Article Text

Abstract
Background Treatment policy of acute rejection after heart transplantation has been changed after adopting the ISHLT endomyocardial biopsy grading system in 1991.
Objective To determine the effect of this policy change on clinical outcome after transplantation.
Methods The outcome of 147 patients who had a transplant before (early group, median follow up 96 months) and 114 patients who had a transplant after (late group, median follow up 41 months) the introduction of the ISHLT biopsy grading system was studied retrospectively. Initially “moderate rejection” according to Billingham’s conventional criteria was treated. From January 1991 grade 3A and higher was considered to require intensification of immunosuppression.
Results There were some differences between the two groups: recipients (50 v 44 years) as well as donors (28 v 24 years) were older in the “late group” and more patients of this group received early anti-T cell prophylaxis (92% v 56%). Despite more extensive use of early prophylaxis more rejection episodes were diagnosed (2.4 v1.4) and considerably more courses of rejection treatment were instituted in the late compared with the early group (3.2v 1.5). There were no deaths because of rejection in the late group, however, more infections occurred within the first year (mean 1.8 v 1.4) and more non-skin malignancies within the first 41 months were diagnosed (8 of 57 v 6 of 147, 95% CIs of difference includes 0). The incidence of graft vascular disease in the late group has been comparable to the early group until now.
Conclusion The interpretation of the ISHLT grading system resulted in lowering of the threshold for the diagnosis of rejection thereby increasing the number of rejections and subsequently the immunosuppressive load and its complications.
- transplantation
- biopsy grading system
- rejection
Statistics from Altmetric.com
The main challenge to transplant cardiologists is to keep the delicate balance between inhibition of rejection, the destructive immune response directed to the “non-self” organ, and prevention of immunosuppression related side effects.
Histological examination of endomyocardial biopsy (EMB) still is the most reliable method to detect and monitor rejection after heart transplantation. In an attempt to provide conformity in multicentre trials and publications a new, international, grading system for the histological diagnosis of acute rejection on EMB was formulated and published by a working group of the International Society for Heart and Lung Transplantation (ISHLT) in 1990.1 We adopted the ISHLT grading system and, like many others, subsequently elected to treat rejection grades 3A and higher. Our interpretation of the ISHLT system produced a shift of the threshold to intensification of immunosuppression. Before 1991 rejection treatment was instituted in cases of “moderate rejection” or more. For this we used Billingham’s conventional criteria (class 2 or higher) for which, besides interstitial mononuclear infiltrates, at least presence of hypereosinophilic myocytes with a pycnotic nucleus (myocytolysis), was considered a conditio sine qua non.2 The shift of the threshold for treating rejection was caused by accepting at least the coexistence of mononuclear infiltrates with more than one focus of myocyte damage (ISHLT 3A and higher) rather than with myocytolysis/necrosis as the indication for rejection treatment.
The purpose of this study was to determine the effect of this change in policy on clinical outcome after cardiac transplantation.
Methods
We conducted a historical comparison of two groups of heart transplant patients in whom the surgical procedure and maintenance immunosuppression were identical.
STUDY POPULATION
The study population consists of all consecutive patients who received a cardiac allograft in our institution between June 1984 and September 1995. In the early phase of the programme the upper age limit for cardiac transplant candidates was 56 years. This upper limit was abandoned early in 1990. Patients with a creatinine clearance less than 30 ml/min, patients with diabetes mellitus requiring insulin, patients with clinical signs of vascular disease outside the heart, and patients with malignancies within the past 10 years have been denied transplantation during the study period.
REJECTION SURVEILLANCE, PREVENTION, AND TREATMENT
Diagnosis of rejection was based on histological asessment of serial EMB. Biopsies were routinely performed according to the following schedule: weekly for the first six weeks after transplantation, biweekly until three months, monthly until six months, and every eight weeks for the rest of the first year. After the first year, two to three EMB specimens per year were taken. The routine EMB schedule had been approved by the medical ethical committee of the University Hospital Rotterdam and allograft recipients had given informed consent. Each EMB specimen consisted of a minimum of four individual samples. Processing of the biopsy samples consisted of fixation in 10% neutral buffered formalin followed by embedding in paraffin wax and staining with haematoxylin and eosin.
