Article Text

Abstract
Objective The aim of this study was to determine the effect of polypill-based care on the achievement of 2016 European Society of Cardiology (ESC) guideline targets for blood pressure (BP), low-density lipoprotein (LDL) cholesterol and antiplatelet therapy.
Methods We conducted an individual participant data meta-analysis of three randomised clinical trials that compared a strategy using a polypill containing aspirin, statin and antihypertensive therapy with usual care in patients with a prior cardiovascular disease (CVD) event or who were at high risk of their first event. Overall, the trials included 3140 patients from Australia, England, India, Ireland, the Netherlands and New Zealand (75% male, mean age 62 years and 76% with a prior CVD event). The primary outcome for this study was the proportion of people achieving ESC guideline targets for BP, LDL and antiplatelet therapy.
Results Those randomised to polypill-based care were more likely than those receiving usual care to achieve recommended targets for BP (62% vs 58%, risk ratio (RR) 1.08, 95% CI 1.02 to 1.15), LDL (39% vs 34%, RR 1.13, 95% CI 1.02 to 1.25) and all three targets for BP, LDL and adherence to antiplatelet therapy (the latter only applicable to those with a prior CVD event) simultaneously (24% vs 19%, RR 1.27, 95% CI 1.10 to 1.47) at 12 months. There was no difference between groups in antiplatelet adherence (96% vs 96%, RR 1.00, 95% CI 0.98 to 1.01). There was heterogeneity by baseline treatment intensity such that treatment effects increased with the fewer the number of treatments being taken at baseline: for patients taking 3, 2 and 0–1 treatment modalities the RRs for reaching all three guideline goals simultaneously were 1.10 (95% CI 0.94 to 1.30, 22% vs 20%), 1.62 (95% CI 1.09 to 2.42, 27% vs 17%) and 3.07 (95% CI 1.77 to 5.33, 35% vs 11%), respectively.
Conclusions Polypill-based therapy significantly improved the achievement of all three ESC targets for BP, LDL and antiplatelet therapy compared with usual care, particularly among those undertreated at baseline.
- cardiac risk factors and prevention
Statistics from Altmetric.com
Introduction
European Society of Cardiology (ESC) guidelines on the prevention of cardiovascular disease (CVD) recommend achievement of target blood pressure (BP) and lipid levels for people who have had a prior CVD event or who are at high risk of their first CVD event, along with antiplatelet therapy for people who have had a prior CVD event.1 A recent cross-sectional survey of European patients with established coronary heart disease (CHD) (EUROASPIRE IV) concluded that ‘therapeutic targets for risk factors are not being achieved in far too many patients’ with 43% not achieving BP and 81% not achieving lipid targets.2 Similar challenges are evident in other countries.3 The ESC guidelines recommend that all targets be met simultaneously, thus a single pill containing aspirin, statin and BP-lowering agents (a ‘polypill’) may assist by treating risk factors concurrently and enhancing uptake and adherence to guideline-recommended care. Polypill-based care has been shown to improve adherence, systolic BP and low-density lipoprotein (LDL) cholesterol compared with usual care among patients with CVD or at high risk of their first event.4 No safety concerns beyond what would be expected given the component medications have been identified.4 Some European guidelines recommend considering the use of a polypill to increase adherence to cardiovascular drug therapy.5 6 The ESC guidelines on the prevention of CVD note that one gap in the evidence regarding the use of polypills is in whom polypill-based care would be the most effective. The aim of this study was to determine whether these effects increase the proportion of patients who achieve targets recommended by the 2016 ESC guidelines on the prevention of CVD and, if so, in whom they would be most effective.
Methods
This study uses data from the Single Pill to Avert Cardiovascular Events (SPACE) collaboration individual participant data meta-analysis.7 The protocol and main results of this meta-analysis have been previously described.4 7
Contributing trials
The SPACE collaboration includes three trials conducted during 2010–2013: IMProving Adherence using Combination Therapy (IMPACT, n=513) with participants from New Zealand,8 Kanyini Guidelines Adherence with the Polypill (Kanyini-GAP, n=623) with participants from Australia9 and Use of a Multidrug Pill In Reducing cardiovascular Events (UMPIRE, n=2004) with participants from England, India, Ireland and The Netherlands.10 The three trials were planned, conducted and analysed collaboratively, and were based on the same protocol11 with minor regional adaptations.12 13 All three trials used a randomised, open label, blinded endpoint design and compared polypill-based care with usual care in individuals with established CVD or at high risk thereof. Individual participant data meta-analysis of the three trials was planned prospectively, although this current analysis was not prespecified.7
Participants
Key inclusion criteria were: (1) established atherothrombotic CVD or calculated 5-year cardiovascular risk of at least 15%14 and (2) all four components of at least one polypill version were indicated according to the participant’s physician. In the UMPIRE trial, half the participants were from India and in the IMPACT and Kanyini-GAP trials, approximately half were indigenous peoples. Recruitment was from primary care clinics (Australia, New Zealand), hospital clinics (India) or a mixture of these clinics (Europe).
