Article Text

Abstract
Sodium glucose cotransporter 2 inhibitors (SGLT2i) have emerged as a class of medications with positive cardiovascular (CV) effects across a spectrum of patients with and without type 2 diabetes (T2D). In heart failure with reduced ejection fraction, there is clear evidence that SGLT2i reduce hospitalisations and mortality regardless of the presence of diabetes, and they are now recognised as the fourth pillar of pharmacological management. Recent trial data also indicate promising effects in heart failure with preserved ejection fraction. In patients with T2D and atherosclerotic CV diseases, multiple CV outcomes trials have shown reductions in major adverse CV events. Meta-analysis of these trials also shows lower rates of incident and recurrent atrial fibrillation with SGLT2i. Concerns regarding utilisation in patients with chronic kidney disease have been allayed in trials showing SGLT2i in fact have renoprotective effects. Questions still remain regarding the safety of SGLT2i in the acute heart failure setting and immediately post myocardial infarction, as well as in patients with more advanced stages of chronic kidney disease. Furthermore, studies are underway evaluating SGLT2i in patients with heart valve disease, where positive effects on left ventricular remodelling may, for example, improve functional mitral regurgitation. In this review, we summarise the available evidence of recent CV outcomes trials of SGLT2i, focusing particularly on the application of these agents across various CV diseases. We detail evidence to support increased utilisation of these drugs, which in many cases will reduce mortality and improve quality of life in patients routinely encountered by the CV specialist physician.
- coronary artery disease
- atrial fibrillation
- heart failure
- valvular heart disease
- diabetes mellitus
Statistics from Altmetric.com
Introduction
Sodium glucose cotransporter 2 inhibitors (SGLT2i) have emerged as drugs with positive cardiovascular (CV) effects across patients with a range of CV diseases with and without type 2 diabetes (T2D). This has prompted optimism regarding the potential for these agents to reduce the burden of CV disease, especially in patients with heart failure (HF). Indeed, SGLT2i now feature in UK,1 European2 and US3 cardiology guidelines, highlighting their importance in contemporary clinical practice.
In this review, we summarise data from cardiovascular outcomes trials (CVOTs) of SGLT2i. Attention is paid not only to patients with HF, where the evidence base for SGLT2i use in people without T2D is greatest, but also to those with atherosclerotic CV disease (ASCVD), atrial fibrillation (AF) and valvular heart disease. We also consider the role of SGLT2i in patients with chronic kidney disease (CKD), a group at high risk of CV disease. In several instances the potential benefits of SGLT2i extend beyond patients with T2D and we consider the use of these agents in people without diabetes.
An overview of SGLT2i
SGLT2i prevent reabsorption of glucose in the proximal convoluted tubule of the nephron. This promotes urinary glucose excretion and lowering of blood glucose levels. Secondary effects include modest weight loss (~3 kg) and blood pressure (BP) reduction (~3 mm Hg), predominantly driven by a diuretic effect.4 The first four major CVOTs of the SGLT2i empagliflozin, dapagliflozin, canagliflozin and ertugliflozin recruited only patients with T2D (table 1)5–8 and we have reviewed these previously.9 The predominant CV effects of SGLT2i were reductions in HF hospitalisations, with early data indicating that patients with reduced ejection fraction (EF) derive particular benefits. This prompted trials to specifically address the efficacy of SGLT2i in patients with HF and reduced EF (HFrEF). Although the mechanisms underlying their benefits remain incompletely understood and are the subject of intense research interest,10 it was clear from these early CVOTs that in patients with T2D with or at high risk of CV disease, SGLT2i had marked benefits on clinical outcomes.
