Article Text

Abstract
Objective: To assess the clinical and cost effectiveness of a brief home-based cognitive behavioural rehabilitation programme (the ICD Plan) for patients undergoing implantation of a cardiac defibrillator.
Design: A prospective multicentred, intention-to-treat, cluster-randomised controlled trial.
Setting: Eight implantable cardioverter-defibrillator (ICD) implantation centres in the UK.
Patients: Consecutive series of patients undergoing implantation with an ICD.
Interventions: The control group received usual care and advice from an experienced healthcare professional. The intervention group received usual care plus the ICD Plan. The plan was introduced before implantation, with three further brief telephone contacts with the nurse over the next 12 weeks.
Main outcome measures: Health-related quality of life (Short Form Health Survey (SF-12)), anxiety and depression (Hospital Anxiety and Depression Scale (HADS)), activity limitations (subscale from the Seattle Angina Questionnaire (SAQ)), unplanned admissions and other economic data using a questionnaire developed for the study.
Results: 192 patients were recruited to the study (71 intervention, 121 control). At 6 months after surgery the intervention group had better physical health (37.83 vs 34.24; p<0.01), fewer limitations in physical activity (34.02 vs 31.72; p = 0.04), a greater reduction in the proportion of patients with a borderline diagnosis of anxiety (21% vs 13%; p = 0.60) and depression (13% vs 2%; p = 0.30), more planned ECGs (89% vs 66%; p = 0.04) and 50% fewer unplanned admissions (11% vs 22%; p<0.01).
Conclusions: The ICD Plan improved health-related quality of life, reduced the incidence of clinically significant psychological distress and significantly reduced unplanned readmissions. It is a cost effective and easily implemented method for delivering rehabilitation and psychological care to patients undergoing ICD implantation.
Trial registration number: ISRCTN70212111.
Statistics from Altmetric.com
Implantable cardioverter-defibrillators (ICDs) have been found to be clinically effective1–4 for the primary and secondary management of life-threatening ventricular arrhythmias. Earlier studies found them to be cost effective.5 6 The National Institute of Health and Clinical Excellence (NICE) in the United Kingdom advocates wider use of ICDs,7 but a recent paper concluded that because of the way they are currently used in the UK they may not meet criteria for cost effectiveness owing to the high rate of admission to hospital after implantation.8
The device brings with it a set of psychosocial challenges for the patient and their family and there is known to be a significant degree of psychosocial morbidity associated with being a recipient; a recent study found that 46% were anxious and 41% were depressed.9 Some patients become unnecessarily disabled because they fear that any untoward activity or excitement may trigger a firing of the device.10 If a firing is experienced they often blame the activity they were taking part in at the time of the firing. While this attribution of cause allows the ICD patient to make sense of events, the activity is often abandoned or severely curtailed.11 These and other common misconceptions are predictive of anxiety and depression.12 13
Cognitive behaviour therapy delivered by a psychologist14 has been shown to benefit ICD patients by reducing anxiety and depression. It has been claimed that this may lead to fewer firings of the device.15 Cardiac rehabilitation can also reduce anxiety, depression and disability and improve secondary prevention. A cognitive behavioural cardiac rehabilitation programme, the Heart Manual, delivered at home, facilitated by brief contacts with a healthcare worker has been shown to provide identical benefits to those of hospital-based programmes.16 Both the Heart Manual and the Angina Plan, a home-based rehabilitation programme for people with angina, have been widely adopted in the National Health Service (NHS) in the UK16 17 and it is clear that many patients prefer home-based rehabilitation.18 Responses from a national survey of staff working with ICD patients19 suggested wide support from clinical staff for developing a similar home-based rehabilitation package for ICD patients.
The aim of this study was to evaluate the clinical and cost effectiveness of a home-based rehabilitation plan for patients with an implantable cardiac defibrillator (the ICD Plan).
METHODS
Study design
Full ethical approval was gained before the start of the study and the study was undertaken in accordance with the Helsinki Declaration. The study was a pragmatic prospective cluster randomised controlled trial. Cluster randomisation was necessary to minimise the possibility of contamination. To deal with the problems associated with resentful demoralisation, control centres were offered the same training and access to the ICD Plan as the intervention centres at the end of the study period. Centres were allocated to either intervention or control using a block randomisation algorithm independent of the research group.
Inclusion criteria
Study sites were eligible if they had an implantation volume of at least five ICDs a month and had on-site support from a cardiac healthcare professional who could take part in the brief training in using the ICD Plan and deliver the intervention as part of their care routines.
Patients were eligible if they were aged ⩾18 years, if it was their first ICD implantation and they were able and willing to provide informed consent.
Exclusion criteria
Patients were excluded from the study if they were medically unsuitable according to the judgment of a cardiologist, currently awaiting coronary artery bypass grafting or heart transplantation, known to suffer from exercise-induced arrhythmias, had a diagnosis of angina pectoris CCS III and IV, had a comorbid life-threatening condition or a documented history of psychotic illness.
