACE (with a p value <0.2 in the univariate analyses). This effect was further assessed by analysing the interaction of revascularisation with MACE in the multivariate model.
Statistical significance was considered for p<0.05. SPSS 11.0 and Stata 9.0 were used throughout.
RESULTS
All patients were followed up for at least 6 months (mean 640 (360) days, range 182–1603 days, median 553 days); 69 MACE including 21 cardiac deaths, 14 non-fatal myocardial infarctions and 34 admissions for unstable angina with documented abnormal angiography were detected. The baseline and the CMR characteristics of the whole group and of patients with and without MACE are shown in tables 1 and 2.
Out of 601 patients, the C1 group comprised 354 patients (59%) with no evidence of ischaemia, the C2 group had 181 patients (30%) with isolated perfusion deficit and the C3 group had 66 patients (11%) with simultaneous perfusion deficit and inducible WMA. All patients with inducible WMA displayed a perfusion deficit. C3 associated to a significantly larger perfusion deficit (7.4 (3.2) segments) than C2 (5.6 (2.8) segments) and C1 (0.03 (0.2) segments), p<0.001 in all cases.
In the whole group (n = 601), the MACE rate was 5% (17/354) in C1, 20% (36/181) in C2 and 24% (16/66) in C3, p<0.001 C2 and C3 vs C1; p = 0.4 C3 vs C2.
In spite of not showing a perfusion deficit or inducible WMA, 35 patients in the C1 group (10%) displayed WMA at rest. The presence of WMA at rest was associated with a higher MACE rate (7/35 (20%) vs 10/319 (3%), p<0.001).
In the C1 group all patients had 0 or 1 segments with inducible WMA. The MACE rate was 16/342 (5%) in patients with 0 segments with perfusion deficit vs 1/12 (8%) in patients with one isolated segment with perfusion deficit, p = 0.4.
MACE in non-revascularised patients
In non-revascularised patients (n = 499), the MACE rate was 4% (14/340) in C1, 20% (26/128) in C2 and 39% (12/31) in C3 (p<0.001 for the trend).
In the multivariate analysis (fig 2, table 3), adjusted for variables shown in tables 1 and 2, groups C2 (p = 0.001) and C3 (p<0.001) independently increased the risk of MACE in comparison with C1, and group C3 in comparison with C2 (p = 0.004).

Revascularisation and MACE
In the C1 group, the reason for revascularisation was refractory chest pain. Revascularised patients had more MACE (3/14 (21%) vs 14/340 (4%), p = 0.02). Owing to the good spontaneous evolution (5% MACE rate overall) and the low revascularisation rate (4%) in group C1, the effects of revascularisation on patient outcome in the multivariate analyses was only evaluated in groups C2 and C3.
We created a propensity score to quantify the individual probability of patients undergoing revascularisation by testing all variables included in tables 1 and 2 in a stepwise logistic regression model. Male sex, the extent of perfusion deficit and the extent of inducible WMA persisted as independent predictors for undergoing revascularisation. The accuracy of the propensity score was confirmed by means of the C-statistic in the final model (0.83).