Sodium glucose cotransporter 2 inhibitor cardiovascular outcomes trials in patients with type 2 diabetes
SGLT2i in patients with CV conditions
Heart failure
Two large, multicentre, randomised controlled trials, DAPA-HF11 and EMPEROR-Reduced,12 evaluated the impact of the SGLT2i dapagliflozin and empagliflozin on clinical outcomes in patients with HFrEF (table 2). Patients with New York Heart Association (NYHA) class II–IV HF with and without T2D, with reduced left ventricular EF (≤40%) and raised natriuretic peptide levels were included, with excellent baseline contemporary HF treatments. In both studies, there was a significant reduction (~25%) in the primary composite outcome of CV death or HF hospitalisation. Benefits were also observed in symptoms, physical function and quality of life.13 Importantly, the treatment effect was consistent across patients with and without T2D. Understandably these trials have prompted optimism that SGLT2i are the fourth pillar of survival-enhancing medications for HF.14
Sodium glucose cotransporter 2 inhibitors in patients with heart failure and reduced ejection fraction
All patients with stable chronic HFrEF, regardless of NYHA symptom class or diabetes status, should undergo a blood test for fasting plasma glucose and haemoglobin A1c (HbA1c). The prevalence of dysglycaemia is even higher in patients with HF than for ASCVD, approaching 50% in contemporary HF trials.15 16 Diagnosis of T2D, regardless of EF, will permit prompt identification and treatment of diabetes and could be an indication for SGLT2i in patients not represented in the DAPA-HF and EMPEROR-Reduced trials (which only included those with reduced EF).
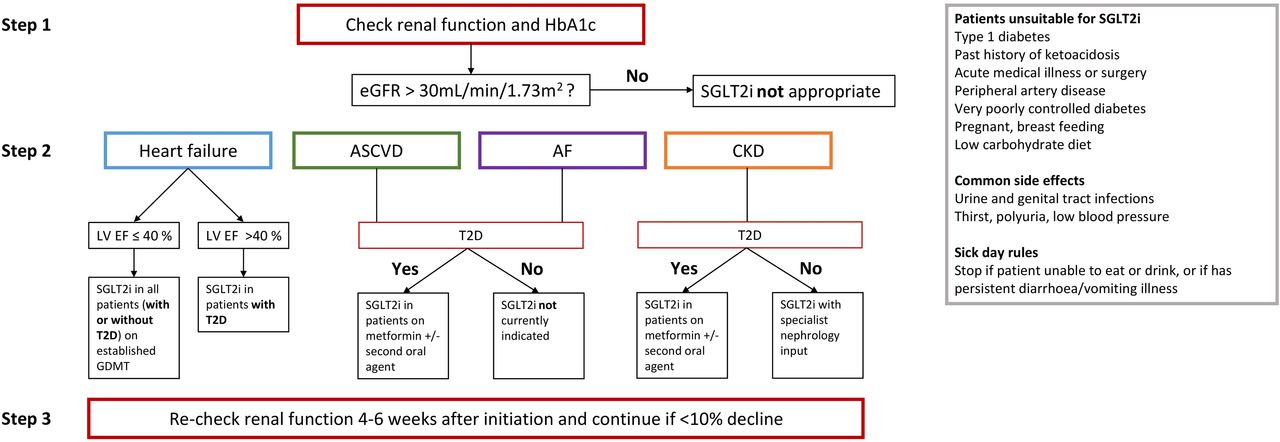
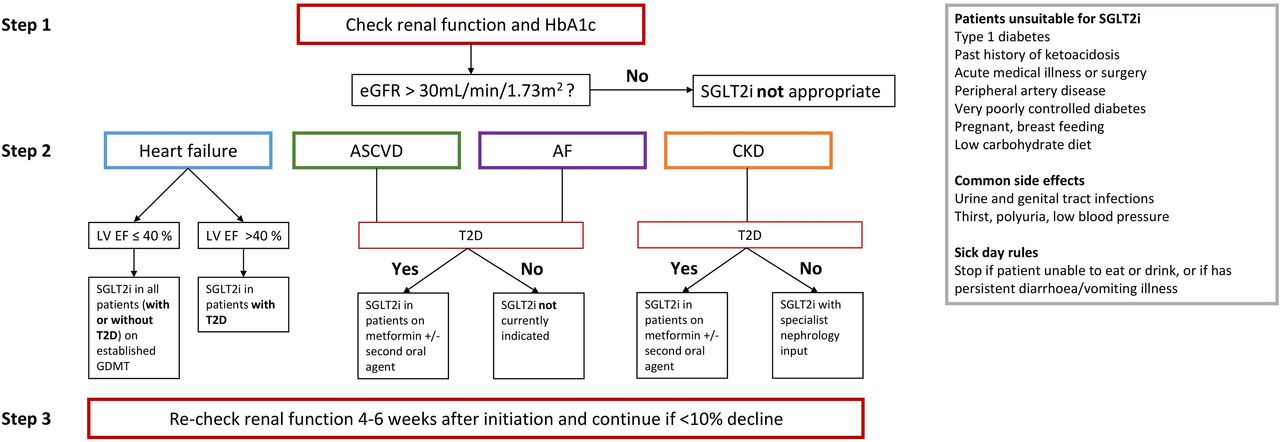
In all patients with HF and EF ≤40%, priority should be given to treatment with contemporary guideline-directed therapies (renin–angiotensin–aldosterone system inhibitors including the angiotensin-neprilysin inhibitor sacubitril-valsartan, beta blockers and mineralocorticoid receptor agonists). Regardless of patients’ HbA1c or diabetes status, initiation of SGLT2i (dapagliflozin 10 mg or empagliflozin 10 mg daily) is advocated in all those with EF ≤40% and estimated glomerular filtration rate (eGFR) ≥30 mL/min/1.73 m2 (figures 1 and 2). Additionally, in patients with T2D and EF >40% (with or without symptoms of HF), commencement of SGLT2i is recommended in those on single or dual oral hypoglycaemic therapy. This is because early SGLT2i CVOTs demonstrated reductions in major adverse CV events (MACE) and HF hospitalisations only in the presence of T2D.5–7

