Article Text

Abstract
Objective The coexistence of wild-type transthyretin cardiac amyloidosis (ATTR) is common in patients with severe aortic stenosis (AS) undergoing transcatheter aortic valve implantation (TAVI). However, the impact of ATTR and AS on the resultant AS-ATTR is unclear and poses diagnostic and management challenges. We therefore used a multicohort approach to evaluate myocardial structure, function, stress and damage by assessing age-related, afterload-related and amyloid-related remodelling on the resultant AS-ATTR phenotype.
Methods We compared four samples (n=583): 359 patients with AS, 107 with ATTR (97% Perugini grade 2), 36 with AS-ATTR (92% Perugini grade 2) and 81 age-matched and ethnicity-matched controls. 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid (DPD) scintigraphy was used to diagnose amyloidosis (Perugini grade 1 was excluded). The primary end-point was NT-pro Brain Natriuretic Peptide (BNP) and secondary end-points related to myocardial structure, function and damage.
Results Compared with older age controls, the three disease cohorts had greater cardiac remodelling, worse function and elevated NT-proBNP/high-sensitivity Troponin-T (hsTnT). NT-proBNP was higher in AS-ATTR (2844 (1745, 4635) ng/dL) compared with AS (1294 (1077, 1554)ng/dL; p=0.002) and not significantly different to ATTR (3272 (2552, 4197) ng/dL; p=0.63). Diastology, hsTnT and prevalence of carpal tunnel syndrome were statistically similar between AS-ATTR and ATTR and higher than AS. The left ventricular mass indexed in AS-ATTR was lower than ATTR (139 (112, 167) vs 180 (167, 194) g; p=0.013) and non-significantly different to AS (120 (109, 130) g; p=0.179).
Conclusions The AS-ATTR phenotype likely reflects an early stage of amyloid infiltration, but the combined insult resembles ATTR. Even after treatment of AS, ATTR-specific therapy is therefore likely to be beneficial.
- aortic valve stenosis
- transcatheter aortic valve replacement
- cardiomyopathy
- restrictive
Data availability statement
No data are available.
Statistics from Altmetric.com
Introduction
Severe aortic stenosis (AS) and wild-type transthyretin cardiac amyloidosis (ATTR) are common in the elderly.1 2 Recent studies have demonstrated that transthyretin amyloid coexists with severe AS at a prevalence of 13%–16%.3–5 Cardiac amyloid is graded with bone scintigraphy using the Perugini system: 0 representing no amyloid, 1–3 representing increasing grades.6 In AS, a small degree of amyloid (Perugini grade 1) is typically considered bystander, but grades 2 and 3 (AS-ATTR) have been described as having amyloidosis-like characteristics including: demographics (older age and marked male predominance), electrocardiography (low voltage), cardiac morphology (unexplained hypertrophy, low-flow and low-gradient AS) and poorer outcomes.3 4 7 However, studies to date have had three limitations: first, some have made the distinction between AS and AS-ATTR in response to clinical suspicion, risking selection bias. Second, many studies have reported cases from a single centre/region. Third, comparisons have not been complete: while AS has been compared with AS-ATTR,3 5 8 comparisons with ATTR (specifically, wild-type transthyretin cardiac amyloidosis) and older age controls have not been made. A fuller appreciation of AS-ATTR requires this 2×2 matrix comparison of AS (present/absent) and ATTR (present/absent). Biologically, AS and ATTR are both diseases impacting the myocardium through incompletely understood processes affecting both the interstitium and myocytes, with age-specific and sex-specific influences. It is therefore plausible that the resulting phenotype, AS-ATTR, may be the product of a biological interaction between both diseases, sufficient to render AS-ATTR an extreme phenotype from the sum of both diseases. Alternatively, one disease could dominate the clinical phenotype, with the other disease either acting as a bystander or having less impact.
Recent advances in diagnostics, particularly bone scintigraphy, have underlined the clinical impact of cardiac amyloidosis, while new pharmacotherapies now offer symptomatic and prognostic benefits.9 10 Transcatheter aortic valve implantation (TAVI) has revolutionised the treatment of AS for nearly the last two decades and has demonstrated improved mortality in cases of AS-ATTR.5 11 This is intriguing as the amyloid component still remains post-TAVI but does not seem to influence mortality. Studies to date have not evaluated the effect of amyloid-targeted therapy on outcomes among patients with AS-ATTR. It is therefore important to understand the phenotype of AS-ATTR as its presentation, natural history, response to treatment and prognosis may behave differently in the presence of a potential disease modifier. Clinically, this will help define diagnostic and therapeutic pathways and allow evaluation of associated costs, side effects and complications. Accordingly, we set out to evaluate myocardial structure, function, stress and damage by comparing AS-ATTR to AS and ATTR in patients, and older age controls, in order to understand the relative impact of each individual disease (AS related afterload and amyloid infiltration) on the resulting phenotype.
