Article Text

Abstract
Objectives To examine recent trends in first and recurrent ischaemic heart disease (IHD) deaths and hospitalisations.
Methods Using anonymous patient-linkage of routinely collected data, all New Zealanders aged 35–84 years who experienced an International Statistical Classification of Diseases and Related Health Problems I(CD)-coded IHD hospitalisation and/or IHD death between 1 January 2005 and 31 December 2015 were identified. A 10-year look-back period was used to differentiate those experiencing first from recurrent events. Age-standardised hospitalisation and mortality rates were calculated for each calendar year and trends compared by sex and age.
Results 160 109 people experienced at least one IHD event (259 678 hospitalisations and 35 548 deaths) over the 11-year study period, and there was a steady decline in numbers (from almost 24 000 in 2005 to just over 16 000 in 2015) and in age-standardised rates each year. With the exception of deaths in younger (35–64 years) women with prior IHD, there was a significant decline in IHD events in men and women of all ages, with and without a history of IHD. The decline in IHD mortality was greater for those experiencing a first rather than recurrent IHD event (3.8%–5.2% vs 0%–3.7% annually on average). In contrast, the decline in IHD hospitalisations was greater for those experiencing a recurrent compared with a first IHD event (5.6%–7.3% vs 3.2%–5.7% annually on average).
Conclusions The substantial decline in IHD hospitalisations and mortality observed in New Zealanders with and without prior IHD between 2005 and 2015 suggests that primary and secondary prevention efforts have been effective in reducing the occurrence of IHD events.
- Coronary artery disease
- Acute myocardial infarction
- Acute coronary syndromes
- Epidemiology
Statistics from Altmetric.com
Introduction
Steady declines in deaths from ischaemic heart disease (IHD)1–3 have been noted in most high-income countries for many years. Trends in hospitalised IHD, by contrast, have been more variable, with some countries reporting declines and others a plateau.4–9 In New Zealand, IHD death rates have declined by approximately 90% since the late 1960s.10 IHD hospitalisation rates reached a peak in the late 1990s, before declining through the early 2000s.11 Trends in IHD hospitalisations have not been examined in New Zealand since 2005,1 and there are limited data on whether mortality and hospitalisation trends differ by sex and for first and recurrent events.
Over the past two decades, there have been important changes in the clinical classification and diagnosis of IHD that may have affected the pattern of IHD hospitalisations. These changes include refining the definition of myocardial infarction (MI),12 the use of ‘acute coronary syndrome’ (ACS) as the main way of classifying major acute IHD events and an increased availability of more sensitive cardiac biomarkers, particularly troponins.13 Such changes would be expected to increase the diagnosis of MIs that may have previously gone undetected. In addition, the evidence-based management of IHD has improved, including the more frequent use of primary percutaneous coronary intervention (PCI) for acute reperfusion therapy and more systematic prescribing of antiplatelet, antihypertensive and statin medications.14 These changes would be expected to improve outcomes, including recurrent hospitalisations and deaths, for those with existing IHD.
Measuring trends in IHD incidence is important to define the burden of cardiovascular disease and identify high-risk populations, assess the success of primary prevention efforts and generate useful information for updating priorities regarding health promotion.15 Furthermore, in an era of ageing populations,16 improved survival2 and increasing IHD prevalence,17 it is also important to examine changes in recurrent IHD events to assess the likely impact of secondary prevention and treatment.18 However, very few studies have included people with previous IHD,7 19 and none have examined recurrent trends in both deaths and hospitalisations at a national level.
In New Zealand, every person who has had contact with the national health system (>98% of the population)20 has a unique identifier (a National Health Index number), which enables individual linkage of multiple national routinely collected datasets, including hospitalisations and mortality. The objectives of this study were to use this data-linkage process to: (1) examine recent trends in first and recurrent IHD deaths and hospitalisations and (2) investigate whether these trends differ by age and sex.