Procedures
The ICD Plan
Healthcare staff in the intervention centres participated in a half-day training session delivered by a clinical psychologist. Training consisted of a mixed format using presentations, case studies, role playing and clinical scenarios. The training dealt with a number of topics, including risk factors and their reduction, the psychology of cardiac disease, cardiac concerns and misconceptions, goal setting and pacing, the overactivity and rest cycle, self-management of anxiety and low mood, basic breathing and relaxation techniques and basic principles of cognitive behavioural therapy.
The ICD Plan comprised two patient-held booklets, a booklet for relatives, a goal-setting diary and a relaxation tape or CD. The first booklet was given to patients while they were awaiting implantation. It dealt with common fears experienced by patients before surgery. These were identified from consultation with ICD patients, healthcare staff and the research. It targeted the specific ICD concerns that have been shown to lead to increased disability and anxiety and depression,13 and introduced relaxation and better breathing to help patients cope with the “stress” of surgery and ICD implantation. The second booklet explained the best way “to get back to normal and to avoid further problems”. It was a cognitive behavioural rehabilitation programme in self-help form. The facilitator and the patient, and when possible the family, discussed the patient’s rehabilitation needs and set some simple initial goals. The patient and facilitator made contact three more times by phone, at weeks 1, 3 and 6 after discharge, to discuss progress, reinforce success and to set new goals.
Normal care
In control centres patients were also seen by a specialist arrhythmia nurse or ECG physiologist who carried out their usual care. Patients were educated about the procedure and on how to cope after discharge. To control for attention and time, control group patients were provided with a generic information booklet developed by the British Heart Foundation20 and contacted by the facilitator to discuss postoperative progress.
Recruitment
Consecutive patients attending for implantation between February 2004 and May 2005 were approached by a facilitator in each centre and assessed for eligibility. If a patient was eligible, the study was explained, and they were provided with a written information sheet. Patients who provided informed written consent were provided with either usual care or the ICD Plan, depending upon the centre’s allocation.
Outcomes were measured at preimplantation, before provision of the ICD Plan and 6 months after implantation. Outcomes were assessed using a patient self-completed questionnaire. Data on appropriate shocks were collected from information downloaded from devices during routine clinic appointments.
Outcome measures
Anxiety and depression, the primary outcome, was measured using the Hospital Anxiety and Depression Scale (HADS).21 HADS is a 14-item instrument with two subscales measuring anxiety and depression, with higher scores indicating greater psychological morbidity. A score of eight or more on either subscale indicates borderline anxiety or depression.22 Health-related quality of life was measured using the Short Form Health Survey (SF-12), an established generic 12-item instrument that assesses both physical and mental components of quality of life.23 Changes in the functional status of the sample were measured using the physical limitations subscale of the Seattle Angina Questionnaire (SAQ).24 Data on the number of shocks and ICD storms (three or more ICD shocks in any 24 h period) in the 6 months after implantation were provided by the electrophysiologist at each centre. Service utilisation was measured using self-completed questionnaires developed for the measurement of health economic events in randomised controlled trials.25
Measurement of treatment costs
We measured the time nurses spent in training, taking into account a cost associated with space and materials. We extrapolated this training cost across the number of patients who would receive the intervention before retraining would be required to gain a pragmatic estimate of training costs. We also estimated the time each nurse in the intervention group would spend with each patient in delivering the intervention over and above usual care.
Measurement of healthcare resources
We used a questionnaire developed by members of the research team to gather economic resource use data in a number of other randomised evaluations.25 We chose a period of 6 months so as to capture important but infrequent events within the patients’ recall. We measured both defibrillator-related and non-defibrillator-related resource use. We measured resource use arising through both primary and secondary care and the associated costs of inpatient stays and emergency admissions. We estimated unit costs of each resource from national sources.26
Sample size calculation
The sample size was based upon a clinically important effect size difference of 0.5 between the groups on anxiety and depression. Detection of this difference at the 0.05 significance level with 80% power requires 64 patients in each group, control and intervention. Because the study is a cluster design we needed to take into account the design effect in our sample size calculations. Assumption of an intraclass correlation coefficient of 0.01 inflated the required sample to 86 patients in each group. Taking into account a potential loss to follow-up of 10% in each group at 6 months, increased this figure to a total sample of 188.
Statistical analysis
Statistical analysis was conducted using an intention-to-treat approach, in which patients were analysed as part of the group to which they were randomised rather than according to the treatment they received. This approach provides a pragmatic interpretation of the effectiveness of a given intervention. We used two-sided significance tests to analyse the outcomes. We analysed the differences between the intervention and control groups 6 months after implantation. We adjusted the analysis for preimplantation score and centre using analysis of covariance. We used multilevel modelling to make allowance for the innate clustering of patients within centres. Changes in the number of patients considered borderline or cases of anxiety or depression were analysed using a χ2 test. All data were analysed using SPSS, version 12.