Randomisation
Participants were randomised 1:1 by central computer-based randomisation to polypill-based care or to continued usual care. Randomisation was stratified by recruitment site (Kanyini-GAP and UMPIRE) or Primary Health Organisation (IMPACT), presence of CVD at baseline (all trials), indigenous status (IMPACT) and whether participants were taking full combination therapy (antiplatelet, statin and ≥2 BP-lowering agents) at baseline (IMPACT and Kanyini-GAP).
Intervention and control
Two polypills were available, both manufactured and supplied by Dr Reddy’s Laboratories, Hyderabad, India. The choice of polypill was made by the participant’s physician (within a primary care or hospital clinic), who indicated prior to randomisation the version they would use for that participant if they were randomised to the polypill group. The polypills were: polypill 1: aspirin 75 mg, simvastatin 40 mg, lisinopril 10 mg, atenolol 50 mg; polypill 2: aspirin 75 mg, simvastatin 40 mg, lisinopril 10 mg, hydrochlorothiazide 12.5 mg. Polypills were available from community pharmacies in IMPACT and Kanyini-GAP (with the usual copayment of a subsidised medication) and were dispensed for free from trial clinics in UMPIRE (due to the requirements of the approving ethics committees). Both polypill and usual care groups were managed by the participant’s physician (within primary care or hospital clinic) according to local clinical guidelines. Participants randomised to the polypill group could be prescribed additional antiplatelet, statin and BP-lowering medication on top of the polypill, at the discretion of the treating physician.
Outcomes
The primary outcomes for this analysis were whether or not 2016 ESC guideline targets1 for BP, LDL and antiplatelet therapy (separately or together) had been achieved for trial participants (table 1). Outcomes were assessed at 12 months.
2016 European Society of Cardiology1 targets for BP, LDL and antiplatelet therapy
BP was measured using calibrated automated sphygmomanometers during study visits, and all recordings were printed and logged to ensure unbiased measurement. Two models of sphygmomanometer were used (Omron T9P in IMPACT and Omron 705CPII for Kanyini GAP and UMPIRE), both of which have been validated against protocols for both the European Society of Hypertension and the British Hypertension Society. Cholesterol was measured by community laboratories blind to participation in the trial and treatment allocation.
Participants in whom aspirin or an alternative antiplatelet drug are indicated according to 2016 ESC guidelines (ie, those with established CVD) were regarded as having achieved the antiplatelet therapy treatment target if they self-reported adherence to an antiplatelet drug on at least 4 days in the preceding week. Direct measurement of antiplatelet adherence was not used in the trials because of its high cost and the intrusiveness and impracticality of this method of measurement in ambulatory care settings.15 Indirect measurement of antiplatelet adherence can be obtained through self-report, which is a practical and valid way to measure adherence in clinical practice according to a review of measures of adherence.16 Further, self-reported non-adherence has been associated with an increase in cardiovascular events in a cohort of patients with stable CHD.17 The 2016 ESC guidelines do not recommend antiplatelet therapy in patients without established CVD. Therefore, participants at high risk but without established CVD were excluded from the analysis of the antiplatelet therapy treatment target, and for the analysis of the achievement of all three guideline targets for BP, LDL and antiplatelet therapy simultaneously, only BP and LDL target achievement were considered.