Methods
The study population included all New Zealand residents aged 35–84 years for the period 2005–2015. Over this time period, the New Zealand population in this age group increased from approximately 2.05 to 2.35 million and the proportion of people aged 65–84 years increased from 21.6% to 25.4%.
Numerators and denominators for the calculation of hospitalisation and mortality rates were obtained using data from the National Minimum Dataset, a national collection of ICD-10-coded public hospital admission and discharge information,21 and the Mortality Collection, a national dataset classifying the underlying cause of death for all deaths registered in New Zealand.22 Both datasets used version ICD-10-AM (International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification).
Denominators for recurrent events included all people alive at the beginning of each study year who had been hospitalised with a primary or secondary diagnosis of IHD (ICD-10 codes I20–I25) in the preceding 10 years. These were estimated for each year (2005–2015) by identifying all people in the National Minimum Dataset who had been admitted with an IHD diagnosis in the 10 years prior to the study year, and linking individuals to mortality data to ensure they were still alive on 1 January of that year. As data were individually linked, accurate estimates of the denominator population by age and sex were available. Denominators for first IHD events comprised all individuals without an IHD hospitalisation in the previous 10 years and were calculated by subtracting denominators for recurrent events from the New Zealand population projections for each calendar year (obtained from the Ministry of Health and Statistics New Zealand) during the study period.
Numerators for hospitalisation rates included people from the denominator populations who were acutely admitted to a public hospital with a primary diagnosis of IHD between 1 January and 31 December of the study year. This was a per-person-per-year, rather than a per-event, analysis, so even if someone was hospitalised multiple times during the year, he or she contributed to the numerator once for that year. If a person without prior IHD was admitted multiple times in a study year, his or her events were counted as a single first event, as he or she would have been included in the ‘first events denominator’ for that year. In subsequent years, that person would then be moved to the ‘recurrent events denominator’. The subgroup of people hospitalised with MI specifically (ICD-10 codes I21 and I22) was also recorded. Privately funded hospitalisation data were not complete and therefore not included in these analyses; however, based on reported data, privately funded admissions represent fewer than 3% of all IHD hospitalisations in New Zealand,23 with most coded as chronic IHD and admitted electively for non-acute procedures.11
Numerators for mortality rates included all people with an ICD-10 coded underlying cause of death of IHD. If a person experienced both an IHD hospitalisation and a subsequent IHD death in the same year, both events were counted in the calculation of hospitalisation and death rates.
Statistical analysis
Characteristics of people who experienced an IHD event during 2005 and 2015 were examined, and characteristics of those with and without prior IHD compared using descriptive statistics. Differences between the two groups and 95% CIs for both years were examined using a two-sample test of equality of proportions (with continuity correction) using the normal approximation to the binomial distribution.
MI and IHD hospitalisation and IHD mortality rates were calculated per 100 000 population for those with and without prior IHD for each calendar year. Age-specific rates were calculated for three age groups: 35–64, 65–74, 75–84 years. Crude rates were age standardised, using these three age groups, to the Projected New Zealand Population 2015 (35–84 years) by the direct method (table 1). Age-standardised rates were calculated by sex.
Standard population used for age standardisation
Temporal trends in IHD-specific hospitalisation and mortality rates by sex and age group were examined for first and recurrent events using negative binomial regression, with year of admission (continuous variable) and 5-year age group (categorical variable) included as independent variables. Interactions between year and age group were tested for, but there was no evidence for an interaction effect. The results of the final models were summarised by presenting the incidence rate ratio (IRR) changes, interpreted as age-adjusted annual per cent changes in hospitalisation rates over the study period. IRRs were calculated by taking the exponential of the beta coefficient for year of admission and the IRR changes were calculated using the formula (IRR−1) × 100%. Data analysis was performed using Stata SE statistical software V.13.0.24
Ethical approval
This analysis is part of the VIEW research programme, which receives annual ethical reapprovals from the Northern Region Ethics committee Y (original approval in 2003 (AKY/03/12/314)) and the Multi-Region Ethics Committee (original approvals in 2007 (MEC/01/19/EXP) and 2011 (MEC/11/EXP/078)). Individual patient consent is not required as all data are anonymised.