Economic analysis
We improved estimates of quality-adjusted life years (QALYs) by adjusting for baseline measurements. While analysis of covariance yield more precise estimates, the nature of the data collected in this study violates some of the assumptions of covariance. It was considered more appropriate to analyse changes between baseline and follow-up.27
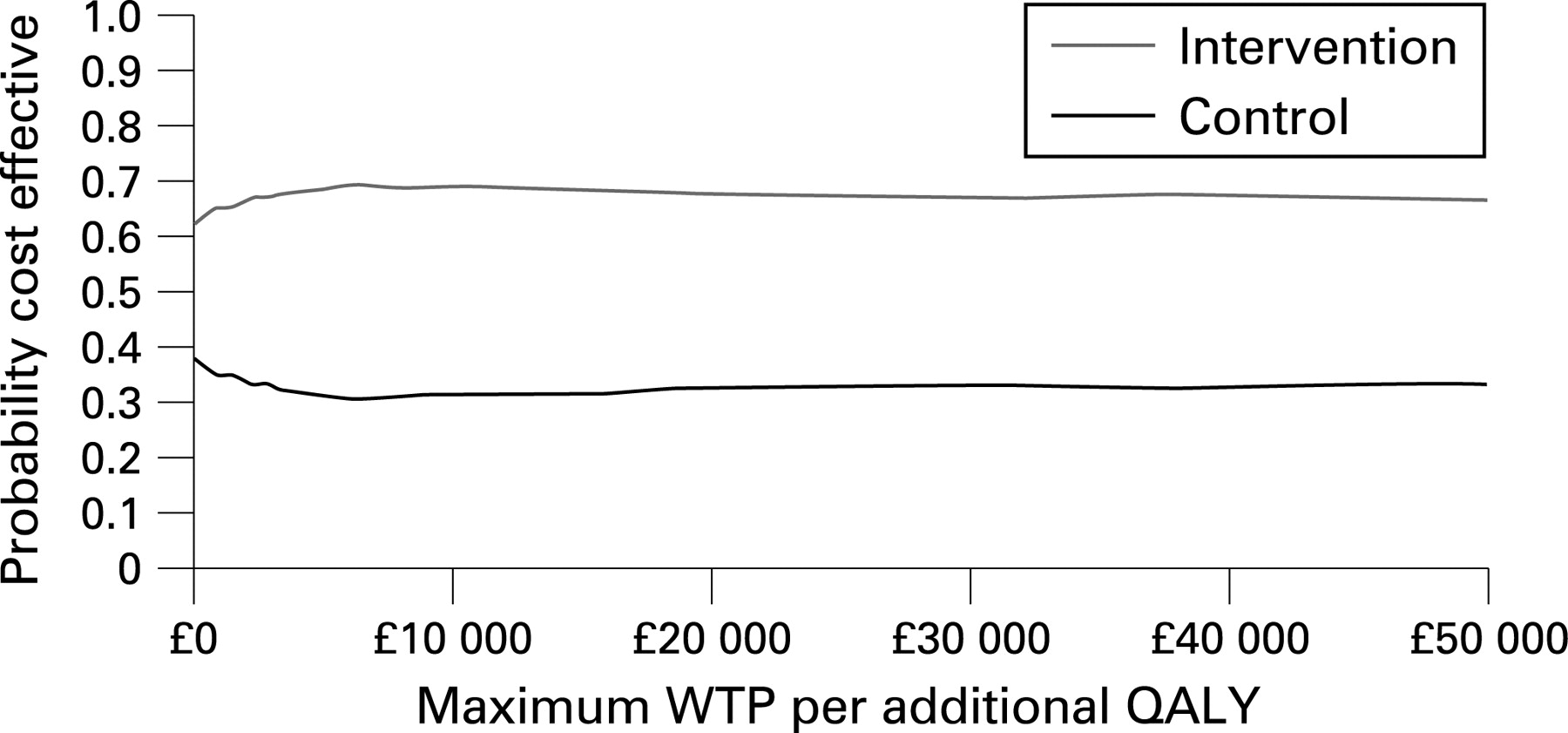
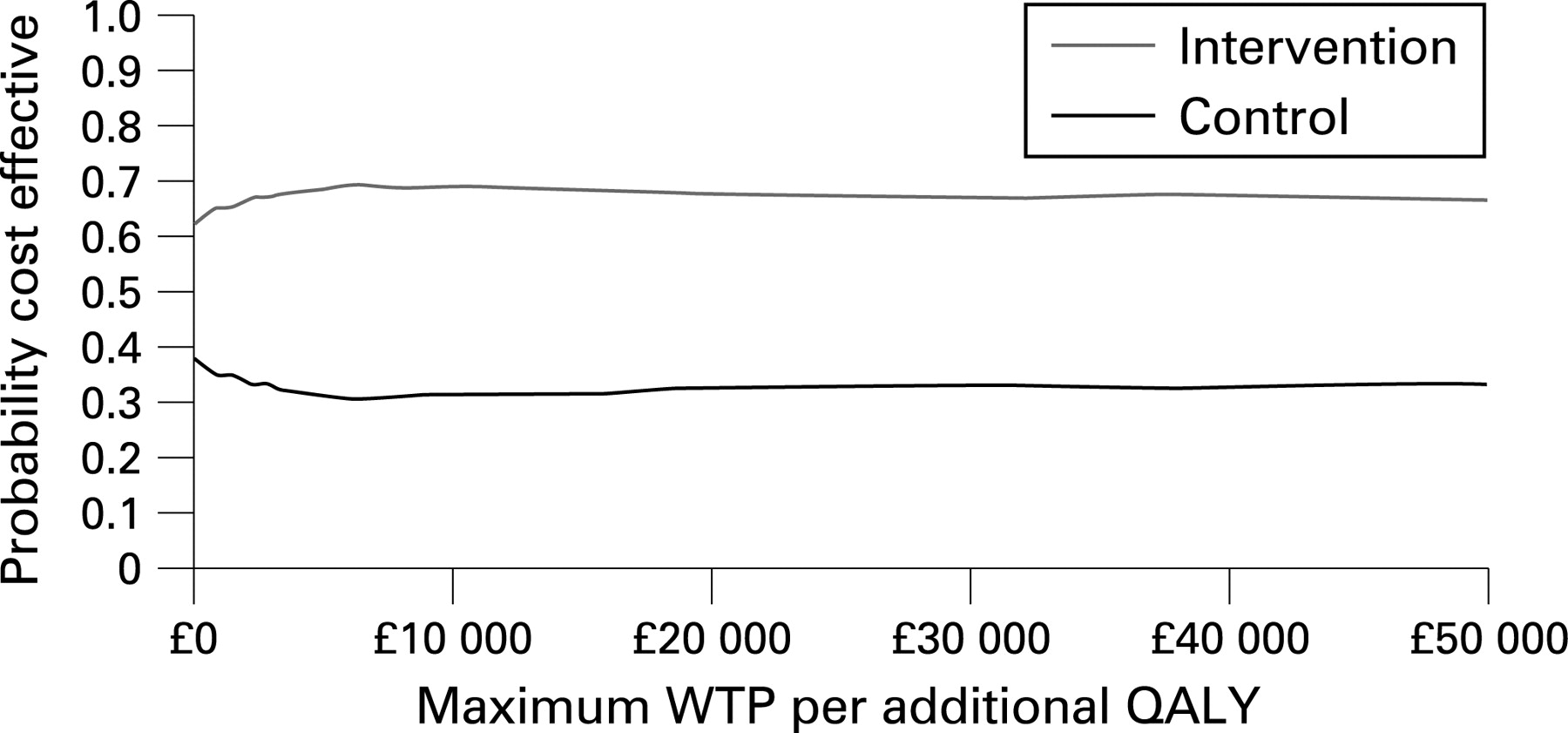
It is often the case that economic data are skewed. To estimate more reliable confidence intervals we used bootstrapping techniques.28 This approach allowed the generation of bootstrapped confidence intervals for QALY gains and health service utilisation costs. We then calculated the incremental cost-effectiveness ratio by dividing the net cost of the different interventions