Article Text

Abstract
Objective To compare vessel, lumen, and plaque volumes in atherosclerotic coronary lesions with inadequate compensatory enlargement versus lesions with adequate compensatory enlargement.
Design 35 angiographically significant coronary lesions were examined by intravascular ultrasound (IVUS) during motorised transducer pullback. Segments 20 mm in length were analysed using a validated automated three dimensional analysis system. IVUS was used to classify lesions as having inadequate (group I) or adequate (group II) compensatory enlargement.
Results There was no significant difference in quantitative angiographic measurements and the IVUS minimum lumen cross sectional area between groups I (n = 15) and II (n = 20). In group I, the vessel cross sectional area was 13.3 (3.0) mm2 at the lesion site and 14.4 (3.6) mm2 at the distal reference (p < 0.01), whereas in group II it was 17.5 (5.6) mm2 at the lesion site and 14.0 (6.0) mm2 at the distal reference (p < 0.001). Vessel and plaque cross sectional areas were significantly smaller in group I than in group II (13.3 (3.0)v 17.5 (5.6) mm2, p < 0.01; and 10.9 (2.8) v 15.2 (4.9) mm2, p < 0.005). Similarly, vessel and plaque volume were smaller in group I (291.0 (61.0) v 353.7 (110.0) mm3, and 177.5 (48.4) v 228.0 (92.8) mm3, p < 0.05 for both). Lumen areas and volumes were similar.
Conclusions In lesions with inadequate compensatory enlargement, both vessel and plaque volume appear to be smaller than in lesions with adequate compensatory enlargement.
- intravascular ultrasound
- ultrasonics
- remodelling
- coronary artery disease
Statistics from Altmetric.com
Intravascular ultrasound provides transmural images of coronary arteries in vivo. The coronary vascular wall, the cross sectional area of the atherosclerotic plaque, the consequences of plaque accumulation, and the mechanisms of lesion formation can be studied in humans in a manner previously not possible.1-9
Atherosclerotic arteries tend to undergo compensatory vascular enlargement to accommodate increasing plaque burden during the early stages of plaque accumulation.10-12 Because of this adaptation, lumen dimensions are preserved and an angiographic underestimation of coronary atherosclerosis often occurs.13 This concept was initially derived from anatomical and histopathological studies in vitro.10-12It has been confirmed using intravascular and epicardial ultrasound studies in vivo. 14-18 Recently, Clarksonet al 19 suggested that failure of adaptive remodelling may be an important factor for the development of significant atherosclerotic lesions. The histopathological and intravascular ultrasound data of Pasterkamp et al 20 ,21 in peripheral arteries, and intravascular ultrasound observations of Wong et al,22Nishioka et al,23 and Mintz et al 24 have also shown evidence of inadequate compensatory enlargement.
In the present study, we examined 35 atherosclerotic coronary lesions which were classified as having inadequate (group I) or adequate compensatory enlargement (group II). Automated three dimensional intravascular ultrasound analysis of the lumen, vessel, and plaque dimensions was performed25-29 to gain insight into the volumetric characteristics6 of these lesions.
Methods
PATIENT POPULATION
The study population consisted of 35 patients with primary (not restenotic) atherosclerotic lesions examined using preintervention intravascular ultrasound. Inclusion criteria were: angiography documented non-curved lesion segments; limited plaque calcification throughout a lesion length of 20 mm; absence of a complete occlusion of the stenotic lumen during the ultrasound imaging run; and absence of major side branches. Thirty two men and three women (mean (SD) age 61 (9) years) were examined. Lesions were located in the left anterior descending coronary artery (n = 20), right coronary artery (n = 10), and left circumflex coronary artery (n = 5); 32 were proximal and three were in the mid-portion. The study was approved by the Local Council on Human Research. All patients signed a written informed consent form, approved by the local medical ethics committees.
INTERVENTIONAL PROCEDURE AND INTRAVASCULAR ULTRASOUND IMAGING
The patients received 250 mg aspirin and 10 000 U heparin intravenously. If the duration of the entire catheterisation procedure exceeded one hour, the activated clotting time was measured, and intravenous heparin was given in order to maintain a clotting time of more than 300 s. Intravascular ultrasound imaging was performed after intracoronary injection of 0.2 mg glyceryl trinitrate, starting at least 10 mm distal to the lesion segment. A mechanical intravascular ultrasound system (ClearView, CardioVascular Imaging Systems, Sunnyvale, California, USA) and a sheath based imaging catheter were used. The catheter incorporated a 30 MHz bevelled, single element transducer rotating at 1800 rpm (MicroView, CardioVascular Imaging Systems). This catheter is equipped with a 2.9 F 15 cm long sonolucent distal sheath that has a common lumen that either houses the guide wire (during catheter introduction) or the transducer (during imaging after the guide wire has been pulled back), but not both. This design avoids direct contact of the imaging core with the vessel wall.29 The ultrasonic transducer was withdrawn through the stationary imaging sheath using a motorised pullback device at a constant speed of 0.5 mm/s. All intravascular ultrasound examinations were recorded on high resolution s-VHS videotape for later offline quantitative analysis. After the intravascular ultrasound examination, all patients were successfully treated by balloon angioplasty, coronary stent implantation, or directional coronary atherectomy; there were no procedural or postprocedural in hospital complications.