Results
Between 2005 and 2015, 160 109 New Zealand residents aged 35–84 years were admitted to hospital 259 678 times for IHD and there were 35 548 IHD deaths. Patient characteristics at first event (IHD hospitalisation or death) for the years 2005 and 2015 are shown in table 2.
Characteristics of people who experienced an IHD event in 2005 and 2015, by IHD history
Despite continuous growth in the New Zealand population from 2005 to 2015, the number of people who died or were hospitalised with IHD steadily declined each year (from almost 24 000 in 2005 to just over 16 000 in 2015). Declines over time were also noted in the proportion of people experiencing an IHD event who had prior IHD (from 50% in 2005 to 38% in 2015) and who were female (from 40% in 2005 to 34% in 2015). Among people hospitalised with IHD, about two-thirds of those without a history of IHD were diagnosed with MI, compared with only half of those with prior IHD.
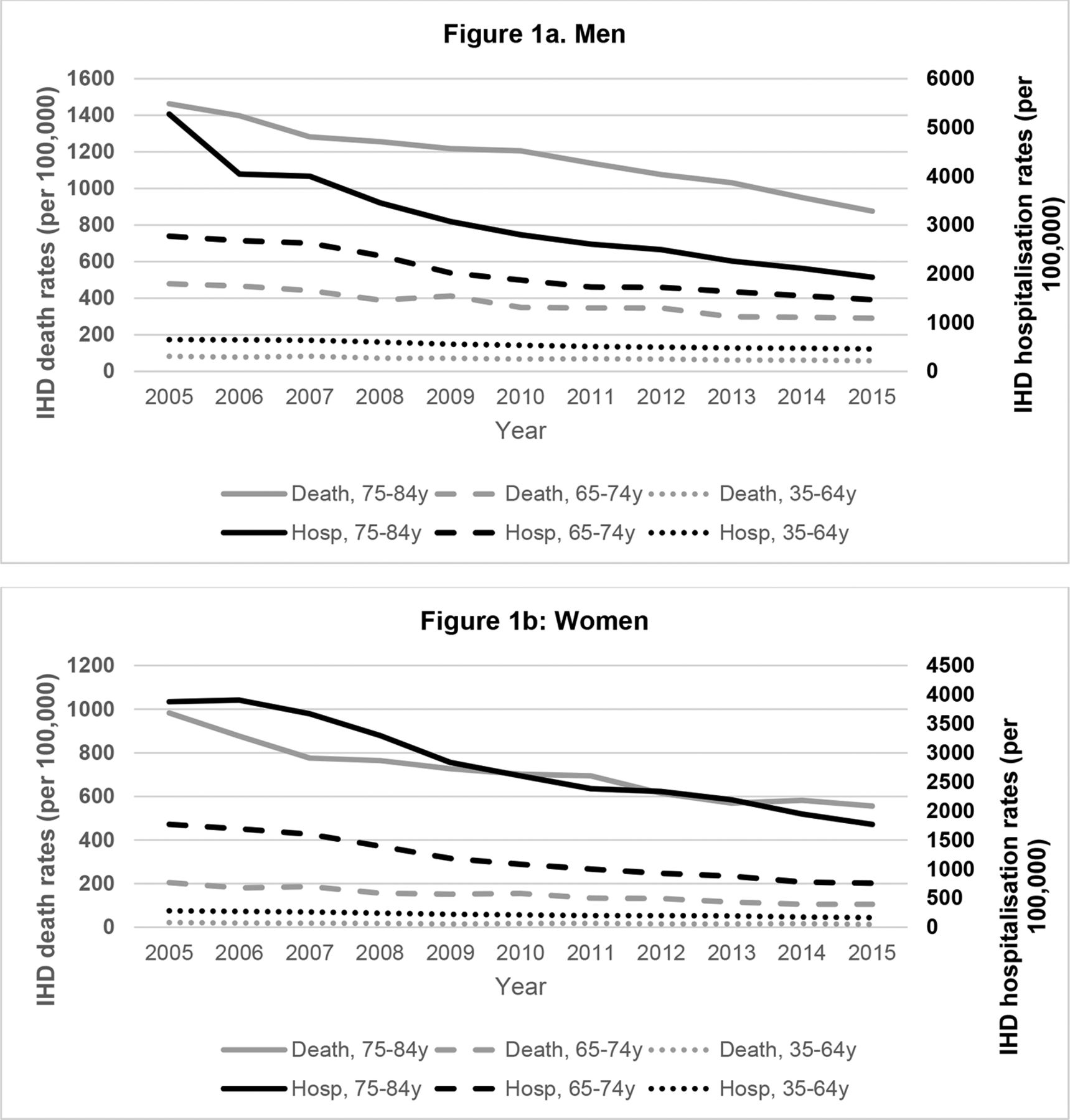
Declining hospitalisation and death rates were observed in all age groups, as shown in figure 1A,B.
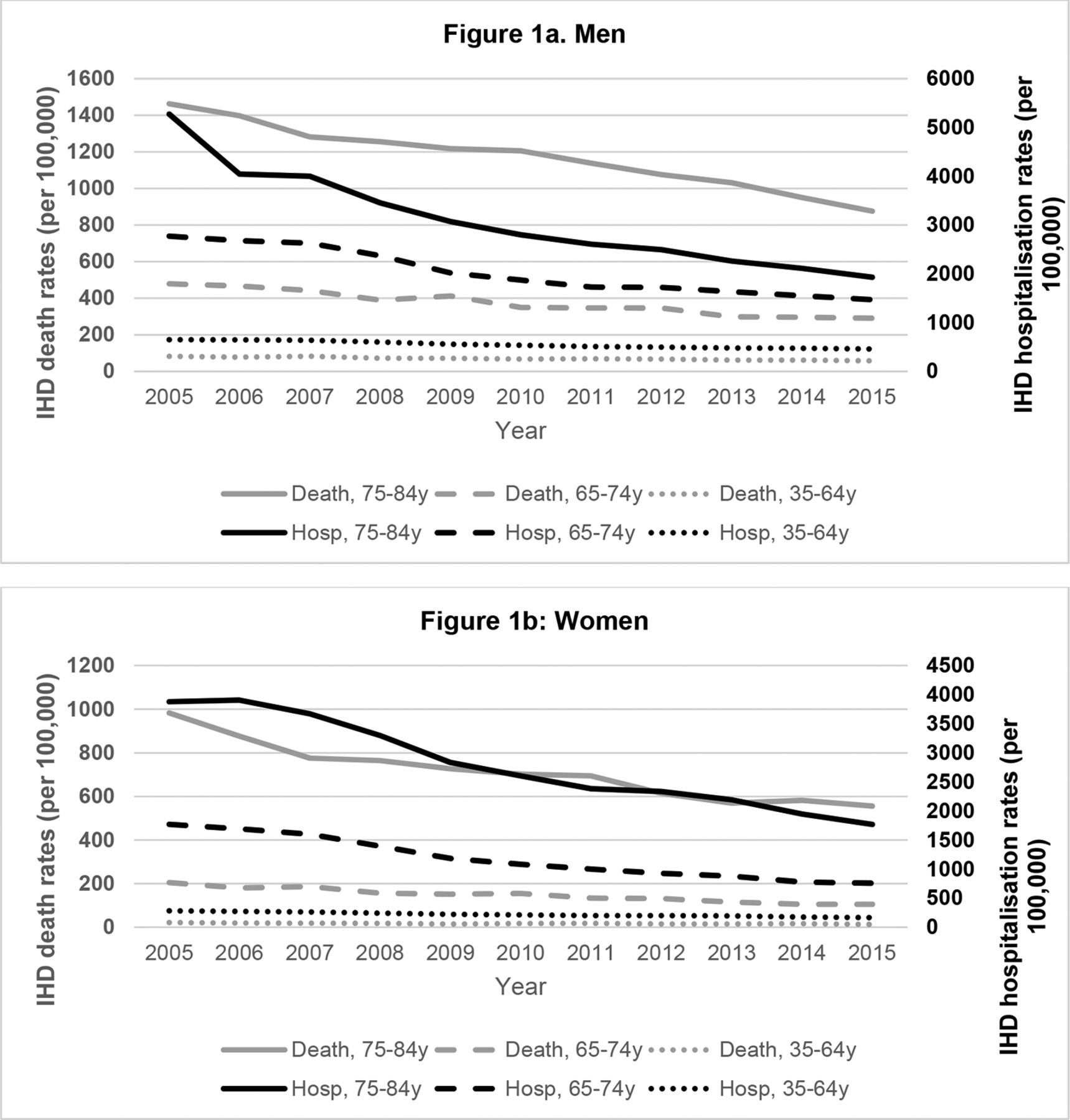
Age-specific IHD death (left axis) and hospitalisation (right axis) rates for men (A) and women (B), 2005–2015. IHD, ischaemic heart disease.
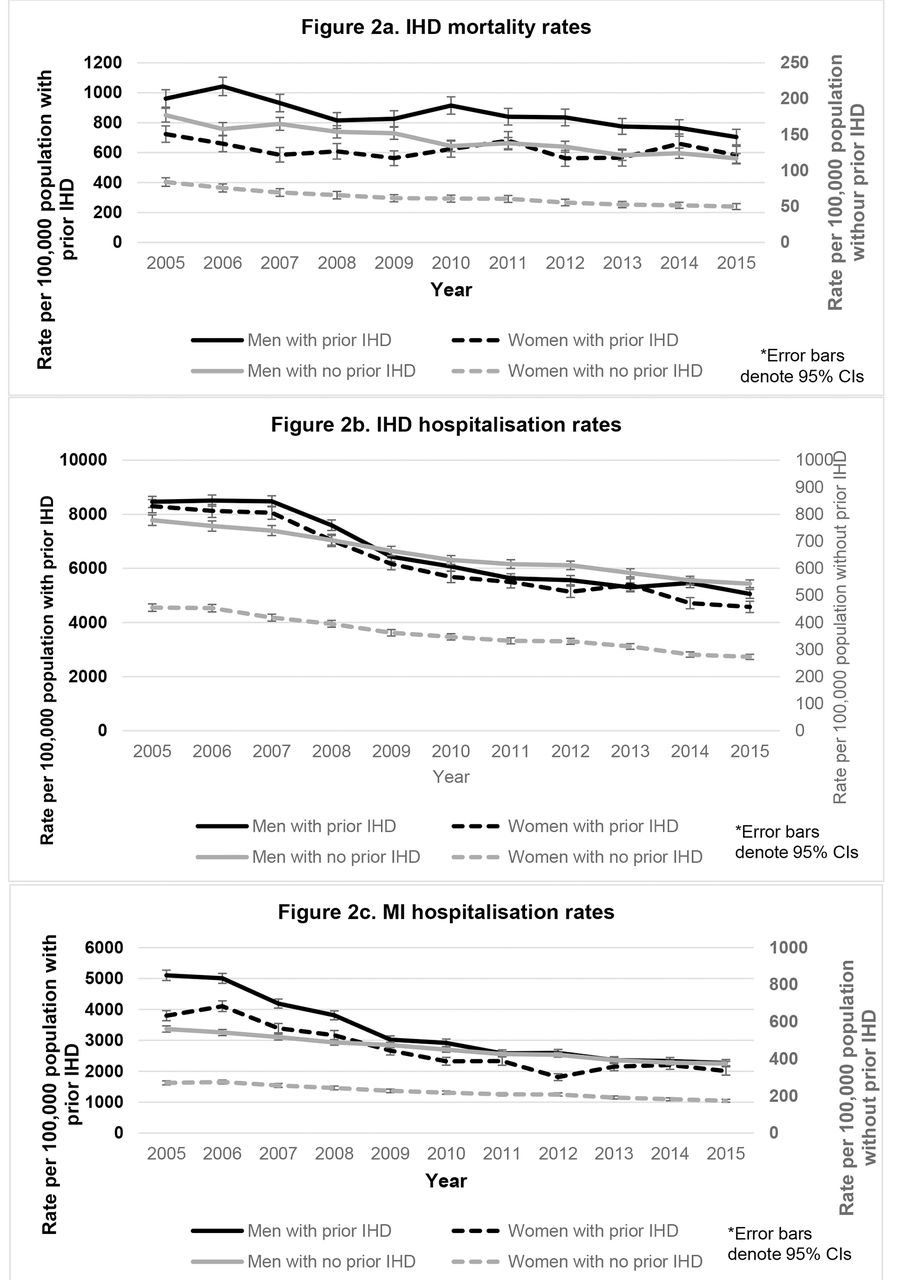
Age-standardised IHD and MI rates in both men and women with and without prior IHD also declined, as shown in figure 2A–C. Men and women with a history of IHD had substantially higher IHD rates than those without prior IHD (rates were approximately fivefold higher for deaths and 10-fold higher for hospitalisations). Men with and without prior IHD had higher mortality rates than their female counterparts. Likewise, men without prior IHD had much higher hospitalisation rates than women without prior IHD. However, there were no sex differences in IHD hospitalisation rates, and from 2009, MI hospitalisation rates, in people with a history of IHD.