Methods
Study population
Four prospectively recruited cohorts were combined (total n=583): older age controls from the Southall And Brent REvisited (SABRE) study.12 AS and AS-ATTR from the Role of Occult Cardiac Amyloid in the Elderly with Aortic Stenosis (ATTRact AS) study and a Vienna General Hospital study and ATTR from the UK National Amyloid Centre (NAC) registry. Table 1 shows the 2×2 matrix cohort model that was used for this study. AS, AS-ATTR and ATTR cohorts consisted of screened patients with complete data. The older age cohort provided age-expected comorbidities, matching that of the patient cohorts. All participants provided informed consent, and each study was approved by a local research ethics committee. Patients, as part of the patient and public involvement programme for valvular heart disease, were involved in the design of this study. Participants had demographic data, cardiac biomarkers (NT-proBNP and high-sensitivity troponin-T), electrocardiography, echocardiography and clinical data collected. Wild-type transthyretin cardiac amyloidosis was identified in all patients using bone scintigraphy and exclusion of light chain (AL) amyloidosis in accordance with international guidelines.13
Study population according to the presence or absence of aortic stenosis and amyloidosis
SABRE cohort
A sample of elderly, European origin patients, without significant valvular heart disease, history of myocardial infarction or known heart failure was selected to provide a population-based, older age, control cohort that was matched to the disease cohorts on age and ethnicity. This cohort did not have 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid (DPD) scintigraphy.
AS-ATTR cohort
This cohort composed of patients recruited from two prospective observational studies: ATTRact AS (a two-centre (John Radcliff Hospital (JRH), Oxford, UK and St Bartholomew’s Hospital (SBH), London, UK), study of patients 75 years or older with severe AS referred for a TAVI recruited between October 2016 and February 2019 (NCT03029026)) and a study from Vienna General Hospital (recruited consecutive patients referred for a TAVI between October 2017 and January 2019). Consenting patients underwent pre-TAVI DPD scintigraphy to identify coexisting amyloid. Further assessments in positive DPD patients (serum free light chain ratio and monoclonal immunoglobulin in the serum and urine by immunofixation and genotyping) identified wild-type transthyretin cardiac amyloidosis based on international guidelines.13 For this study, we only considered patients with wild-type transthyretin cardiac amyloidosis, Perugini grades 2 and 3, named as AS-ATTR and did not include those with Perugini grade 1. This resulted in two cohorts: 359 patients with AS and 36 patients with AS-ATTR.
ATTR cohort
The NAC is a tertiary referral centre in the UK. For this study, we chose consecutively referred, newly diagnosed patients with wild-type transthyretin cardiac amyloidosis, Perugini grades 2 and 3 (ATTR), totalling 107 patients. Diagnosis of wild-type transthyretin cardiac amyloidosis was based on international guidelines.13 Patients with coexisting mild to moderate AS (n=4) and Perugini grade 1 (n=2) were excluded.
Biomarkers
All subjects had NT-proBNP and high-sensitivity troponin-T (hsTnT) measured at their index consultation.
DPD scintigraphy
All patients (not older age controls) underwent DPD scintigraphy. The imaging protocol at the JRH, NAC and SBH consisted of an early (5 min) and late (3 hours) planar whole-body image. Scans were performed using aligned protocols and Perugini scoring, with grade 0 being negative, grades 1–3 increasingly positive as previously described.6 Among positive patients, further assessments (serum free light chain ratio and monoclonal immunoglobulin in the serum and urine by immunofixation) to rule out AL amyloid and genotyping identified wild-type transthyretin cardiac amyloidosis based on international guidelines.13 Patients with Perugini grade 1 were excluded from this study.
Echocardiography
All patients underwent transthoracic echocardiography by experienced accredited echocardiographers. Different machines and software were used at different sites for image acquisition. Chamber and valve quantification was according to international recommendations.14 Cardiac parameters were measured using EchoPAC software (GE Healthcare, Wauwatosa, Wisconsin, USA). Left ventricular (LV) mass was calculated using methodology described previously.15 Myocardial contraction fraction (MCF) was derived from the ratio of stroke volume over myocardial volume. Global longitudinal function (GLS) was acquired using strain imaging in the apical 4, 3 and 2 chamber views and is an average of all 17 segments.