by the QALY gain. We estimated the sampling distribution of this ratio from the 1000 bootstrapped samples and derived a cost-effectiveness acceptability curve. This curve plots the resulting probability that the intervention is better than usual care against the maximum that decision makers would be willing to pay for an additional QALY.28
RESULTS
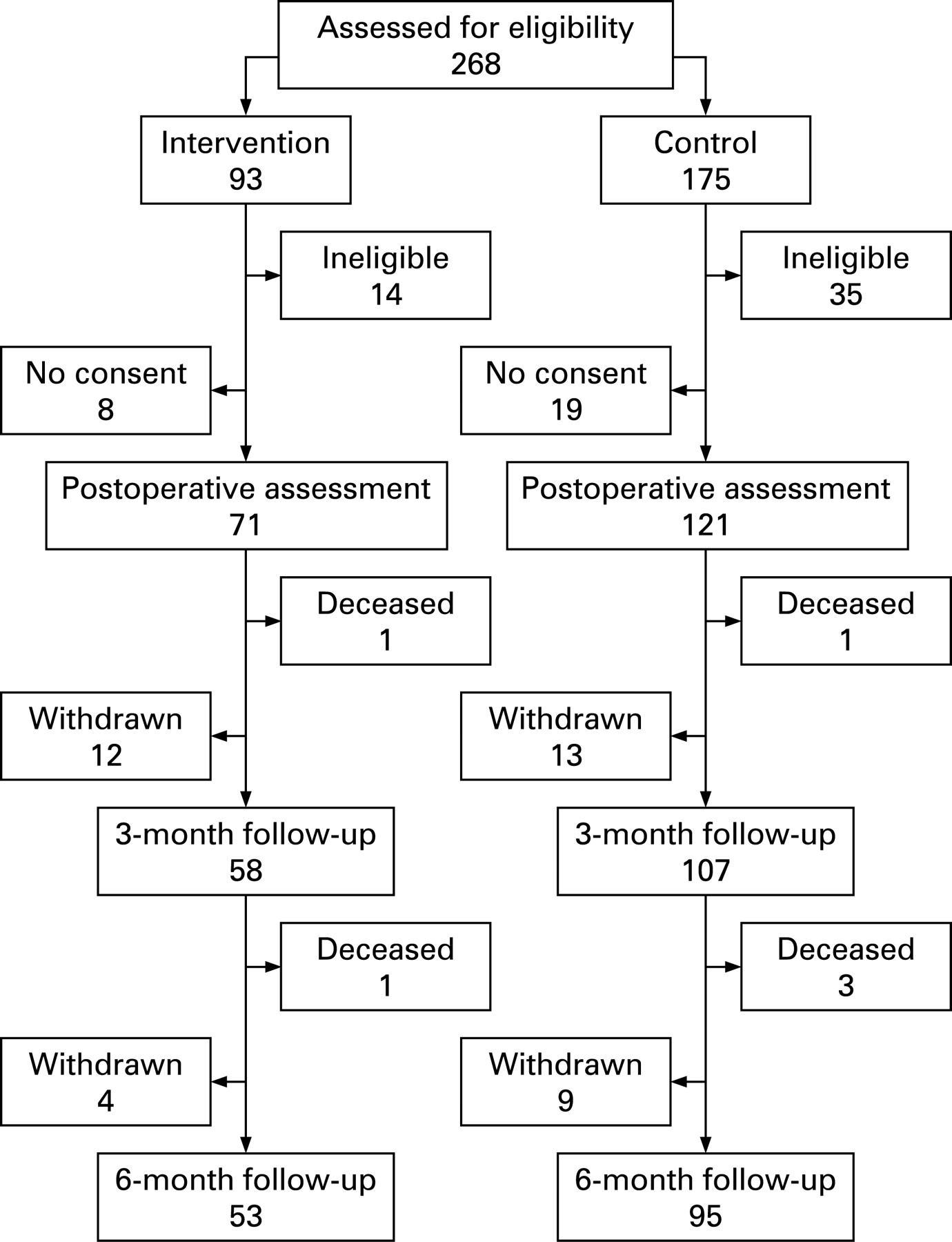
Eight centres geographically distributed across the UK were eligible and willing to take part in the study and these centres were randomised to either control or intervention (four control and four intervention). A total of 268 patients were approached to take part. Of these 43 were ineligible for participation: life-threatening comorbidity (11); previous ICD implantation (10); awaiting coronary artery bypass grafting or transplantation (8); considered medically unstable (4); exercise-induced arrhythmias (3); diagnosis of angina pectoris (3); history of mental illness (2), aged <18 years (2) and 33 eligible patients refused to consent. Of the 192 who were eligible and consented, 71 were from intervention centres and 121 from control centres. The differential ratio between the intervention and control has a minor impact on the power of the study. At 6 months, 148 (77%) were followed up, 38 participants withdrew and six died during the follow-up period. There was no significant differential follow-up between the groups. Figure 1 shows a full consort diagram for the study.
No significant differences in demographic, clinical or outcome variables were seen between the groups at baseline. Table 1 reports the baseline differences.