{kind=link}
{kind=link}
Age-standardised IHD mortality (A), IHD hospitalisation (B) and MI hospitalisation (C) rates in men and women with (left axis) and without (right axis) a history of IHD. IHD, ischaemic heart disease; MI, myocardial infarction.
Table 3 shows age-adjusted annual per cent changes in IHD deaths and hospitalisations by sex, IHD history and age group. Declines in IHD deaths were greater in men and women without prior IHD (3.8%–5.0% and 4.8%–5.2%, respectively) compared with those with prior IHD (2.9%–3.4% for men and 0%–3.7% for women). Younger (35–64 years) women with prior IHD had low IHD death rates and were the only group who did not experience a decline in mortality over the study period. By contrast, declines in IHD hospitalisations were greater in men and women with prior IHD (5.6%–6.6% and 5.9%–7.3%, respectively) than those experiencing first hospitalisations (3.2%–4.8% in men and 4.3%–5.7% in women).
Age-adjusted annual percent changes in IHD hospitalisations and deaths for men and women with (recurrent) and without (first) prior IHD, by age group
Discussion
As far as we are aware, this is the first study to compare trends in IHD event rates in those with and without a history of IHD at a national level. Our analyses have demonstrated a continued decline in IHD event rates (both hospitalisations and deaths) in New Zealand in recent times. With the exception of deaths in younger (35–64 years) women with prior IHD, there was a significant downward trend in IHD and MI events in men and women of all ages, with and without a history of IHD. The decline in IHD mortality was greater for those experiencing a first IHD event (4%–5% annually, compared with 2%–3% for those with prior IHD), but the decline in hospitalisations was greater for those experiencing a recurrent event (6%–7% annually, compared with 4%–5% for those experiencing a first event).