INTRAVASCULAR ULTRASOUND IMAGE ANALYSIS
Twenty millimeter long lesion segments (10 images/mm axial arterial length), centered on the target lesion site, were analysed off-line using a computerised intravascular ultrasound analysis system (fig 1).25-28 Reference images with the smallest plaque burden were acquired no more than 3 mm distal to the lesion segment. Cross sectional area measurements at the reference site were obtained with the computerised analysis system (single frame mode); care was taken to avoid any major side branch between the lesion segment and the reference site.

Principle of automated three dimensional intravascular ultrasound image analysis. Detection of the contours corresponding to the lumen–tissue and media–adventitia interfaces is first performed on two perpendicular longitudinal sections (A, B), reconstructed from the image data of the entire three dimensional “stack” of images. Edge information of the longitudinal contours are represented as points on the planar images, defining there the centre and range of the final contour detection process.
Cross sectional area measurements (mm2) included the lumen and vessel cross sectional area. The vessel cross sectional area was measured by tracing the border between the hypoechoic media and the echoreflective adventitia. As in many previous studies using intravascular ultrasound, the cross sectional area (and thickness) of plaque plus media was used as a measure of atherosclerotic plaque area (and thickness) because ultrasound cannot measure media thickness accurately.30 Plaque cross sectional area was calculated as vessel cross sectional area minus lumen cross sectional area. The cross sectional area plaque burden was calculated as plaque cross sectional area divided by vessel cross sectional area.
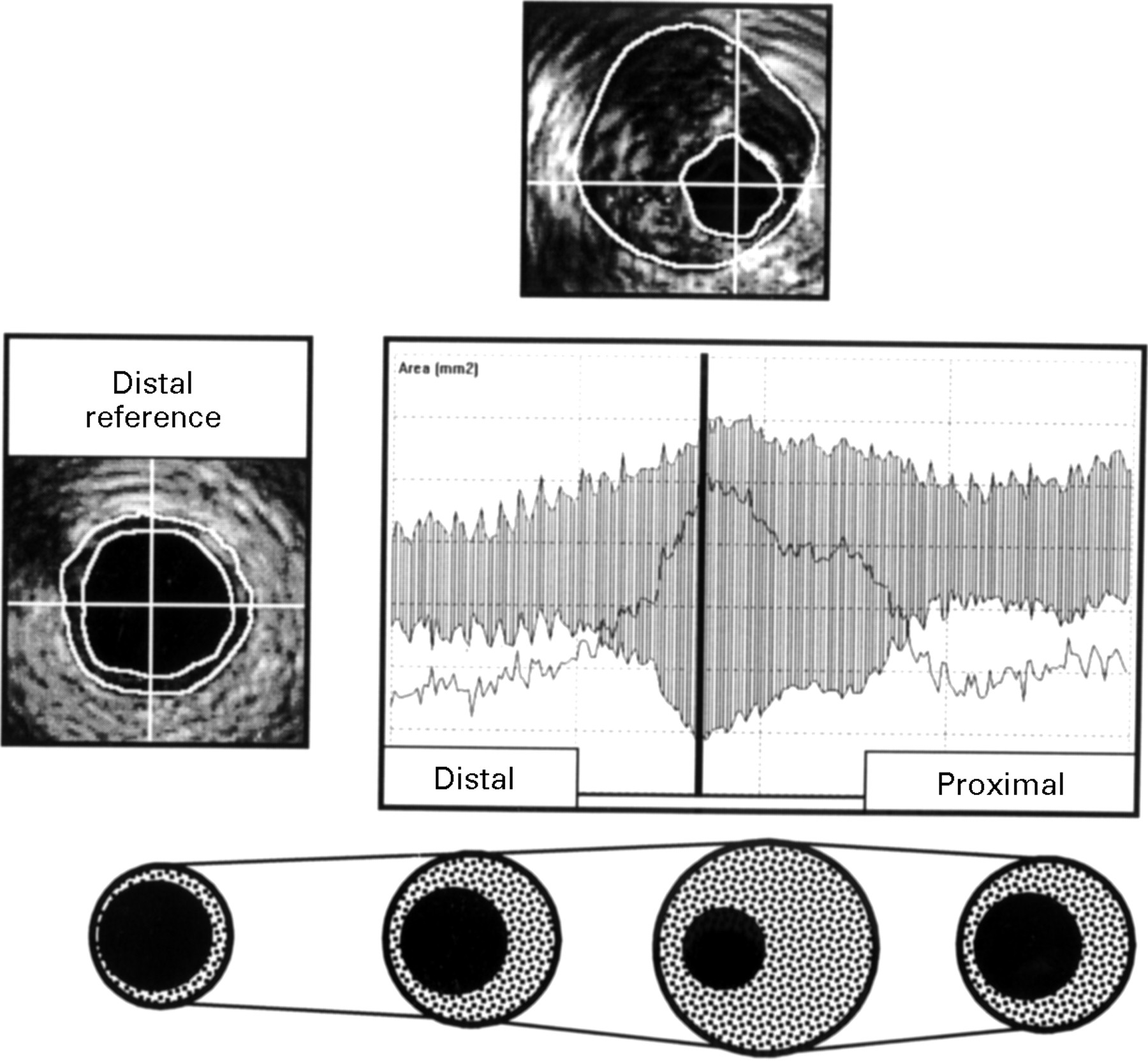
Compensatory enlargement was considered inadequate (group I) if thevessel cross sectional area at the site of the minimumlumen cross sectional area was smaller than that at the distal reference site (fig 2).23 If the vessel cross sectional area at the site of the minimum lumen cross sectional area was larger than or equal to the distal reference site (fig 3), compensatory enlargement was considered adequate (group II).

Analysis of a 20 mm long mid-right coronary segment with inadequate compensatory vascular enlargement (group I). The vessel cross sectional area is smallest at the target lesion site. Markers indicate that site on the longitudinal sections (right upper panels) and the display of the cross sectional area measurements (right lower panel). Linear functions of the vessel and lumen cross sectional area form the upper and lower boundaries of the greyish area, which represents the plaque cross sectional area. Alternatively, the values of plaque cross sectional area can be derived directly from a linear function (single black line), which here partly overlaps the greyish area.

{kind=link}
{kind=link}
{kind=link}