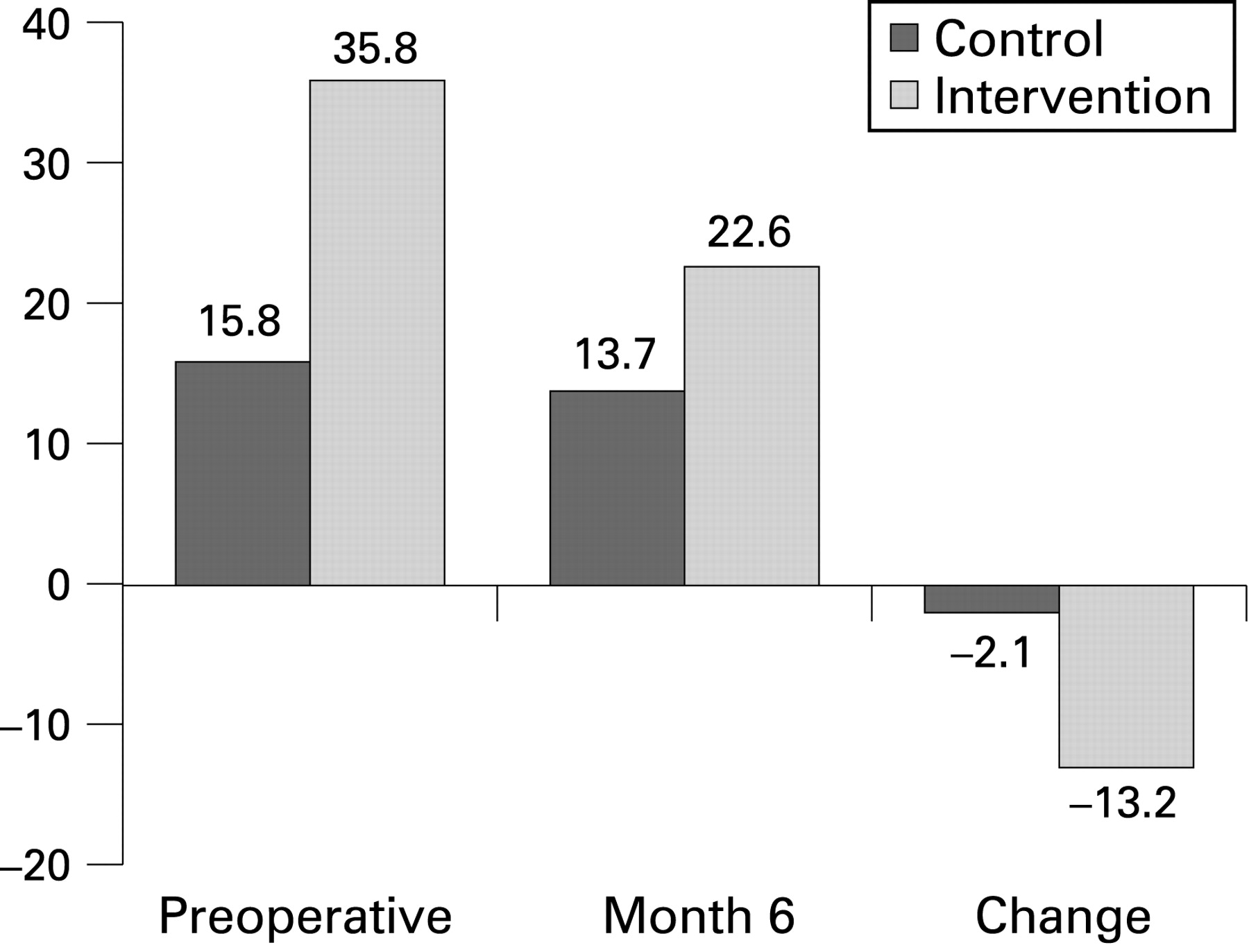
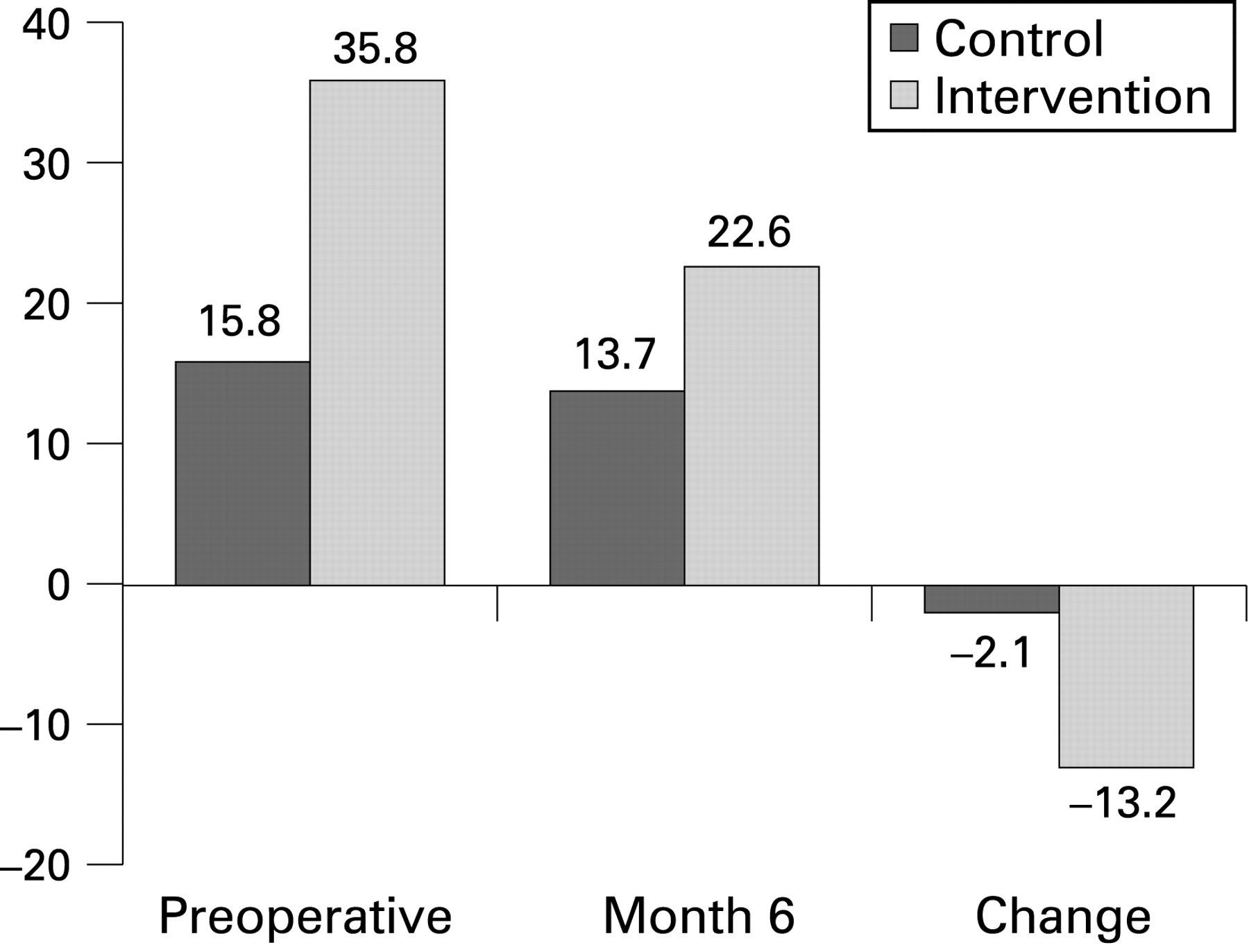
Table 2 reports the outcomes at 6 months. Comorbid anxiety and depression was examined using logistic regression at 6 months. A greater reduction in the proportion with comorbid depression was seen in the intervention group than in the control group 6 months after implantation: −13.2% versus −2.1% (fig 2). A similar pattern was seen with respect to comorbid anxiety at 6 months: −20.8% versus −12.8% (fig 3).

Significant differences at the 0.05 confidence level favouring the intervention group were seen for the physical component of the SF-12 (mean difference 3.58; 95% CI 1.62 to 5.54) and the physical limitations subscale of the SAQ (mean difference 2.30; 95% CI 0.11 to 4.71). No significant difference was seen for the mental component of the SF-12 (mean difference −2.90 (95% CI −6.77 to 0.95). To confirm whether these differences were due to the intervention or any potential centre effect, multilevel modelling was conducted to take into account the clustered nature of participants within centres (table 3). Both the physical component of the SF-12 (mean difference 3.08; 95% CI 1.13 to 5.04) and the physical limitations subscale of the SAQ (mean difference 2.22; 95% CI 0.11 to 7.22) remained significant at the 0.05 level.
The number of patients who had ICD shocks in the 6 months after implantation was similar for both groups (9.5% intervention, 13.1% control). Differences in the number of ICD shocks for each group were not significant (p = 0.53). The number of patients who had ICD storms in the 6 months after implantation was similar for both groups (1.6% intervention, 4.8% control). Differences in the number of storms for each group were not significant (p = 0.66).
Treatment costs