Our findings are consistent with recent studies that have noted steady declines in first MI hospitalisations in Denmark5 and USA,6 total ACS hospitalisations in Ireland,4 first and recurrent IHD hospitalisations in Western Australia25 and IHD mortality in most high-income countries.2 3 By contrast, stable, rather than decreasing, IHD hospitalisation trends have been reported in Hong Kong8 and British Columbia,9 and increasing IHD mortality rates in South and East Asia.3 The continued decline in IHD mortality in most high-income countries has been attributed to a combination of improved primary (improvements in risk factors) and secondary (improved treatment of acute and chronic IHD) prevention.26 27 Using the IMPACT Coronary Heart Disease Model, Ford et al estimated that 47% of the decline in IHD mortality in USA from 1980 to 2000 was attributable to evidence-based medical and surgical treatments and 44% to reductions in major risk factors.27
IHD mortality rates in New Zealand have steadily declined since the late 1960s. In 2015, IHD mortality rates for men and women with prior IHD were six and 12 times higher, respectively, than men and women without an IHD history. After an IHD event, the risk of experiencing a recurrent event is high: a recent national Swedish registry study found that one in five patients discharged with MI had a subsequent event (stroke, MI or cardiovascular death) in the first 365 days after the index MI; more than half of these events were deaths. For patients with MI who survived a year without a subsequent cardiovascular event, one in five patients experienced an event during the subsequent 2 years.28 In the Swedish registry study, the risk of experiencing a subsequent event was highest in elderly patients, those with heart failure and those who had not received revascularisation.
Our analyses started in 2005, as a previous New Zealand study had examined IHD hospitalisation trends up to 2005.11 We have confirmed a continued decline in total IHD hospitalisations and have shown that the rate of decline is now greater for recurrent, compared with first, hospitalisations. Over the study period, the proportion of people hospitalised with IHD who had an IHD history decreased from 50% to 38%. This proportion is similar to that reported in Australia (40%),29 but significantly higher than in European countries such as the Netherlands (21%)30 and UK (17%).31 This downward trend suggests that hospital and primary care-based interventions to prevent recurrent IHD events are having an important impact on hospitalisation rates. Improvements in management include long-term treatment with more systematic and intensive secondary prevention medications, greater utilisation of early intervention strategies in ACS, primary PCI for ST elevation MI and other secondary prevention measures such as cardiac rehabilitation, smoking cessation, promotion of a cardioprotective diet and an increase in physical activity.14
Strengths and limitations
The ability to accurately link multiple national health data bases in New Zealand using a unique health identifier is a significant strength of our study. Linkage of routinely collected datasets enabled us to determine the denominators for recurrent and first events with more accuracy than has previously been possible. Our decision to examine total IHD, as well as MI, hospitalisations also meant that we were able to obtain a more complete picture of coronary trends, as ‘other IHD types’ (mostly angina) comprise a sizeable proportion (over one-third) of IHD admissions. The use of routinely collected data for these analyses enabled us to capture nearly all IHD hospitalisations over the study period, as private hospitals are responsible for very few IHD admissions in New Zealand,23 and the National Minimum Dataset is considered complete for public hospitalisation data.
However, there are several potential study limitations. First, our analyses are unlikely to have captured all non-fatal IHD events, as some people will be undiagnosed or have been treated in the community. This is likely to have been more of an issue for angina or ‘other IHD’ subtypes, as patients diagnosed with ACS, particularly MI, are seldom treated out of hospital in New Zealand.11 Second, IHD hospitalisations and deaths were identified using ICD-10 codes extracted from national hospitalisation and mortality datasets, so the study is reliant on the accuracy and validity of these data. Studies from several European countries have reported high sensitivity and positive predictive values for ICD-coded IHD events in national datasets,32 but there are no published validation studies over a contemporary period in New Zealand. Our group have compared ACS diagnoses in hospitalisation data with a clinical registry and found 95% agreement (unpublished data). Some misclassification or miscoding of non-cardiac chest pain or other non-IHD diagnoses is possible. While we are unaware of any major changes in coding standards or directives over the course of the study period, this may also have impacted on the trends observed. Finally, because we only had hospitalisation data from 1993 onwards, we chose to use a 10-year look-back period across all events to distinguish first from recurrent IHD hospitalisations. While a 10-year look-back period is often used and has been considered a gold standard,33 it will have resulted in a small proportion of recurrent hospitalisations (where previous events occurred >10 years prior) being misclassified as first events.