Adequate compensatory vascular enlargement, as observed in one of the lesion of group II. The vessel cross sectional area is larger at the target lesion site (upper panel) than at the reference site (left mid panel). The lower panel illustrates and underlines the principle of compensatory vascular enlargement.
Volume measurements (mm3) of the lumen, vessel, and plaque (based on 10 intravascular ultrasound images/mm axial arterial length) were calculated according to Simpson’s rule as
 where H = thickness of a coronary artery slice represented by a single tomographic intravascular ultrasound image, and n = number of images in the three dimensional image set. The volume plaque burden (%) was calculated as plaque volume divided by vessel volume.
where H = thickness of a coronary artery slice represented by a single tomographic intravascular ultrasound image, and n = number of images in the three dimensional image set. The volume plaque burden (%) was calculated as plaque volume divided by vessel volume.
The overall plaque eccentricity index was calculated as mean value of the eccentricity indices of all individual image slices; these were derived as previously described (minimum plaque thickness divided by maximum plaque thickness).31 A higher value of that index indicated a more concentric plaque distribution (the maximum value 1.0 would indicate perfectly concentric plaque distribution along the entire lesion segment), whereas a lower value indicated a more eccentric plaque distribution.
The overall lumen symmetry index was calculated as mean value of the lumen symmetry indices (minimum lumen diameter divided by maximum lumen diameter) of all individual image slices. A higher value of that index indicated a more symmetrical lumen shape (the maximum value 1.0 would indicate a perfectly circular lumen along the entire lesion segment).
COMPUTERISED INTRAVASCULAR ULTRASOUND ANALYSIS METHOD
The analysis was performed offline using a computerised intravascular ultrasound analysis system.25-28 The analysis system used the Windows™ (Microsoft, Redmond, Washington, USA) operating system on a personal computer. The computerised analysis required the digitisation of a stack of intravascular ultrasound images from videotape. Two longitudinal sections were automatically reconstructed (fig 1), and the contours corresponding to the lumen–tissue and media–adventitia interfaces were automatically identified. The longitudinal contours were visually checked and, if necessary, edited with computer assistance (see below). The longitudinal contours generated individual edge points on the planar images defining the centre and range of the automated boundary search on the planar images. Subsequently, contour detection of the planar images was performed. The axial location of an individual planar image (on the longitudinal contours) was indicated by a cursor; the cursor was used to scroll through the entire set of planar images while the planar contours were visually checked. Finally, the contour data of the planar images were used for the computation of the results.