Analyses
Analyses were performed on the combined SPACE Collaboration dataset using one-stage meta-analyses (ie, individual participant data were pooled, then models run on the combined dataset).18 Log-binomial regression with fixed treatment and random trial effects was used. This model was used to estimate the proportions of participants achieving targets and risk ratios (RRs) for the treatment. For comparison, we did the same analysis for the achievement of UK19–23 and US24 25 guideline targets. We interpreted significance of the effect estimates after correction of p values for multiple comparisons of the targets within each guideline using the Holm-Bonferroni method, describing corrected p<0.05 as statistically significant. Subgroup analyses were performed by adding a fixed effect for subgroup as well as a fixed interaction between the treatment effect and the subgroup of interest. Subgroups comprised the following at baseline: age group (≤62 years or >62 years, the mean age), sex, the number of medication modalities used (0, 1, 2 or 3 of antiplatelet, BP-lowering and statin therapy), use of all four indicated CVD medications (antiplatelet, statin and >2 BP-lowering medications; yes, no) and history of CVD (yes, no). Patients with missing data were excluded from the main analyses. For composite targets (ie, those based on the achievement of more than one target), patients were classified as not having achieved the target if the target had not been met for any available target, even if data were not available for all targets contributing to the composite measure. In sensitivity analyses, we described baseline characteristics according to whether data for the combined 12-month ESC target were missing, and compared the effect of polypill-based care with usual care on the achievement of 12-month ESC targets including missing data using multiple imputation. All analyses were performed using SAS V.9.2 (SAS Institute), except for the Holm-Bonferroni correction procedure which was performed in Microsoft Excel 2016.
Results
Baseline characteristics
Data on 3140 participants, all those randomised in the three contributing trials, were available for analysis. Mean age was 62 years, 75% were male and 76% had established CVD.4 Intervention and control groups were similar at baseline according to major characteristics (table 2).4
Baseline characteristics of SPACE participants
Outcomes
Participants randomised to polypill-based care were more likely to achieve recommended ESC targets for BP (62% vs 58%, RR 1.08, 95% CI 1.02 to 1.15) and LDL (39% vs 34%, RR 1.13, 95% CI 1.02 to 1.25) but not antiplatelet therapy (96% vs 96%, RR 1.00, 95% CI 0.98 to 1.01) when compared with those receiving usual care at 12-month follow-up (table 3). The benefit of polypill-based care compared with usual care was more pronounced when considering simultaneous achievement of all three targets for BP, LDL and antiplatelet therapy at 12 months (24% vs 19%, RR 1.27, 95% CI 1.10 to 1.47). The absolute achievement of all three targets simultaneously was modest in both groups. Similar relative benefits were observed for the effect of polypill-based care compared with usual care in the achievement of UK19–23 and US24–26 guidelines (online supplementary appendix 1), as well as using a longer follow-up period (end of trial, median duration 15 months, online supplementary appendix 4).
Supplementary file 1
Supplementary file 4
Achievement of European treatment targets at 12 months
After including those with missing data (who were no less likely to have achieved these targets at baseline compared with those with available data, online supplementary appendix 5) using multiple imputation, similar relative benefits of polypill-based care compared with usual care were also observed on the achievement of ESC targets at 12 months (online supplementary appendix 6).