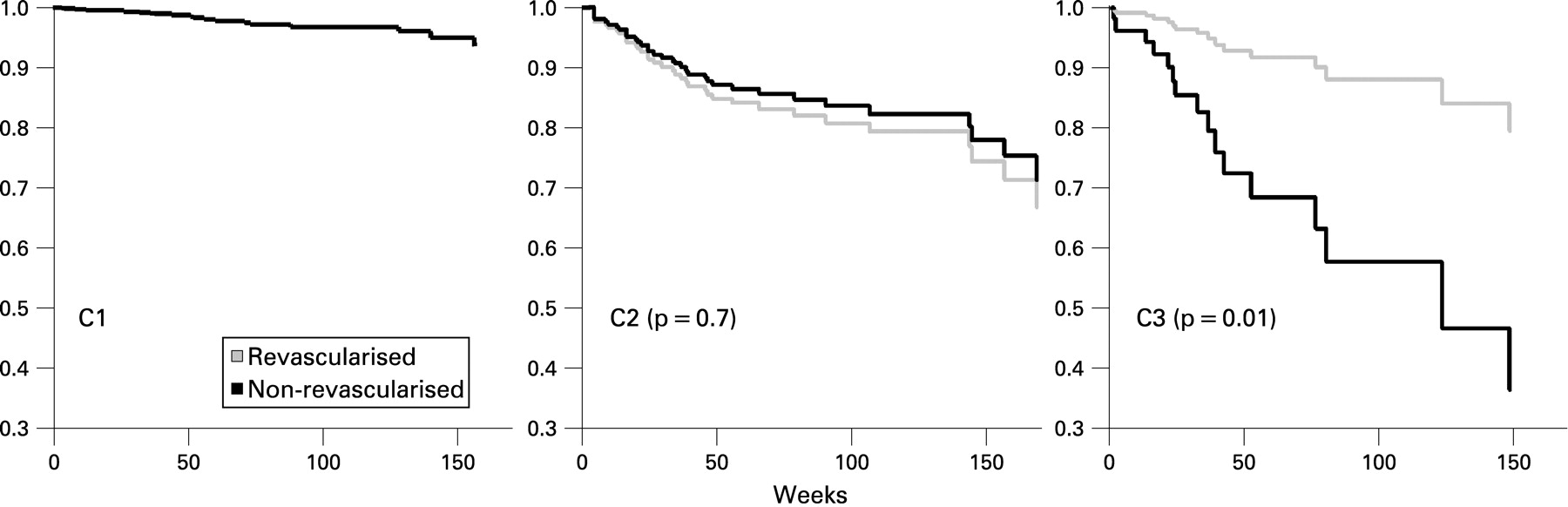
In univariate analysis (table 4), revascularisation had a neutral effect in the C2 group (19% vs 20%, p = 0.9) and reduced the risk of MACE in the C3 group (11% vs 39%, p = 0.01).
Once adjusted for the propensity score and for variables shown in tables 1 and 2 (fig 3, table 4), revascularisation independently reduced the risk of MACE only in the C3 group (p for interaction = 0.01).
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The main finding of the present study is that in patients with ischaemic chest pain and known or suspected coronary artery disease in a stable phase, dipyridamole stress CMR on the basis of the ischaemia cascade is useful to stratify risk and to predict the effect of revascularisation on the event rate. A small group of patients, those with severe ischaemia, are at highest risk and benefit most from MACE reduction due to revascularisation.
Stress perfusion CMR and prognosis
CMR is becoming the preferred technique for evaluating patients with ischaemic heart disease.1 12–15 Besides diagnosis, the validation of prognostic significance has expedited the incorporation of CMR into daily practice.15 16
Only two studies have addressed the prognostic implications of stress perfusion CMR so far.4 5 By analysing the first 420 patients included in this registry we have recently demonstrated that the extent of WMA at stress (as a whole) was the best CMR index to predict patient outcome.4
Our results illustrate the ability of dipyridamole stress CMR to stratify risk on the solid physiological basis of the ischaemic cascade.7 After a comprehensive multivariate analysis, perfusion deficit (as an initial step in the ischaemic cascade) doubled and inducible WMA (as an advanced step of the ischaemic cascade) almost quadrupled the risk of MACE in comparison with patients with no evidence of ischaemia.
While CMR imaging offers excellent spatial resolution for the assessment of subtle changes in myocardial contractility, since the advent of myocardial perfusion imaging using vasodilators the focus has shifted away from stress-induced WMA to stress-induced perfusion deficit. Inducible WMA using vasodilators is infrequent and it relates to severe ischaemia. Paetsch et al8 observed that adenosine-induced WMA occurred in segments with at least 75% transmural perfusion deficit and associated with severe (>75%) coronary stenosis. Nevertheless, dobutamine-induced WMA was detected in less severe (>50%) coronary lesions.
Dobutamine-induced WMA seems to depend more on increased myocardial demand8 17 than on induced perfusion deficit. This different pathophysiological mechanism probably explains why Elhendy et al,17 using dobutamine and single-photon emission computed tomography, did not detect a significant association between the presence of inducible WMA and the extent of the perfusion deficit. Similarly to Paetsch et al,8 we observed that the extent of the perfusion defect was larger in patients with dipyridamole-inducible WMA than in those with isolated perfusion deficit. Though dipyridamole is less potent than dobutamine in inducing WMA, such lesser potency can be advantageous for prognostic purposes because a small group of patients with severe, clinically significant ischaemia (those with inducible WMA) can be defined.8 Actually, in our study group, those patients with simultaneous perfusion deficit and inducible WMA displayed the highest risk of MACE.