Study endpoints
For the purposes of statistical modelling, end-points were selected as markers of myocardial damage, structure and function. The primary end-point was NT-proBNP, based on its prognostic value in patients with AS and ATTR. The secondary endpoints used were:
Left ventricular mass indexed as it is a marker of amyloid burden and a frequent consequence of remodelling in AS.
MCF and global longitudinal strain (GLS) as markers of LV systolic function.
E/A ratio to assess LV diastolic function.
Tricuspid annular planar systolic excursion (TAPSE) to assess right ventricular systolic function.
hsTnT as a marker of myocardial damage.
Carpal tunnel syndrome as a marker of systemic ATTR involvement.
Statistical analysis
Continuous data describing the sample are summarised as mean±SD or median (IQR) for skewed data; categorical data are summarised as frequencies (percentages). Results from the four diagnostic groups were compared using multivariable regression modelling with covariate adjustment to control confounding. Results are presented as marginal means and 95% CIs. Covariates were chosen as potential confounders based on a priori evidence indicating correlations with both exposure and outcome. Covariates were sex, age, diabetes, hypertension, high cholesterol and chronic kidney disease. Additional sensitivity analyses were performed to check the results of the regression modelling, using augmented inverse-probability weighting (AIPW) to achieve confounder balance across the four groups. AIPW is a statistical approach that combines propensity-based inverse probability weighting (where the contribution of an individual’s data is weighted by the propensity score) and regression adjustment. AIPW has the advantage that it is ‘doubly robust’, such that only one of the two methods need be correctly specified to obtain an unbiased effect estimator.16
Additional data on comorbidities, ECG and echocardiographic findings are provided in online supplemental table 1. These parameters were not included in the main analysis and are presented to provide a more complete description of each cohort, rather than for inferential purposes. All statistical analyses were performed using SPSS statistics software (V.26, IBM) or Stata SE (V.15.1, StataCorp LLC). For the primary outcome (NT-ProBNP), a two-sided p value of <0.05 was considered significant. Inferences on other outcomes were made based on the means and 95% CIs.
Supplemental material
Results
Study population
Baseline characteristics of the four prospective cohorts are shown in table 2, online supplemental table 1, figure 1 and figure 2. Patient demographics for the four cohorts were:
Older age controls (AS negative, ATTR unlikely) cohort (n=81) was 69% male, median age of 82 (80, 84) years.
AS (ie, ATTR negative, severe AS) cohort (n=359) was 49% male, median age of 85 (80, 88) years.
AS-ATTR cohort (ATTR positive, severe AS) cohort (n=36) was 61% male, median age of 88 (85, 92) years with Perugini grade 2 identified in 33 patients (92%) and grade 3 in 3 patients (8%).
ATTR (ATTR positive, AS negative) cohort (n=107) was 94% male, median age of 80 (75, 84) years. Perugini grade 2 was identified in 104 patients (97%) grade 3 in 3 patients (3%).