Supplementary file 5
Supplementary file 6
Subgroup analyses
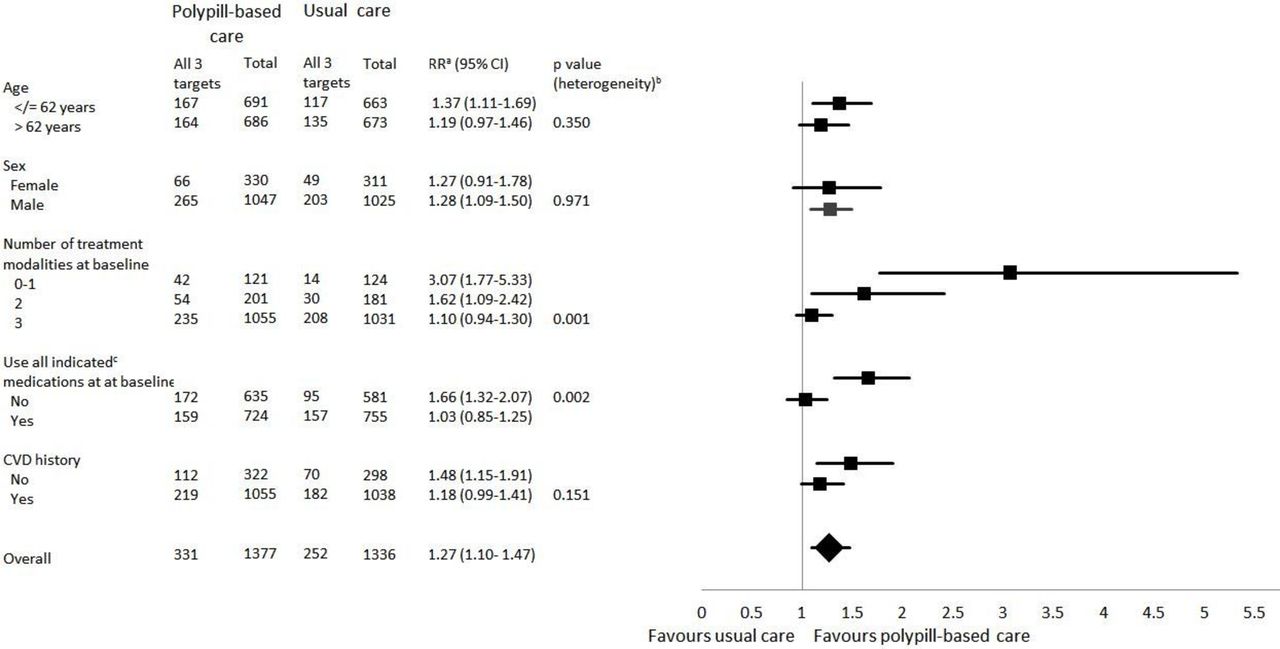
The effect of polypill-based care on the achievement of all recommended treatment targets simultaneously at 12 months was not significantly different according to age group, sex or history of CVD (figure 1, online supplementary appendix 2). There was heterogeneity in the effect of polypill-based care compared with usual care on the proportion of participants achieving all recommended treatment targets at 12 months according to baseline treatment (either on the basis of the number of modalities of treatment (p=0.001), or whether or not all indicated medications were being used at baseline (p=0.002)). For patients taking 3, 2 and 0–1 treatment modalities the RRs for reaching all three guideline goals simultaneously were 1.10 (95% CI 0.94 to 1.30, 22% vs 20%), 1.62 (95% CI 1.09 to 2.42, 27% vs 17%) and 3.07 (95% CI 1.77 to 5.33, 35% vs 11%), respectively. Similar patterns were observed in subgroup analyses of the effect of polypill-based care compared with usual care on the achievement of UK and US guideline targets (online supplementary appendix 3).
Supplementary file 2
Supplementary file 3

{kind=link}
Achievement of all threed treatment targets simultaneously at 12 months by subgroup. a,bRR and p value (heterogeneity) estimated from log-binomial regression model. cStatin, antiplatelet and >2 BP-lowering medications; all were indicated according to the participant’s physician on trial entry. dAntiplatelet target only applicable to people with established CVD. BP, blood pressure; CVD, cardiovascular disease; RR, risk ratio.
While there was a wide range in the background rate of reaching all targets across the different guidelines (54% vs 47%, RR 1.13, 95% CI 1.05 to 1.22 for UK and 16% vs 12%, RR 1.37, 95% CI 1.13 to 1.66 for US guidelines), the absolute treatment effects from allocation to polypill-based care compared with usual care were broadly consistent, with numbers needed to treat of 20 for European, 14 for UK and 25 for US, guideline targets.
Discussion
This individual participant data meta-analysis of 3140 participants at high CVD risk found allocation to polypill-based care increased achievement of ESC targets for BP and LDL separately, and all three targets for BP, LDL and antiplatelet therapy simultaneously, when compared with usual care at 12 months. There was no difference between groups in antiplatelet adherence. The beneficial effect of polypill-based care compared with usual care on the proportion of participants achieving all three targets at the same time at 12 months was most pronounced among those receiving no treatment or only one treatment modality at baseline (35% vs 11%, RR 3.07, 95% CI 1.77 to 5.33), which suggests this strategy is most likely to be best targeted to undertreated populations. Effects were similar when achievement of UK and US guidelines targets was assessed and missing data were imputed using multiple imputation.
Despite the improvement in target achievement, only 24% of participants receiving polypill-based care (compared with 19% of those receiving usual care) achieved all three targets simultaneously at 12 months indicating large treatment gaps remained for guideline-recommended therapy. These low rates are primarily driven by low rates of achievement of the ESC LDL-based cholesterol target (39% vs 34%). It should be noted that in 2010, when the SPACE trials were initiated, target LDL levels were higher (eg, 2.5 mmol/L for people with established CVD in the contemporaneous European guideline27). Absolute achievement of all three targets simultaneously at 12 months was much greater using the UK guidelines, which have a total cholesterol-based target (54% vs 47%).