The total training cost for each nurse was calculated using 2002–3 prices26 as staff, premises and equipment costs for a 4 h training session as £80. As a pragmatic study this cost was distributed as a cost per patient across all patients who could receive an intervention in a 30 month period before refresher training was necessary, a conservative estimate of 150 patients. The training cost for each patient was estimated as £0.53.
Intervention costs included the time taken by the nurse to explain the booklets, estimated as 20 min (£6.67), and three telephone calls to the patient after discharge estimated at 15 min each, a total cost of £14.85, the costs of producing all booklets (£4.32) and the cost of a relaxation CD (£0.40). An additional £0.76 was added to cover the costs of warehousing, packing and distribution of the intervention packs. The total additional cost of the intervention over control including training was estimated as £12.15 per patient, a total of £12.68 including costs associated with training.
Health service resource costs
Health service resource costs consumed by both groups were similar 6 months after implantation, £486 for the intervention group and £528 for the control group. Primary care costs were similar between the groups, £75 for the intervention group and £73 for the control group. Large, but not significant cost differences were seen for outpatient appointments (£302 vs £220: intervention vs control) and inpatient costs (£101 vs £230). Table 4 gives details of unit costs and costs associated with each group.
Cost-effectiveness analysis
Combining the net costs associated with the intervention and the net utility gain yields an incremental cost-effectiveness ratio of −£1429 (marginal cost of −£13.49 divided by a marginal utility gain of 0.0094) relative to the usual care group.