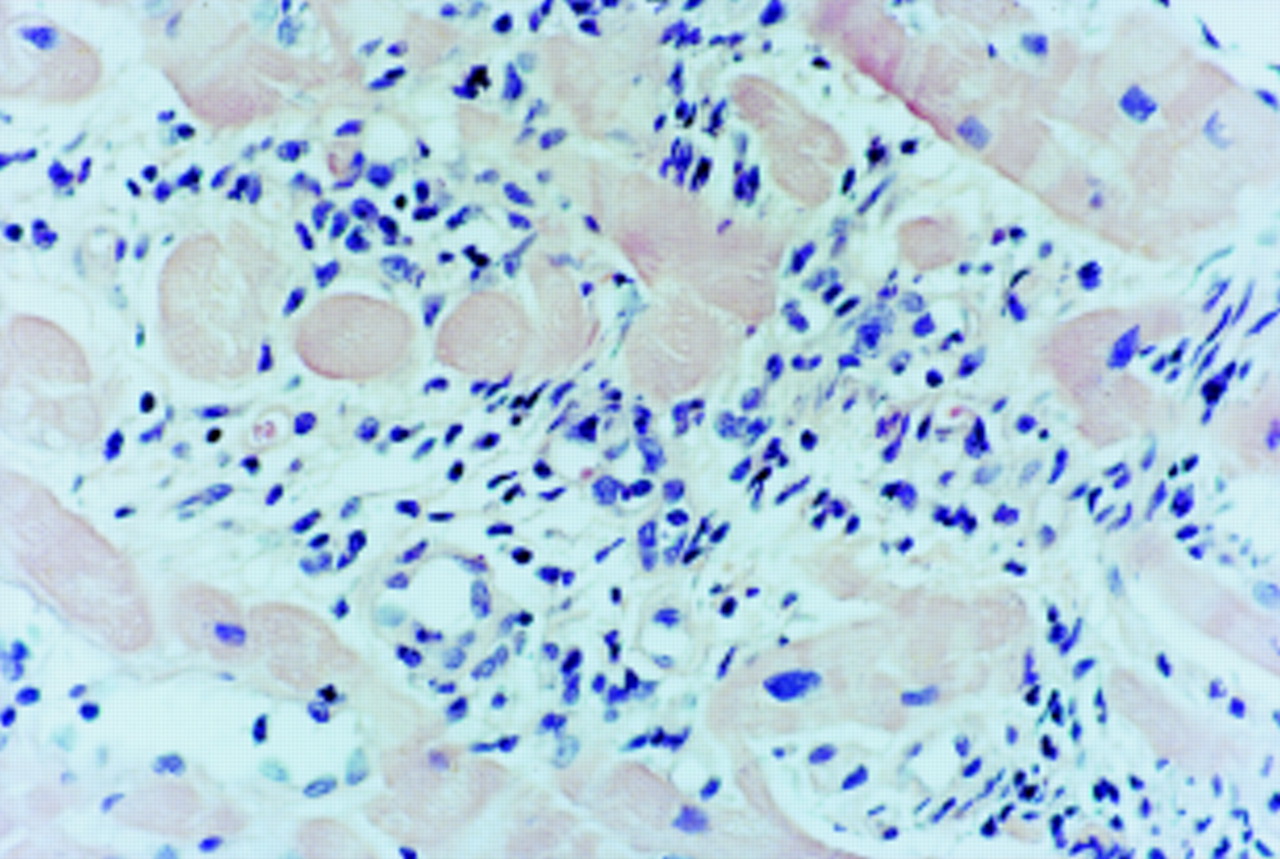
Initially, moderate rejection or more (class 2 or higher) according to Billingham’s early criteria was considered to require treatment: treatment was instituted when interstitial infiltrates at least were accompanied by myocytolysis (hypereosinophilic myocytes with a pycnotic nucleus), diagnosed on light microscopy (fig 1). Increased immunosuppression was given independent of the haemodynamic consequences of rejection. From January 1991 the presence of myocyte damage instead of myocytolysis/necrosis was considered necessary for the diagnosis of acute rejection and the line between treatment/no treatment was drawn between ISHLT grades 2 and 3A: myocyte damage was left untreated when seen within only one focus of interstitial infiltrate (grade 2) as has been shown warranted later on by others.3 Immunosuppression however was intensified from grade 3A, when at least encroachment or damage of the myocytes was visible within more foci of interstitial infiltrates (fig 2). During the whole study period EMB specimens were graded by the same pathologists in close cooperation with the same transplant cardiologists.