A potential limitation of this study is the reliance on self-reported use of antiplatelet therapy, which risks bias due to inaccurate recall or social desirability.15 A post hoc analysis of baseline data from the IMPACT trial found a high level of agreement between self-reported aspirin use and dispensing data (kappa 0.75, 95% CI 0.69 to 0.82).28 Absolute estimates of aspirin adherence were higher from self-reported use than from dispensing data (77% vs 69%), although dispensing data may not have captured over-the-counter (non-dispensed) aspirin.28
This is the first study, to our knowledge, that has compared the effect of access to a polypill (containing statin, aspirin and BP-lowering medications) with usual care on the achievement of guideline-based treatment targets for CVD. A major strength of this study was that individual participant data from 3140 participants were available from three similar pragmatic clinical trials run in six countries. In addition, the large sample size enabled robust subgroup analyses. This study provides evidence directly relevant to clinical implementation, contrasting with trial designs in which participants are prescribed the same medications as separate pills in the usual care group. In addition, participants were recruited regardless of baseline level or type of therapy, which again aids in assessment of treatment impact in real-life situations29 and is of particular importance when assessing the potential role of a polypill in reducing treatment gaps.
The SPACE trials were designed to compare the efficacy of a polypill-based approach with usual care among patients with indications for treatment. Blinding of participants and their physicians to treatment allocation was not possible. However, a number of strategies reduced the risk of bias associated with the open-label design, such as automated sphygmomanometers with printed recordings and community laboratories blind to participation in the trial for cholesterol measurement.
The rate of achieving all three (LDL, BP and antiplatelet therapy) targets in the usual care group in this trial population was broadly similar to that seen in the EUROASPIRE2 (all participants from Europe) and Survey of Risk Factors (SURF, 66% of participants from Europe)30 surveys. For individual BP, LDL and antiplatelet goal achievement among participants with CVD, we observed 63%, 27% and 96%, respectively, in the usual care group at 12 months, while EUROASPIRE2 observed 57%, 20% and 94%, and SURF30 observed 60%, 30% and 90%. There are relatively few data on the rates of people reaching all three goals simultaneously elsewhere in the literature. Kerr et al reported that 59% of the New Zealand population with CVD were receiving BP-lowering therapy, statin and an antiplatelet.31 This compares with 76% receiving all three modalities in the SPACE trial population at baseline. These results, together with the consistency of treatment effects in terms of improved adherence across diverse geographical regions,4 suggest these findings have important clinical relevance.
The improvements seen here were achieved with two polypill versions containing no dose options. They also contained simvastatin (which was off patent when the trials were designed); more potent statins such as atorvastatin and rosuvastatin were used more commonly in the usual care group. Future research in polypill-based care should use newer polypills encompassing more dose versions and/or more potent components, as this may lead to greater achievement of treatment targets,32 particularly those of the most recent US cholesterol guidelines, which are based on the intensity of statin therapy as opposed to cholesterol levels.33
Although this study assesses achievement of European guidelines, along with those from the UK and USA, our findings are applicable to, and have implications for, low-income and middle-income countries. Generally, guidelines from these countries propose similar targets with respect to BP and lipid levels. For example, guidelines from India and Malaysia recommend a target LDL of less than 1.8 mmol/L and BP of less than 140/90 mm Hg among people with established CVD.34 35
In addition to supporting the achievement of treatment targets, there is evidence that polypill-based care is preferable to treatment with separate medications for other reasons. In the TEMPUS cross-over trial, treatment with the polypill was preferred by 92% of participants compared with treatment with separate medications.36 Given the increasing recognition of the importance of patient experience and preference to the delivery of high-value cardiovascular care,37 patient preference for polypill-based care needs to be considered alongside other benefits of polypill-based care such as improvements in adherence,4 risk factor levels4 and the achievement of treatment targets.
A systematic review and meta-analysis by Santo et al, assessing interventions to improve medication adherence in patients with CHD, found that simple interventions to improve adherence to multiple CVD medications, such as a polypill, significantly improved the odds of being adherent.38 Further, there was no significant difference in the improvement in adherence whether the intervention was simple or complex (two or more components).38 The reviewers concluded that ‘simple one-component interventions might be a promising way to improve medication adherence in a CHD population, as they would be easier to replicate in different settings and on a large scale.’38 However, recent trials that have assessed alternatives to polypill-based care (reminder devices either alone39 or in combination with financial incentives and social support40) have found no statistically significant difference in adherence to usual care.