Overview of SGLT2i in patients with cardiovascular disease(s) and chronic kidney disease. AF, atrial fibrillation; CAD, coronary artery disease; CKD, chronic kidney disease; CV, cardiovascular; eGFR, estimated glomerular filtration rate; HF, heart failure; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; MACE, major adverse cardiovascular event; MI, myocardial infarction; PAD, peripheral artery disease; RCT, randomised controlled trial; SGLT2i, sodium glucose cotransporter 2 inhibitor; T2D, type 2 diabetes.
{kind=link}
{kind=link}
Guide for patient selection when initiating SGLT2i. AF, atrial fibrillation; ASCVD, atherosclerotic cardiovascular disease; CKD, chronic kidney disease; EF, ejection fraction; eGFR, estimated glomerular filtration rate; GDMT, guide-directed medical therapy; HbA1c, haemoglobin A1c; LV, left ventricular; T2D, type 2 diabetes; SGLT2i, sodium glucose cotransporter 2 inhibitor.
Patients with HF and preserved EF (HFpEF) represent up to half of those hospitalised with HF,17 18 and T2D is recognised as a risk factor for HFpEF.19 Currently, there are no available therapies proven to improve outcomes in these patients. Trials are underway evaluating the efficacy of SGLT2i in patients with HFpEF both with and without diabetes (EMPEROR-Preserved, ClinicalTrials.gov Identifier: NCT03057951; DELIVER, ClinicalTrials.gov Identifier: NCT03619213). In the recent randomised, placebo-controlled SOLOIST WHF trial, the safety and efficacy of the SGLT2i sotagliflozin (which also provides limited inhibition of the gastrointestinal SGLT1 receptor) were evaluated in patients with T2D (n=1222, age 70 years, 66% male, HbA1c 7.1%) with a recent hospitalisation for acute decompensated HF.20 In almost half (48.7%) of the patients, the study treatment (sotagliflozin or placebo) was initiated during hospital admission, with the remainder soon after discharge (median 2 days). Importantly, 21% of the patients randomised had HFpEF, with an EF ≥50%. Although the trial ended early due to loss of funding from the sponsor, the primary composite outcome of CV death and/or HF hospitalisation was lower in the drug versus placebo group (HR 0.67, 95% CI 0.52 to 0.85, p<0.001) over a median follow-up of 9 months. The treatment effect was more marked in patients with EF ≥50% (HR 0.48, 95% CI 0.27 to 0.86),20 which is an exciting signal of potential efficacy in HFpEF.
Lastly, there are few studies aside from SOLOIST WHF that have explored early in-hospital initiation of SGLT2i following admission with acute decompensated HF. Concerns of early initiation include worsening renal function, hypotension and precipitating euglycaemic ketoacidosis. In selected patients, initiation of SGLT2i in-hospital may be appropriate once clinically stable. Nevertheless, SGLT2i should be commenced as soon as possible after discharge following hospitalisation for HF and will enable patients to derive the most benefit.