This study represents the largest series of patients for analysing the prognostic implications of stress perfusion CMR so far and it is the first to demonstrate that, using CMR, inducible WMA offers additional prognostic value in combination with perfusion data, making stress CMR a truly comprehensive approach in the evaluation of ischaemia.
Therapeutic implications of stress perfusion CMR
Extrapolating beyond acute coronary syndromes, the beneficial effect of revascularisation in terms of event rate reduction is controversial. Recently, Boden et al18 reported the results of a randomised study suggesting that PCI did not reduce the risk of death, myocardial infarction or other cardiovascular events when added to optimal medical therapy.
In order to reduce clinical events, recent guidelines recommend revascularisation only in patients with clear evidence of ischaemia,19 highlighting the fact that the physiological significance of coronary lesions rather than the mere presence of coronary plaques is of major concern. Therefore, along with a comprehensive clinical evaluation of patients and the valuable information provided by exercise ECG,20 cardiac imaging techniques have a central role in the decision-making process of patients with stable coronary artery disease.15 16 19 The usefulness of stress CMR for making therapeutic decisions has not been proved so far, however.
The majority of our study group did not show evidence of ischaemia in CMR. In this scenario, medically treated patients displayed a very low MACE rate. Actually, the small group of patients who underwent revascularisation despite the absence of myocardial ischaemia displayed a high MACE rate. These data support the value of stress CMR in making decisions: revascularisation seemed to bring about detrimental effects in those few patients without ischaemia who underwent revascularisation.
A third of the study group showed perfusion deficit without inducible WMA, an initial step of the ischaemic cascade.6 7 These patients were at intermediate risk but medical treatment and revascularisation resulted in an identical MACE rate. It could be speculated that invasive management improves quality of life and reduces chest pain episodes.19 In the absence of severe ischaemia, however, decisions should be made on a patient-to-patient basis, keeping in mind that great benefits in terms of event rate reduction from revascularisation cannot be expected.
Only a small subset of patients (11% of the whole group) on an advanced step in the sequence of the ischaemic cascade—namely, simultaneous perfusion deficit and inducible WMA, statistically benefited from revascularisation in terms of MACE reduction. With medical treatment they had the highest MACE rate during follow-up.
Our results confirm recent studies18 21 and recommendations19 suggesting that revascularisation does not bring about a generalised reduction in event rate. Interestingly, stress perfusion CMR was able to identify a small subset of patients, those with severe ischaemia, in whom revascularisation exerted beneficial effects in terms of MACE reduction.
Limitations
This was not a randomised study. We included in the multivariate analysis a propensity score to undergo revascularisation. Although adjusting by propensity score is an accepted statistical approach,11 we cannot exclude the fact that the inherent referral bias could alter our results concerning the therapeutic implications of stress CMR results.
Revascularisation in clinical practice is based on a variety of variables; therefore CMR results cannot be considered the only factor that prompted patient management. The cardiac catheterisation and revascularisation rates within the predefined three-month period were much higher if stress CMR suggested the presence of myocardial ischaemia—this strongly indicates that CMR exerted a decisive influence on patient management, however.
CONCLUSIONS
In patients with chest pain and known or suspected coronary artery disease, without acute coronary syndromes, dypiridamole stress CMR can be useful in stratifying patients at very low risk, those with no evidence of ischaemia, in whom a conservative management is warranted. Patients with an isolated perfusion deficit are at moderate risk but, as a whole, medical therapy results in a similar event rate in comparison with revascularisation. On the basis of the ischaemic cascade, dypiridamole stress CMR is able to identify a small group of patients at high risk with severe ischaemia—namely, simultaneous perfusion deficit and inducible WMA, in whom an invasive approach can exert beneficial effects in terms of MACE reduction.
REFERENCES
Supplementary materials
web only media 95/1/49
Files in this Data Supplement:
Footnotes
▸ Additional images in the form of videos are published online only at http://heart.bmj.com/content/vol95/issue1
Funding: This work was supported by the grants “Bayer” from the Spanish Society of Cardiology and “HERACLES” fom the “Spanish Ministry of Health”.
Competing interests: None.
Ethics approval: The local ethics committee approved the research protocol. Informed consent was obtained from all subjects.