Automated contour detection and computer assisted contour editing were based on the application of a minimum cost algorithm to detect the luminal and external vessel boundaries.26-28 Each digitised intravascular ultrasound image was resampled in a radial format (64 radii per image), and a cost matrix representing the edge strength was calculated from the image data. For the boundary between lumen and plaque, the cost value was defined by the spatial first derivative. For the external vessel boundary a cross correlation pattern matching process was used for the cost calculations. The path with the smallest accumulated value was determined by dynamic programming techniques.
The computer assisted editing differed considerably from conventional manual contour tracing. The computer mouse was used to indicate the correct boundary. This forced the contour through the manually entered point by assigning this point a very low value in the cost matrix. Editing the contour of a single slice caused the entire dataset to be updated (dynamic programming). Side branches with relatively small ostium and small calcified portions of the plaque were generally ignored by the algorithm as a result of its robustness, which means that the automated contour detection did not follow every abrupt change in the cost path.
This algorithm has been validated in tubular phantoms.27 A comparison between automated three dimensional intravascular ultrasound measurements in atherosclerotic coronary specimen in vitro, and morphometric measurements on the corresponding histological sections revealed good correlations (r = 0.80 to 0.94 for cross sectional area, and r = 0.83 to 0.98 for volume measurements).26 Both area and volume measurements by the automated system agreed well with results obtained by manual tracing of intravascular ultrasound images (mean differences ⩽ 3.7%; areas:r ⩾ 0.97, and volumes:r = 0.99).26 In vivo, intraobserver and interobserver comparisons of the analysis method revealed high correlations (r = 0.95 to 0.98 for area andr = 0.99 for volume) and small mean differences (⩽ 1.1%), with SD of lumen, vessel, and plaque not exceeding 7.3%, 4.5%, and 10.9% for areas, and 2.7%, 0.7%, and 2.8% for volumes, respectively.27
QUANTITATIVE CORONARY ANGIOGRAPHY
Quantitative angiographic analysis was performed off-line as previously described32 ,33 on end diastolic frames with homogeneous opacification of the coronary lumen, acquired after intracoronary application of nitrates. We used a computer based coronary angiography analysis system (CAAS, Pie Medical, Maastricht, Netherlands). The measurements were performed by an experienced analyst in at least two projections, obtained from opposite (ideally orthogonal) angiographic views without overlapping side branches or foreshortening. Briefly, automated detection of the coronary artery contours was performed on the basis of the weighted sum of the first and second derivative functions applied to the digitised brightness silhouette. The diameter function of the coronary artery lumen was determined by computing the shortest distances between the edge points of the right and left contours. The absolute angiographic diameter of the stenosis was determined using the non-tapering part of the contrast-free guiding catheter as a scaling device. The minimum lumen diameter was measured by edge detection; the interpolated reference diameter was based on a computerised estimation of the original arterial dimension at the site of the obstruction. The diameter stenosis was derived from the measured minimum luminal diameter and the interpolated reference diameter.
STATISTICAL ANALYSIS
Quantitative data are given as mean values (SD). Dichotomous variables are expressed as frequencies. Continuous variables are compared using the two tailed Student t test and linear regression analysis. Probability (p) values < 0.05 are considered statistically significant.
Results
ADAPTIVE REMODELLING STATE
Inadequate compensatory enlargement was found in 15 lesions (group I); in these cases the vessel cross sectional area at the site of the minimum lumen area was smaller than at the distal reference (13.3 (3.0) v 14.4 (3.6) mm2, p < 0.01). In the other 20 lesions (group II), the vessel cross sectional area at the minimum lumen area was larger than that at the distal reference (17.5 (5.6) v 14.0 (6.0) mm2, p < 0.001).
The patients in the two groups did not differ in age (61 (6) yearsv 62 (10) years) or sex (male: 14/15 v18/20). Lesion location was also similar for both groups: left anterior descending (9/15 v 11/20), right (5/15 v5/20), and left circumflex coronary arteries (1/15 v4/20).
PLANAR INTRAVASCULAR ULTRASOUND
Quantitative coronary angiographic measurements were similar in both groups (table 1)
Quantitative coronary angiographic measurements
QUANTITATIVE ANGIOGRAPHIC ANALYSES
Reference segment measurements were similar in both groups (table2). There was no difference in minimum lumen cross sectional area or cross sectional area plaque burden (table 2); however, both vessel and plaque cross sectional area were significantly smaller in group I (lesions with inadequate remodelling). .