Coronary artery disease
Large-scale CVOTs of SGLT2i in patients with T2D and ASCVD (eg, coronary artery disease (CAD), stroke and peripheral artery disease (PAD)) have demonstrated reductions in MACE and HF hospitalisations (table 1). For example, in the EMPA REG OUTCOME trial, ~75% of participants had established CAD, with almost half having had prior myocardial infarction (MI) and a quarter prior coronary artery bypass grafting. A quarter had a history of stroke and over one-fifth had PAD.6 By contrast, only 10% had a history of HF, suggesting that the benefits of SGLT2i extend beyond patients with HF.6 No trial data exist using SGLT2i for secondary prevention of ASCVD in patients without T2D. While the European Society of Cardiology (ESC) recommends initiation of SGLT2i as first line in patients with newly diagnosed T2D and coexisting CAD,2 this approach is not supported by CVOTs, where the vast majority (~75%) of patients were on at least metformin monotherapy prior to enrolment. However, a recent meta-analysis of CVOTs has suggested that the CV benefits of SGLT2i occur regardless of the presence of baseline metformin treatment.21
All patients with and without T2D and CAD should undergo a blood test for fasting plasma glucose and HbA1c, given their high prevalence (5%–30%) of previously undiagnosed diabetes.22–24 Patients with established T2D and CAD should all be considered for SGLT2i (assuming eGFR >30 mL/min/1.73 m2)2 (figures 1 and 2), with the choice of agent based on the discretion of the prescribing clinician, primary care physician and patient preference. It is worth noting that there are alternative glucose-lowering medications to SGLT2i, in particular glucagon-like peptide 1 receptor agonists (GLP-1RAs), which may confer greater benefits in ASCVD in people with T2D.9 GLP-1RAs suppress appetite, glucagon secretion and gastric emptying, and stimulate the release of insulin. Multiple CVOTs of GLP-1RAs have also been completed in people with T2D. Reductions in MACE were demonstrated, which were predominantly driven by lower rates of MI and stroke, rather than HF. Not all GLP-1RAs improved outcomes in their respective CVOTs, suggesting more heterogeneous effects across different drugs in this class.9 Importantly, SGLT2i and GLP-1RA can be used in combination, when their impact may be synergistic.25
Data on the safety and efficacy of SGLT2i in hospitalised patients are limited, although randomised trials are underway.26 27 Initiation of SGLT2i in patients following acute MI should be reserved for the outpatient setting, preferably at the first outpatient clinic appointment post discharge. Unless MI is complicated by acute cardiogenic shock, acute kidney injury or other cause of metabolic acidosis, routine discontinuation of SGLT2i on admission to hospital with acute MI is not recommended.
Atrial fibrillation
T2D is associated with an increased risk of AF,28 and in patients with AF diabetes is associated with worse symptoms, poorer quality of life and increased risk of death and HF hospitalisation.29 Given SGLT2i reduce body weight, BP and HbA1c, it is possible that they may play a role in reducing the burden of symptoms and frequency of AF as obesity and hypertension are themselves risk factors for AF. However, no randomised trials have specifically evaluated the impact of SGLT2i on AF-related outcomes.
In a recent meta-analysis of 16 randomised trials of SGLT2i in patients with T2D (comprising 38 335 patients), SGLT2i use was associated with lower incidence of new-onset and recurrent AF, regardless of patients’ age, body weight, HbA1c or BP on initiation.30 It is posited that the multifactorial AF risk factor reduction conferred by SGLT2i may be responsible for this observed effect. Indeed, the 2020 ESC guidelines advocate risk factor control as a key component for the management of AF,31 for which SGLT2i may be beneficial (figures 1 and 2), especially in those patients with coexisting obesity and hypertension.
Valvular heart disease
No studies have explored the potential benefits of SGLT2i in patients with valvular heart disease. Patients with HF secondary to a primary valvular aetiology were excluded from the DAPA-HF and EMPEROR-Reduced trials. Mechanistic studies have shown that treatment with SGLT2i may be associated with positive left ventricular remodelling,32 33 which may contribute to the observed benefits in HF risk reduction with these agents. There may therefore be a role for SGLT2i in patients with, for example, functional mitral regurgitation. Trials are underway exploring this indication for SGLT2i.34 Nevertheless, there is currently no apparent role for SGLT2i in patients with primary valvular heart disease out with the indications listed in figure 1.