The ESC guidelines on the prevention of CVD have requested evidence regarding in whom polypill-based care would be most effective.1 This study has demonstrated that polypill-based care resulted in an increase in the proportion of patients achieving treatment targets, especially those who are undertreated at baseline. Polypill-based care should therefore be prioritised in patients undertreated at baseline, particularly given the lack of alternative evidence-based and scalable solutions to address the global problem of suboptimal implementation of guidelines for the prevention of CVD.
Key messages
What is already known on this subject?
Polypill-based care has been shown to improve adherence, systolic blood pressure (BP) and low-density lipoprotein (LDL) cholesterol levels compared with usual care among patients with cardiovascular disease (CVD) or at high risk of their first event.
What might this study add?
This study demonstrates that polypill-based care also resulted in an increase in the proportion of patients achieving guideline treatment targets for BP, LDL and antiplatelet therapy, particularly for patients undertreated at baseline, and despite the use of more potent statins in the usual care group.
How might this impact on clinical practice?
This study adds weight to the growing evidence base supporting polypill-based care as an additional strategy to improve the implementation of guidelines for the prevention of CVD, particularly for undertreated patients.
Acknowledgments
We acknowledge the contribution of the hundreds of collaborators and coinvestigators who helped to undertake the IMPACT, Kanyini-GAP and UMPIRE trials, and the steering committees of each of these trials. We are indebted to the 3140 individuals who volunteered as participants in these trials.
References
Footnotes
Contributors All authors are members of SPACE trial steering committees and as such made substantial contributions to the acquisition of the data for the work. RW is the coordinator, AR is the chair and AP is the deputy chair of the SPACE Collaboration. Analyses were undertaken by SS. The first draft of this paper was written by VS and all authors revised the article critically for important intellectual content. All authors provided final approval of the work to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding RW is funded by an NHMRC early career fellowship. The authors have received grants from several research charities and national funding agencies for research on cardiovascular polypills, and from Dr Reddy’s Laboratories for coordination of the SPACE program (www.spacecollaboration.org). The polypills used in the SPACE trials were manufactured and supplied by Dr Reddy’s Laboratories free of charge. Some authors received funding from Dr Reddy’s Laboratories to attend investigator meetings related to the polypill (VS, RW, AP, ST, CRE, NR, AW, AR). All authors are independent from trial funders. All authors accept full responsibility for the conduct of the study, had access to the data and controlled the decision to publish.
Disclaimer None of the funders or Dr Reddy’s Laboratories had any role in study design, the collection, analysis or interpretation of data, the writing of the article or the decision to submit the article for publication.
Competing interests Support for the submitted work: RW is funded by an NHMRC early career fellowship. The authors have received grants from several research charities and national funding agencies for research on cardiovascular polypills, and from Dr Reddy’s Laboratories for coordination of the SPACE programme (www.spacecollaboration.org). The polypills used in the SPACE trials were manufactured and supplied by Dr Reddy’s Laboratories free of charge. Some authors received funding from Dr Reddy’s Laboratories to attend investigator meetings related to the polypill (VS, RW, AP, ST, NR, AW and AR). George Health Enterprises, the social enterprise arm of The George Institute for Global Health (employer of some coauthors) has received investment for the development of fixed dose combination therapy containing statin, aspirin and blood pressure lowering medications.
Patient consent Not required.
Ethics approval Each SPACE trial complied with the Declaration of Helsinki. Local ethical and regulatory approval was obtained for each SPACE trial. Trial participants gave informed consent before taking part.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note Institutions where work performed: (1) International trial coordinating centre: The George Institute for Global Health, University of New South Wales, Australia. (2) National trial coordinating centres: Centre for Chronic Disease Control, New Delhi, India; International Centre for Circulatory Health, National Heart and Lung Institute, Imperial College London, UK; Julius Center for Health Sciences and Primary Care / Julius Global Health, University Medical Center Utrecht, Utrecht, The Netherlands; National Institute for Health Innovation, University of Auckland, New Zealand; Royal College of Surgeons in Ireland, Dublin, Ireland; The George Institute for Global Health, University of New South Wales, Australia and Hyderabad, India.