In conclusion, favourable IHD hospitalisation and mortality trends were observed in men and women, with and without prior IHD, in most age groups in New Zealand between 2005 and 2015, indicating that both primary and secondary prevention efforts have been effective. Declines in hospitalisation rates were greatest in people with a history of IHD, but declines in mortality were greatest in those experiencing a first event.
Key messages
What is already known on this subject?
Total ischaemic heart disease (IHD) mortality has fallen significantly over the past few decades. Studies in Western countries have also reported decreasing rates of IHD hospitalisations, but have generally not distinguished between IHD events occurring in those with and without a history of IHD. The extent to which IHD deaths and hospitalisations are falling in those experiencing first versus recurrent events is therefore unknown.
What might this study add?
Between 2005 and 2015, there were significant declines in both IHD deaths and hospitalisations in men and women with and without prior IHD in New Zealand. These declines were observed in all age groups, with the exception of deaths in younger (35–64 years) women. Declines in IHD mortality were greater for those experiencing a first IHD event (4%–5% annually, compared with 2%–3% for those with prior IHD), but declines in IHD hospitalisations were greater for those experiencing a recurrent event (6%–7% annually, compared with 4%–5% for those without prior IHD).
How might this impact on clinical practice?
The sustained decline in IHD deaths and hospitalisations for those with and without prior IHD indicates that both primary and secondary prevention efforts, including the increased use of secondary prevention medication and revascularisation following an acute coronary syndrome, have been effective and need to continue in New Zealand.
Acknowledgments
The authors would like to thank the New Zealand Health Board for enabling use of the data and Arier Lee for providing additional statistical advice.
References
Footnotes
Contributors CG, RJ and AJK designed the study. CG, KP and BW acquired the data. CG analysed the data and all authors interpreted the data. CG drafted the work and all authors revised it critically for important intellectual content. All authors approved of the version to be published. All authors, external and internal, had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This research project has been supported by the Health Research Council (grant number 11/800). This research was supported by Health Research Council Clinical Research Training Fellowship (grant number 11/814) and a National Heart Foundation Research Fellowship (grant number 3709384). Researchers are independent from funders. The study funders/sponsors had no role in the study design, collection, analysis or interpretation of data.
Competing interests All authors have completed the Unified Competing Interest format at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that HW has had grants from Sanofi Aventis, Eli Lilly, National Institute of Health, Merck Sharpe & Dohm, AstraZeneca, GlaxoSmithKline, Omthera Pharmaceuticals, Pfizer New Zealand, Intarcia Therapeutics, Elsai, DalGen Products and Services, Daiichi Sankyo Pharma Development for research outside the submitted work. SW has received a grant from Roche Pharmaceuticals for research outside the submitted work. CG, RJ, WCC, KP, BW and AJK have no conflicts of interest to declare.
Ethics approval Multi-Region Ethics Committee; Northern Region Ethics Committee Y.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Technical appendix, statistical code and dataset available on request from the corresponding author at c.grey@auckland.ac.nz. Consent was not obtained but the presented data are anonymised and risk of identification is minimal. Applications will only be granted and data provided after agreement from our contributing providers and the Ministry of Health and after ethical approval by the New Zealand Multi-Region Ethics Committee.
Correction notice This paper has been amended since it was published Online First. Figure 2 was duplicated as figure 1. We have replaced this with the correct figure 1. Also, the authors have discovered that in table 2 in the row IHD death there was a minor error with the data. This has been changed and the author point out that this doesn’t affect any other parts of the paper, the findings or conclusions.