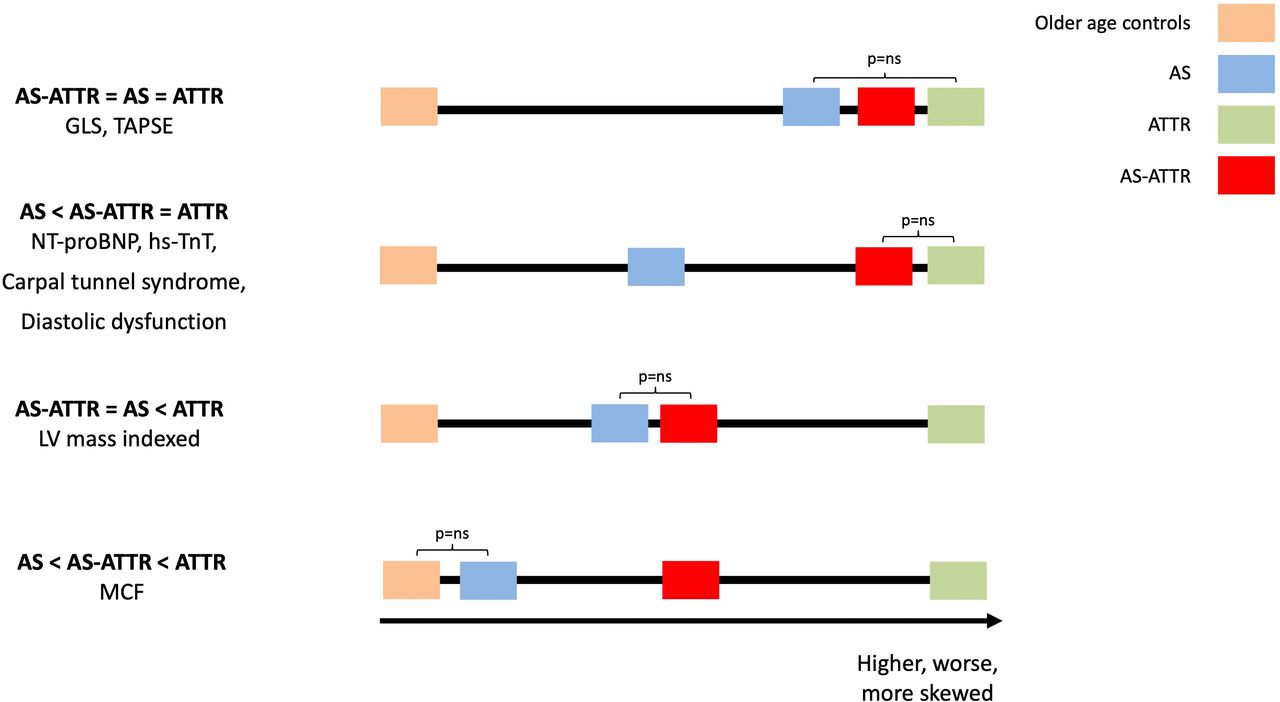
Characterisation of AS-ATTR. AS-ATTR was compared with AS, ATTR and older age controls (not drawn to scale). For some parameters (GLS and TAPSE), AS-ATTR was similar to AS and ATTR, while for others, it was similar to ATTR and higher than AS (cardiac biomarkers, carpal tunnel syndrome and diastolic dysfunction). AS-ATTR was similar to AS and less than ATTR for LV mass indexed and in between AS and ATTR for MCF. AS, aortic stenosis; hsTnT, high-sensitivity troponin; LV, left ventricular; LVEF, left ventricular ejection fraction; MCF, myocardial contraction fraction; TAPSE, tricuspid annular plane systolic excursion; TNT-proBNP, N terminal probrain natriuretic peptide.

{kind=link}
{kind=link}
Multimodality characterisation of AS-ATTR. Echocardiographic and DPD (axial single photon emission CT/CT (SPECT/CT) and planar) images of patients from all four cohorts: older age control, AS, AS-ATTR and ATTR. Echocardiography shows an apical four-chamber (A4C) view. SPECT/CT shows coronal slices at the level of the heart showing radioisotope uptake superimposed on a CT image. Planar images show cardiac radioisotope uptake relative to bony uptake. AS, aortic stenosis; DPD, diphosphono-1,2-propanodicarboxylic acid.
Comparison of AS-ATTR to older age controls, AS and ATTR using regression analysis
AS-ATTR patients with Perugini grade 1 were excluded from this study (n=16). The AS-ATTR cohort was older than all three other cohorts (p<0.005 for trend) but between AS and ATTR for male predominance (61%; p<0.005 for trend).
Impact on myocardial stress
Patients with AS-ATTR had higher NT-proBNP (2844; 95% CI (1745 to 4635) ng/dL) than older age controls (127; 95% CI (100 to 162) ng/dL; p<0.001) and AS (1294; 95% CI (1077 to 1554)ng/dL; p=0.002) and similar to ATTR (3272; 95% CI (2552 to 4197)ng/dL; p=0.63). These results are consistent with the doubly robust analysis (table 2 and online supplemental table 2).
Impact of myocardial structure
LVMi in AS-ATTR was greater than in older age controls, similar to AS and lower than ATTR. Doubly robust analysis demonstrated no significant difference between groups except between older age controls and AS-ATTR. However, CIs are wide (table 2 and online supplemental table 2).
Impact of myocardial function
GLS and TAPSE in AS-ATTR was impaired and similar to AS and ATTR. All three patient cohorts had worse function compared with older age controls. However, MCF in AS-ATTR was worse compared to AS and better compared to ATTR, with older age controls demonstrating the best MCF. E/A ratio in AS-ATTR (restrictive diastology) was worse than AS and older age controls and similar to ATTR. These results are consistent with the doubly robust analysis except for GLS where CIs for older age controls are wide and for E/A ratio where comparison with AS demonstrates a trend towards significance (p=0.069) (table 2 and online supplemental table 2).