Endomyocardial biopsy specimen showing a pycnotic nucleus within a lytic myocyte (haematoxylin and eosin; original magnification ×20).
{kind=link}
{kind=link}
Endomyocardial biopsy specimen showing encroachment and damage of cardiac myocytes (haematoxylin and eosin; original magnification ×20).
Maintenance immunosuppression consisted of cyclosporine and low dose corticosteroids. Azathioprine was added only in cases of recurrent rejection (more than three episodes in the first year) and in patients who developed cyclosporine related severe renal failure. Different regimens of early postoperative immunosuppression have been used and evaluated in randomised trials (OKT3, 5 mg for seven days; horse-ATG for seven days; rabbit-ATG one dose of 8 mg/kg; BT563, an anti-interleukin 2 monoclonal antibody, 10 mg for seven days).4-6 Rejection was treated by methylprednisolone 1 g intravenously on three consecutive days and polyclonal (rabbit-ATG) or monoclonal (OKT3) anti-T cell antibodies in cases of persisting or frequently recurring rejection.
INFECTION
Infection was defined as a symptomatic infectious episode with concurrent demonstration of the causative agent by culture or changes in serological status. Superficial, spontaneously healing, herpes simplex I lesions of the oral mucosa, and pityriasis versicolor have been excluded from the analysis. Prevention of oral candidiasis was by local application of amphotericin-B solution during the first three weeks after transplantation. Prevention of bacterial infection was by eradication of infection preoperatively and the use of intranasal mupirocin ointment and intravenous cephalosporins perioperatively. Cytomegalovirus (CMV) seronegative recipients received blood from CMV seronegative donors and were treated prophylactically with anti-CMV hyper-immunoglobulin (Cytotect, Biotest Pharma GmbH, Dreiech, Germany) in case of a CMV seropositive donor.7 ,8 CMV infection was defined as any appearance of immunoglobulin M, isolation of CMV from urine, throat or blood or demonstration of the immediate early antigen or pp65 antigen. CMV disease was diagnosed when infection coexisted with two of the following: fever of more than 38°C for more than two days, organ involvement or leucocytopenia or thrombocytopenia. Recipients who were seronegative for Toxoplasma gondii and received the heart of a seropositive donor were treated prohylactically with spiramycine in the early phase of the programme and with pyrimethamine later on.9
GRAFT VASCULAR DISEASE
The occurrence of graft vascular disease was monitored by coronary arteriography.10 Initially, arteriography was performed annually. After analysis of sequential arteriograms of the first 119 one year survivors however, second and third year coronary arteriography was omitted in patients who had shown smooth epicardial branches on their first year arteriogram.11 Subsequently arteriography was performed each year or every two or three years depending on earlier findings. Graft vascular disease was considered present in cases of localised lesions (anything more than wall irregularities), tapering of branches or abrupt ending or disappearance of secondary or tertiary branches, or all three.
All heart transplant recipients have been followed up by transplant cardiologists of the Thoraxcenter, Rotterdam.
STATISTICAL ANALYSIS
Data are presented as mean (SD) values, medians or absolute numbers when appropriate. Group comparisons were performed using 95% confidence intervals analysis.12 The Kaplan- Meier method was used for analysis of survival rates.
Results
One hundred and forty seven patients received 148 cardiac allografts before the introduction of the ISHLT biopsy grading system and the change of our criteria for treating acute rejection. One patient underwent re-transplantation after eight months and has been assessed as two separate cases. One patient died during the operation, the 147 patients who survived the operation constitute the early group. From January 1991 to October 1995, 119 consecutive patients were operated upon, 114 of whom survived the operation (late group). Table 1shows the demographic and clinical characteristics. Because the incidence of acute rejection after the first year is very low and may be influenced by the low frequency of EMB the presented data concern the first year after transplantation only.
Characteristics of the early (before 1991) and late (after 1991) transplant patients
The late group differed slightly from the early group: recipients as well as donors were older and more patients received anti-T cell induction treatment. Inherent to a historical comparison, the follow up of the patients of the late group was shorter than of the patients of the early group (table 2). Despite the fact that 92% of the patients received early anti-T cell prophylaxis more rejection episodes were diagnosed in the late group, which resulted in considerably more courses of rejection treatment. During seven rejection episodes (in seven patients) of the early group the patient was haemodynamically compromised versus four episodes (in four patients) of the late group.