Bootstrapping generated 1000 different artificial samples to characterise the distribution of health outcomes and net costs between the two groups. In 666 samples the intervention was more effective in generating QALYs and less costly, whereas in the remaining 334 samples, usual care was more effective in generating QALYs and less costly. In essence, in 66% of samples the intervention was the favoured approach for both QALY gain and cost.
The cost-effectiveness acceptability curve (fig 4) plots the resulting probability that the intervention is more cost effective than usual care against the amount decision makers may be willing to pay. The curve indicates that at all values decision makers may be willing to pay for an additional QALY, the intervention dominates usual care. If decision makers value a QALY at £30 000 (a value consistent with previous recommendations made by the National Institute of Health and Clinical Excellence in the UK) then the intervention has a 67% probability of being more cost effective than usual care.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
We have conducted a rigorously designed pragmatic cluster randomised controlled trial to assess the effectiveness and cost effectiveness of augmenting usual care with a home-based, self-management rehabilitation programme. The results demonstrate that intervention significantly improved physical aspects of quality of life, reduced physical limitations and reduced the number of unplanned emergency admissions in the 6 months after implantation. The intervention also resulted in fewer cases of anxiety and depression 6 months after implantation. These findings concur with the few other studies of cardiac rehabilitation or cognitive behavioural interventions with ICD patients.14 15 29–32 They are strikingly similar to our previous trials of cognitive behavioural home-based rehabilitation in other groups of cardiac patients. For example, the first randomised controlled trial of the Heart Manual, a self-help rehabilitation programme for post-myocardial infarction, was against routine care and reduced the incidence of anxiety and depression, improved quality of life and reduced readmissions by 30% over the next 6 months.16
As the majority of ICD patients have coronary artery disease there is an additional need to learn about the illness and be helped to manage it through lifestyle change, adherence to secondary prevention regimens and increasing activity levels. There are compelling reasons to believe that these patients would benefit from taking part in cardiac rehabilitation33 and there is some experimental evidence to support the use of a rehabilitation programme in this context.29–32 Unfortunately, in the UK, only a few patients do take part in cardiac rehabilitation. To find out why we surveyed, in 2002, three key health professionals at 39 implantation centres listed by the UK National Pacemaker Database. The majority of respondents (74%) believed they were not meeting their patients’ need for rehabilitation and the most commonly given reasons were limited access to multidisciplinary staff; a wide geographical catchment area; patients having transport difficulties; time and other administrative and organisational difficulties. The respondents supported the idea of a home-based programme such as that reported here.
Study limitations
It might be argued that patients in the intervention group had more attention directed towards them and more “gifts” in the form of written materials and a relaxation CD or tape. It might be that the self-reported improvements in psychological status and health-related quality of life simply reflect a non-specific effect of more attention. The dramatic reduction in unplanned admissions provide a “harder” outcome measure and support the idea that these differences observed represent true differences because use of medical resource is known to be driven by unmet psychological needs.34 In addition it is unlikely that greater activity levels would arise simply from more attention or gratitude.
For pragmatic reasons, to avoid overloading NHS staff and patients, we did not examine the effect of the intervention on secondary prevention or health behaviour other than activity levels. Future research might usefully examine this and it might also compare the intervention with other ways of delivering the same help. However, in view of the very similar results from other manualised self-help programmes for other cardiac patient groups and the current lack of other rehabilitation facilities or psychological support for ICD patients, the implementation should not be delayed until such trials are conducted and analysed. Experience suggests that subsequent trials will produce similar results.
From the perspective of the economic component of this study we could have chosen a broader perspective for our analysis, taking into account the costs accrued by patients and society in general. Our decision to focus on health service costs was based upon informing the decision maker and the desire to limit the response burden on patients.
CONCLUSIONS
The ICD Plan is a simple and relatively inexpensive way to meet many of the rehabilitation, educational and emotional needs of ICD patients. It was cost effective in comparison with usual care for patients undergoing ICD implantation at all values associated with a decision maker’s willingness to pay for an additional QALY. The intervention is associated with improved physical health, reduced physical limitations and reductions in anxiety and depression. It can overcome barriers to providing a rehabilitation service such as travelling restrictions and lack of a multidisciplinary staff that were disclosed in a survey of ICD implanting centres.19 It could be adopted quickly across the NHS at relatively low cost and, by reducing the number of unplanned admissions, its use might improve the cost efficacy of the use of ICDs.8
Acknowledgments
We acknowledge the contribution made by the participating collaborating centres (table 5).
REFERENCES
Footnotes
Funding: The study was funded in full by an educational grant provided by Medtronic UK.
Competing interests: Declared. GK has received funding for research projects and invited talks from Medtronic UK.
Ethics approval: Ethical approval by London MREC Ref: MREC/03/2/053.