Impact on myocardial damage
HsTnT in AS-ATTR was higher than AS and older age controls and similar to ATTR. These results are consistent with the doubly robust analysis (table 2 and online supplemental table 2).
Systemic impact of ATTR
Carpal tunnel syndrome in AS-ATTR was more frequent compared with AS and similar to ATTR. These results are inconsistent with the doubly robust analysis; however, overall numbers of carpal tunnel syndrome are small limiting statistical power (table 2 and online supplemental table 2).
Discussion
Using a multicentre, multicohort approach of over 500 patients, we characterised AS-ATTR by comparing the phenotype to that of AS, ATTR and age-matched and ethnicity-matched controls.
Four main conclusions can be drawn (figure 1). First, despite an equivalent amyloid infiltration bone scintigraphy grade of ATTR, myocardial remodelling (LVMi) in AS-ATTR is similar to AS and less than ATTR, suggesting a lower amyloid burden in AS-ATTR patients and possibly that they are detected early. Second, the impact of dual pathology on the clinical phenotype is increased myocardial stress and damage with NT-proBNP and hsTnT levels similar to patients with ATTR. Third, systolic longitudinal function is impaired in AS-ATTR but similar to the AS and ATTR phenotype. Fourth, diastology in AS-ATTR is restrictive and closely resembles ATTR. We therefore conclude that the dual insult of AS and ATTR results in a combined phenotype most closely resembling ATTR (rather than a more severe phenotype) due to a lower amyloid but higher afterload burden.
AS-ATTR creates several challenges, from diagnostics- screening patients with AS for coexisting ATTR to management-timing (either pre-aortic or post-aortic valve replacement) and mode of aortic valve interventions (either surgical aortic valve replacement or TAVI) and amyloid-targeted therapy. This makes understanding the relative impact of each contributing pathology very important.
DPD grades are indicative of the distribution of amyloid in the heart relative to other organ systems. Despite comparing patients with only Perugini grade 2 (majority of patients) and 3 and adjusting for several covariates, AS-ATTR had a lower amyloid burden (estimated using LVMi) compared to ATTR. The most plausible reason for this is that the amyloid in AS-ATTR, here discovered by screening, was simply an earlier phase of amyloid compared with the ATTR cohort, which was derived from a national referral cohort. Despite the lower amyloid burden, the dual impact of AS-related afterload and ATTR-related infiltration may be sufficient to drive certain markers of myocardial remodelling to resemble those of ATTR.
Both NT-proBNP and hsTnT have demonstrated prognostic value in patients with AS17 18 and ATTR.19 20 In AS-ATTR, the double hit to the myocardium from AS-related afterload and amyloid infiltration significantly increases both biomarkers. However, despite this increase, mortality is similar between AS and AS-ATTR post-TAVI,5 11 suggesting that the AS component of AS-ATTR is the dominant pathology in AS-ATTR. This calls for an evaluation of the biomarkers’ prognostic role in AS-ATTR but supports their diagnostic value in discriminating AS-ATTR from AS.11
Assessment of LV systolic function using left ventricular ejection fraction in patients with cardiac remodelling can be misleading as changes in ventricular capacitance are not accounted for. GLS is a more sensitive marker of LV function and was found to be similar between AS-ATTR and AS and ATTR, indicating that longitudinal deformation is unaffected by dual pathology. However, when indexing stroke volume to the amount of myocardium using MCF, there is a clear difference between all four cohorts with AS-ATTR demonstrating better function than ATTR but worse function than older age controls and AS. This indicates the impact of amyloid in AS-ATTR alters ventricular geometry and reduces function without significantly increasing LVMi. The amyloid component of AS-ATTR also contributes to worse diastolic function compared with AS, resulting in a restrictive physiology similar to ATTR.