Clinical outcome of the early (before 1991) and late (after 1991) transplant patients
The increase in rejections diagnosed and treated in the late group was accompanied by more infections within the first year. CMV disease however did not occur more frequently. The incidence of infection within the total follow up period was comparable in both groups despite a much longer follow up period in the early group.
The incidence of non-skin malignancy was higher in the group with the longer follow up compared with the late group: 12% versus 7%. When considering a 41 month follow up period (the median follow up duration of the late group) there were more non-skin malignancies in the late group. However, the difference in survival free from malignancy between the early and late groups was not statistically significant. The rates at one, three, and five years were: 90%, 89%, and 82% versus 85%, 82%, and 76%, respectively. Skin malignancies occurred only in the group with the longest follow up.
The incidence of graft vascular disease, diagnosed by coronary arteriography (or by necropsy if no recent arteriogram was available) was not lower in the patients of the late group despite a higher overall immunosuppressive load.
In contrast with the early group, there were no deaths caused by acute rejection in the late group. Instead, however, three deaths were caused by infection (table 3).
Causes of death in the patients of the early (before 1991) and the late (after 1991) groups
Survival rates of the total study population were 90%, 85%, 81%, and 66% after one, three, five, and eight years, respectively. To date there are no differences in the survival rates between the patients who had a transplant before and after January 1991.
Discussion
To some extent the value of this study is limited by its retrospective nature and by the fact that two non-contemporaneous groups differing in early prophylaxis have been compared. Notwithstanding that we chose to report our findings because we consider them of interest for transplant cardiologists and pathologists. In our hands the ISHLT grading system lowered the threshold for the diagnosis of acute rejection, which cannot have been the intention of the working group. A lower threshold for the diagnosis of acute rejection resulted in a higher number of treatments for acute rejection and a decreased mortality by acute rejection on the one hand but in increased immunosuppressive load and hence its complications on the other hand.
Aiming at a lower incidence of rejection we used anti-T cell prophylaxis in several subsequent randomised trials thereby increasing the immunosuppressive load especially in most of the patients having a transplant after 1990.4-6 The immunosuppressive load of the heart transplant recipients, however, was determined mainly by courses of rejection treatment. So, lowering of the threshold for the diagnosis of rejection had considerable effects on the total immunosuppressive burden.
Myocytolysis, diagnosed on light microscopy, as a criterion for acute rejection needing additional immunosuppression has been questioned.13 Using this criterion however and considering the presence of myocytolysis a conditio sine qua non for instituting rejection treatment, the outcome of patients operated on in the early phase of our programme was excellent with 90%, 82%, and 67%, one, five, and eight year survival rates, respectively. Although much more interstitial infiltrates were accepted without treatment (when no myocytolysis/necrosis could be identified) before 1991 left ventricular function was equally good at the end of the first year compared with the function in the patients operated after 1990. In addition, left ventricular function remained good during the first five years in the patients of the early group.11 In our hands, rejection requiring treatment was diagnosed considerably more often using the presence of myocyte damage instead of myocytolysis/ necrosis as a criterion. Our interpretation of the ISHLT system must have been wrong because the ISHLT system was, as far as we know, not meant to lower the threshold for the diagnosis of acute rejection. We therefore believe that such ambiguity of guidelines aiming at conformity requires revision of the system. Furthermore, for comparison of results in multicentre trials the use of a core laboratory seems mandatory.
Other centres also questioned the usefulness of the first version of the ISHLT system.14 We now question whether we have been right to change our policy after the adoption of a new grading system. The data presented here at least do not show favourable effects: fewer deaths by rejection are compensated by a higher morbidity because of infection and a tendency to more cases of malignancy. The absence of an increased incidence of CMV disease may be explained by the use of anti-CMV hyperimmunoglobulin in CMV seronegative patients who received the heart of a seropositive donor. Longer follow up of the patients who received a transplant after 1990 will show whether death caused by malignancy in this group ultimately will surpass death by malignancy in the early group. Only a reduction of death caused by graft vascular disease eventually could compensate for that. The data up to now have encouraged us to reconsider our criteria for rejection requiring treatment.