Cerebrovascular disease
No significant reduction in stroke events was observed in SGLT2i CVOTs (table 1), although none of the trials was specifically powered to detect improvements in this outcome. Meta-analysis findings (incorporating data from 32 randomised trials in over 75 000 patients) have shown that SGLT2i do not increase the relative risk of stroke,35 indicating that these drugs can be used safely in individuals who have a history of cerebrovascular disease. Furthermore, SGLT2i lead to beneficial effects on a number of stroke risk factors, including blood glucose levels, BP, body weight and AF. In the longer term, this could lead to a reduced risk of stroke with SGLT2i therapy, although GLP-1RAs have demonstrated greater efficacy in this regard.9 While SGLT2i can be safely continued in patients with a history of stroke or transient ischaemic attack, there are no data to support their use for primary or secondary prevention of cerebrovascular events.
Peripheral artery disease
The observation from the CANVAS trial that canagliflozin was associated with an increased risk of leg and mid-foot amputations has understandably led to caution with the use of SGLT2i in patients with PAD.7 The same risk of limb amputation was not observed in trials of other SGLT2i or indeed in the CREDENCE trial of canagliflozin in patients with diabetic kidney disease,36 and it is unclear whether this is a class effect. Retrospective data in patients newly commenced on SGLT2i suggest there is a twofold increased risk of amputation compared with sulfonylureas, metformin or thiazolidinediones (adjusted HR 2.12, 95% CI 1.19 to 3.77). Further studies are needed to clearly define whether SGLT2i do indeed increase the risk of limb amputation. This is especially important given a high proportion (eg, ~20% in the EMPA REG OUTCOME trial)6 of patients in SGLT2i CVOTs had a history of PAD, and these patients may derive considerable benefit from SGLT2i if they can be safely administered.
Chronic kidney disease
Alongside their cardioprotective effects, CVOT data indicate that SGLT2i confer significant renoprotection. These effects were first reported in the CANVAS-R trial, where treatment with canagliflozin was associated with a reduction in the progression of albuminuria (HR 0.73, 95% CI 0.67 to 0.79) and a reduction in the risk of the composite outcome of a sustained 40% reduction in eGFR, need for renal replacement therapy or death from renal causes in patients with diabetic kidney disease (HR 0.60, 95% CI 0.47 to 0.77).7 Similar effects were observed in prespecified secondary analyses of the EMPA REG OUTCOME trial, regardless of the severity of CKD.37 38 These data were confirmed in the CREDENCE study, in which patients with T2D and albuminuric CKD received canagliflozin 100 mg daily or placebo. The primary outcome was a composite of end-stage kidney disease, a doubling of the serum creatinine level, or death from renal or CV causes, and the relative risk of the primary outcome was 30% lower in the canagliflozin group than in the placebo group (HR 0.70, 95% CI 0.59 to 0.82).36
As with the DAPA-HF and EMPEROR-Reduced trials in patients with HF, the observed renoprotective effects of SGLT2i prompted their investigation in patients with CKD, with and without diabetes. In the DAPA-CKD trial, patients with CKD (n=4304, age 62 years, 33% female, mean eGFR: 43 mL/min/1.73 m2; eGFR <30: 14%, 30–45: 44%, 45–60: 31%) with or without T2D were randomised to dapagliflozin 10 mg daily versus placebo. Over a median follow-up of 2.4 years, dapagliflozin was associated with a reduction in the primary composite endpoint of decline in eGFR ≥50%, end-stage kidney disease, death from renal causes or CV death versus placebo (HR 0.61, 95% CI 0.51 to 0.72, p<0.001). This finding was consistent regardless of the presence of T2D, again indicating that SGLT2i have beneficial effects extending beyond people with diabetes. Although the glucose-lowering potential of SGLT2i is curtailed in patients with impaired kidney function, the renoprotective benefits persist, supporting their use in patients regardless of HbA1c. Furthermore, the inclusion of patients with eGFR as low as 25 mL/min/1.73 m2 indicated that SGLT2i may be safely used in patients with as low as stage 3b CKD even in the absence of T2D.