Our study differed from previous descriptions of AS-ATTR, which likely reflects differences in sample selection, study methodology and ascertainment, here exclusively by prospective screening. There are similarities between our data and others on the description of AS-ATTR compared with AS: worse diastolic function and MCF. However, our study has demonstrated similar GLS and LVMi, higher cardiac biomarkers and more carpal tunnel syndrome in AS-ATTR compared with AS.3 4
Our findings have important clinical implications. The similarities in cardiac function, biomarkers and carpal tunnel syndrome between AS-ATTR and ATTR suggest that the amyloid component in AS-ATTR plays a key role in the phenotype, and given that the amyloid burden may be lower in AS-ATTR, the phenotype may be more amenable to treatment than previously thought. Although speculative, amyloid-stabilising drugs such as tafamidis may have a greater benefit when treating amyloid at an earlier stage than at later stages when the amyloid burden and impact is greater. Therefore, studies evaluating the effect of amyloid-targeted therapy are needed for AS-ATTR.21 Treating AS-ATTR only with aortic valve replacement would neglect a significant part of phenotype. The subtle differences between AS-ATTR and AS call for a high index of suspicion and screening pathways to identify AS-ATTR in patients with AS. AS-ATTR affects the elderly, where quality of life and symptomatic relief are just as important as mortality benefit; future studies need to consider these outcomes when trialling interventions for AS-ATTR.
Limitations
Ascertainment bias remains in this study due to the different recruitment strategies for each cohort. Although we matched across cohorts using regression and augmented inverse probability weighting, some differences may persist. Despite a relatively high prevalence of coexisting amyloid in patients with AS, the number of patients in this study with AS-ATTR is low; a multicohort approach was therefore used to overcome this. Diastolic function was only assessed with one parameter: E/A ratio and further studies need to provide a more detailed analysis of diastology. Pacemaker rates were not compared due to the impact of TAVI on pacemaker need. Lastly, the older age cohort did not have bone scintigraphy, so some occult amyloid may have been missed; we, minimised this by selecting participants without a history of heart failure, and given their normal echocardiographic appearance and biomarker levels, ATTR within this cohort was deemed unlikely. This is a cross-sectional study at a single time point, and further longitudinal studies are needed.
Conclusions
AS-ATTR is a mixed phenotype, which is worse than AS but is not the summation or even potentiation of the two insults (afterload and infiltration). It likely reflects an early stage of amyloid infiltration, but the combined insult in a phenotype resembles ATTR. Even after treatment of AS, ATTR-specific therapy is therefore likely to provide benefit.
Key messages
What is already known on this subject?
Wild-type Transthyretin cardiac amyloidosis (ATTR) is common among patients with aortic stenosis (AS). Transcatheter aortic valve implantation reduces mortality and should not be withheld among such patients.
What might this study add?
AS-ATTR is a mixed phenotype, which is worse than AS but is not the summation or even potentiation of the two insults (afterload and infiltration); it is likely to reflect an early stage of amyloid infiltration. Despite this, the phenotype resembles ATTR in terms of cardiac biomarkers, longitudinal systolic function, diastology and the prevalence of carpal tunnel syndrome. The AS-ATTR phenotype is also broad with majority of features resembling ATTR, a few features resembling AS and some different from both AS and ATTR.
How might this impact on clinical practice?
ATTR-specific therapies are likely to be of benefit among patients with AS-ATTR. Current screening approaches (eg, screening only males, or low-flow low-gradient AS) may miss patients with AS-ATTR due to its broad and varied phenotype.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was first published. Duplications of a sentence in the Abstract were removed and the headings in Figure 2 were updated to be consistent with the main text.
Contributors Conception and study design: KPP, PRS, CN, AAK, GL, TAT, JCM, JM, MF, JG, AK, PNH, ADH and TT. Data acquisition: KPP, PRS, CN, AAK, GJ, GT, RH, SW, TT, LC, JDG, PNH, MF, AK, NS, JN, SK, MO, MM and LM. Data analysis/interpretation: KPP, PRS, CN, AH, PNH, TAT, GL and JCM. Drafting manuscript: KPP, PRS, CN, AH, PNH, TAT, GL and JCM. Critical revision of manuscript: all authors. final approval of manuscript: all authors. All authors agree to be accountable for all aspects of this manuscript.
Funding KPP is supported by a British Heart Foundation Clinical Research Training Fellowships (FS/19/d8/34523) and has research grant from Edwards Lifesciences. PRS (FS/16/31/32185) and RH (FS/17/82/33322) are supported by British Heart Foundation Clinical Research Training Fellowships; TAT (FS/19/35/3434) and MF are supported by British Heart Foundation Intermediate fellowships. FP has received research support from Siemens Healthineers. MM has received grants and personal fees from Edwards Lifesciences and personal fees from Abbott Vascular. JCM and TAT are directly and indirectly supported by the UCLH and Barts NIHR Biomedical Research Units.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.