Cross sectional area (CSA) measurements with intravascular ultrasound
INTRAVASCULAR ULTRASOUND VOLUMETRIC ANALYSIS
Overall, an average of 62.8(10.8)% of the vessel volume (326.9 (7.0) mm3) was filled with plaque (206.4 (80.1) mm3); this defined the volumetric plaque burden. The residual lumen volume measured 120.5 (47.2) mm3. Plaque and vessel volumes were smaller in group I than in group II (p < 0.05 for both) (table 3); there was no significant difference in lumen volume or in volumetric plaque burden.
Volumetric measurements by intravascular ultrasound
The eccentricity index (minimum plaque thickness divided by maximum plaque thickness) was significantly higher in group I than in group II (0.28 (0.07) v 0.21 (0.11), p < 0.05), indicating a more concentric plaque distribution in group I. The lumen shape was significantly more symmetrical in group I; this was shown by the higher lumen symmetry index (minimum lumen diameter divided by maximum lumen diameter) in group I (0.86 (0.02) v 0.84 (0.03), p < 0.05).
Discussion
Three dimensional intravascular ultrasound was initially used for visual assessment of the spatial configuration of plaques and dissection membranes,34-37 whereas contemporary three dimensional intravascular ultrasound systems are equipped with algorithms for computer assisted analysis of the plaque or lumen volumes and dimensions.6 ,25-29 ,33 ,38 ,39 The three dimensional intravascular ultrasound analysis system used in the current study has been extensively validated; it permits the rapid automated analysis of lumen and plaque volumes and dimensions on a large number of planar image slices.6 ,26-28
We used this three dimensional intravascular ultrasound analysis system to compare 15 lesions with inadequate compensatory enlargement to 20 lesions with adequate compensatory enlargement. Compared to lesions with adequate compensatory enlargement, lesions with inadequate compensatory enlargement had smaller plaque and vessel volumes, more concentric plaque distribution, more symmetrical lumen shapes, and similar lumen volumes and dimensions.
Importantly, lumen volumes and dimensions were similar in both groups, whether assessed by intravascular ultrasound or by quantitative coronary angiography. This emphasises the significance of intravascular ultrasound in the assessment of human atherosclerosis in vivo.
Our observations corroborate recent studies, which showed that inadequate compensatory enlargement may contribute to the development of significant luminal narrowing.19-25 In these previous studies, despite intracoronary injection of nitrates before the ultrasound examination, local vasospastic activity could not be excluded23; and a collapse of the coronary artery could have resulted from a decrease in coronary arterial pressure, attributable to subtotal occlusion of the residual lumen during the ultrasound imaging run. However, neither local vasospasm nor collapse of the coronary artery can explain the significantly smaller vessel and plaque volumes of lesions with inadequate compensatory enlargement, as observed in the current study.
LIMITATIONS AND POTENTIAL SOURCES OF ERROR
As all previous studies of the natural history of coronary atherosclerosis in human were performed at a single point in time, the time course and magnitude of vascular response to plaque growth remains unknown.
Imaging with intravascular ultrasound can be hampered by eccentric catheter position, non-uniform transducer rotation, and non-coaxial catheter position.
As the external vascular boundary cannot be seen in the acoustic shadow behind calcium, we did not include lesions with severe plaque calcification. As in all studies with intravascular ultrasound, intracoronary injections of nitrates were performed before the ultrasound examination to prevent vasospasm; no angiographic changes before and after the intravascular ultrasound imaging procedure were observed, but this does not exclude local vasospastic activity.
Linear three dimensional systems, as used in the current study, provide approximate volumetric indices because they do not account for the presence of vascular curvatures.28 ,29 ,40 In the current study, only relatively straight coronary segments on the angiogram were included to minimise the curve induced error in the volume calculation. Approaches that combine data obtained from angiography and intravascular ultrasound can provide information on the real spatial geometry of the vessel, but these sophisticated techniques are still subject to refinement and ongoing research.29
CONCLUSIONS
Planar intravascular ultrasound analysis identified a population of coronary artery lesions with inadequate compensatory vascular enlargement. Volumetric intravascular ultrasound analysis showed that these lesions have less atherosclerotic plaque. Serial intravascular ultrasound studies will be required to determine whether the adaptive remodelling state of atherosclerotic lesions has any implication for the success of catheter based or pharmacological treatment strategies.
Acknowledgments
CvB is the recipient of a fellowship of the German Research Society (DFG, Bonn, Germany).