The findings of the DAPA-CKD trial support the use of SGLT2i in patients with CKD, which is highly prevalent in patients with CV disease and has previously been a limiting factor for the adoption of these drugs in clinical practice.9 National and international guidelines recommending the use of SGLT2i in patients with CKD are awaited. Trial data indicate SGLT2i can be safely initiated in patients with T2D and CV disease, with eGFR as low as 30 mL/min/1.73 m2, alongside watchful monitoring of renal function (figure 1). Use of SGLT2i in patients with CV disease and CKD in the absence of T2D, for renoprotection alone, would currently constitute off-label use and at the time of writing should only be initiated by nephrologists in secondary care.
Patients unsuitable for SGLT2i and monitoring requirements
We have previously reviewed key considerations for prescribing SGLT2is, including their risks and side effects.9 Despite the largely inclusive indications for commencing SGLT2i in a wide range of patient groups, there remain a proportion of patients in whom SGLT2i may not be suitable. Patients taking other oral hypoglycaemic agents and/or insulin may require dose adjustment after initiation of SGLT2i, where diabetes specialist physician input is advisable. Given their specific risks and side effects, the Association of British Clinical Diabetologists suggests avoiding SGLT2is in certain groups (figure 2),39 which included patients with eGFR <60 mL/min/1.73 m2 and those on loop diuretics. However, recent trial data have shown in patients with HF and CKD that SGLT2i are safe in patients on diuretics11 12 and in fact reduce progression of CKD.40 Nevertheless, routine blood testing for renal function should be undertaken 4–6 weeks after initiation of SGLT2is, where these agents can be safely continued if there is an anticipated <10% reduction in eGFR.
Sick day rules
Clinician and patient education regarding the risk of euglycaemic ketoacidosis associated with SGLT2i is essential to ensure safe administration (figure 2). Although the relative risk of ketoacidosis is low (incidence ~1.3 per 1000 patient years),41 it is a serious complication of SGLT2i use. Risk factors include intercurrent illness, reduced oral intake, low carbohydrate diets, reduced insulin doses and history of alcohol intake. The Association of British Clinical Diabetologists suggests patients taking SGLT2i should be provided clear guidance to reduce the risk of ketoacidosis during an acute illness or in the event of reduced intake.39
Euglycaemic diabetic ketoacidosis should be suspected in patients on SGLT2i with nausea, vomiting, abdominal pain, dyspnoea, confusion, fatigue and drowsiness. A prompt venous blood gas helps confirm the diagnosis (ketones >3.0 mmol/L, pH <7.30, bicarbonate <15 mmol/L), noting that blood glucose levels may be normal. Patients with ketosis should have a fixed-rate intravenous insulin infusion and fluids, regardless of the glucose level (indeed additional glucose infusion may be necessary to avoid hypoglycaemia).39 Clinicians should refer to local guidance for more details on the management of euglycaemic ketoacidosis.
Conclusions
SGLT2i have beneficial effects across a spectrum of CV conditions, including in certain patients without T2D. In HFrEF there is clear evidence that SGLT2i reduce hospitalisations and mortality regardless of the presence of diabetes. Recent trial data also indicate promising effects in HFpEF. In patients with T2D and ASCVD, multiple CVOTs have shown reductions in MACE. Meta-analysis findings show lower rates of incident and recurrent AF with SGLT2i. Concerns regarding utilisation in patients with CKD have been allayed in randomised trials showing SGLT2i in fact have renoprotective effects. Questions remain regarding the safety of SGLT2i in the acute HF setting and post-MI, as well as in patients with more advanced stages of CKD. Nevertheless, administration of SGLT2i in suitable patients can improve symptoms and prolong length of life. Every effort should be made to increase utilisation of these drugs, while being aware of their potential risks and side effects.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors GSG conceived the idea for the review. GSG and MPMG-B drafted the manuscript, which was critically reviewed by GPM, IS and MJD. All authors approved the final submission.
Funding GPM is funded through a National Institute for Health Research (NIHR) Research Professorship (RP-2017-08-ST2-007) and GSG is supported by a British Heart Foundation Travel Fellowship (FS/TF/21/33008). All authors receive support from NIHR Leicester Biomedical Research Centre and NIHR Leicester Clinical Research Facility.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.