Article Text

Abstract
Objective To compare the predictive value of dobutamine echocardiography (DE) and positron emission tomography (PET) in identifying reversible chronic left ventricular (LV) dysfunction (hibernating myocardium) in patients with coronary artery disease (CAD) and overt heart failure.
Patients 30 patients (four women) with CAD and heart failure undergoing coronary artery bypass grafting (CABG).
Methods Myocardial viability was assessed with DE (5 and 10 μg/kg/min) and PET with [18F] 2-fluoro-2-deoxy-D-glucose (FDG) under hyperinsulinaemic euglycaemic clamp. Regional (echo) and global LV function (MUGA) were assessed at baseline and six months after CABG.
Results 192 of the 336 (57%) dysfunctional LV segments improved function following CABG (hibernating) and the LV ejection fraction (EF) increased from 23(7) to 32(9)% (p < 0.0001) (in 17 patients > 5%). DE and PET had similar positive predictive values (68% and 66%) in the identification of hibernating myocardium, but DE had a significantly lower negative predictive value than PET (54% v 96%; p < 0.0001). A significant linear correlation was found between the number of PET viable segments and the changes in EF following CABG (r = 0.65; p = 0.0001). Stepwise logistic regression identified the number of PET viable segments as an independent predictor of improvement in EF > 5%, whereas the number of DE viable segments, the baseline LVEF, and wall motion were not.
Conclusions DE has a higher false negative rate than PET in identifying recoverable LV dysfunction in patients with severe postischaemic heart failure. The amount of PET viable myocardium correlates with the functional outcome following CABG.
- dobutamine echocardiography
- positron emission tomography
- coronary artery disease
- heart failure
- hibernating myocardium
Statistics from Altmetric.com
- dobutamine echocardiography
- positron emission tomography
- coronary artery disease
- heart failure
- hibernating myocardium
In patients with coronary artery disease (CAD), dysfunctional left ventricular (LV) segments subtended by a stenotic coronary artery can recover contractile function following revascularisation and this myocardium has been defined as hibernating.1 ,2 The revascularisation of hibernating myocardium is associated with improvement in LV function3 ,4 in patients with CAD, and recent studies have suggested that patients with non-revascularised hibernating myocardium have a propensity to suffer adverse cardiac events.5 ,6 The condition of myocardial hibernation raises the possibility that patients with severe LV impairment and heart failure may benefit from revascularisation and the correct preoperative identification of recoverable LV dysfunction may reduce their risk of surgery.7
The presence of hibernating myocardium can be predicted by non-invasive imaging techniques such as positron emission tomography (PET) with [18F] 2-fluoro-2-deoxy-D-glucose (FDG), thallium-201 scintigraphy, and dobutamine echocardiography (DE). These methods probe different mechanisms associated with cellular viability such as preserved myocardial uptake of exogenous glucose for PET, sarcolemmal integrity for thallium-201, and the presence of inotropic contractile reserve on stimulation of β adrenoceptors for DE.8 DE is usually the initial approach for the identification of hibernating myocardium because it is inexpensive, widely available, and has a good predictive value.9 However, there is some evidence that in severely dysfunctional myocardium DE yields a lower negative predictive value (higher false negative rate) than PET or thallium-201 scintigraphy.10-14 Thus, patients with heart failure and hibernating myocardium might be missed by DE and denied the potential benefits of revascularisation.
This study aimed at comparing the predictive value of DE and PET in identifying hibernating myocardium in patients with chronic CAD and severe LV dysfunction resulting in overt heart failure.
Methods
PATIENTS
The study population was 30 patients (four women, mean (SD) age 57 (7) years, with multivessel CAD and stable chronic heart failure (New York Heart Association (NYHA) class ⩾ III). These patients were part of a study investigating the role of CABG in postischaemic heart failure in which patients with angina (irrespectively of the demonstration of viability) and those without angina but with significant viability underwent CABG, and patients with no angina or exercise inducible ischaemia and no evidence of viable myocardium (both at PET and DE) were excluded.15 All patients were in sinus rhythm and had suffered at least one (range 1–3) Q wave myocardial infarction a mean (SD) of 30 (14) months (range 12–60) before the study. Nine patients had mild effort angina. Seven patients were diabetic and five hypertensive. Patients were receiving treatment with angiotensin converting enzyme (ACE) inhibitors (25), diuretics (18), digoxin (7), nitrates (7), and calcium channel blockers (3). No patient was on β blockers. All medical treatment was withdrawn on the study day both at baseline and follow up. The radionuclide LV ejection fraction (EF) was 25(7)% (range 10–37%). Table 1 shows the baseline characteristics of the patient population.
Patient characteristics
The study was approved by the local ethics committee and written informed consent was obtained from all the patients. The radiation exposure was licensed by the UK Administration of Radioactive Substances Advisory Committee (ARSAC).
STUDY PROTOCOL
All patients had assessment of viability before CABG with PET and DE, and assessment of regional and global LV function before and six months after CABG.
Assessment of LV function
MUGA—All patients underwent radionuclide ventriculography16 for the assessment of LVEF. Briefly, after red blood cells had been labelled in vivo with 740 MBq of technetium-99m sodium pertechnetate, the intracardiac blood pool was imaged using a γ camera (Siemens LEM+, Munich, Germany) equipped with a low energy all purpose collimator and interfaced with a dedicated computer system (Nuclear Diagnostics, Gravesend, UK). Data for each cardiac cycle, synchronised to the R wave on the electrocardiogram, were divided into 32 frames. Six million counts for each view were acquired. Planar blood pool imaging was performed in the left anterior oblique projection with up to a 20° caudal tilt (best septal separation). The analysis was performed by two experienced, independent physicians who were blinded to all clinical details including the preoperative or postoperative status. The analysis was performed using a commercially available computer program (Hermes Gated Heart Analysis FUGA, Nuclear Diagnostics), which automatically allocates a region for background subtraction. In each case the position of such a region was checked and relocated appropriately (away from cardiac chambers or great vessels) when necessary. The interobserver and intraobserver agreement was assessed in a random subset of 10 patients using the method described by Bland and Altman.17 The mean (SD) of the differences in LVEF was 0.05(1.5)% points and the 95% confidence intervals (CI) were −2.9% to 3%.
Transthoracic echocardiography—Segmental LV wall motion was assessed by transthoracic echocardiography (HP Sonos 2500, Hewlett Packard, Andover, Massachusetts, USA) according to the recommendations of the American Society of Echocardiography.18 To circumvent the problem of postoperative paradoxical septal movement, wall thickening was used primarily for the assessment of septal segments. The wall motion was graded as 1 (normal), 2 (hypokinetic), 3 (akinetic), or 4 (dyskinetic). The wall motion score index (WMSI) was calculated as the sum of the scores of the left ventricular segments divided by the number of segments evaluated.18 A segment was considered as recovering contractile function following CABG if there was a reduction of at least 1 point in the wall motion/systolic thickening score.
Assessment of myocardial viability
Dobutamine echocardiography—After the baseline echocardiographic study, dobutamine infusion was started at 5 μg/kg/min for five minutes and increased to 10 μg/kg/min for an additional five minutes. Echocardiographic undigitised images for preoperative and postoperative wall motion and for the dobutamine study were analysed off-line from the videotape playback by continuous display by two independent operators unaware of all the clinical details of the patients. A dysfunctional LV segment was considered viable if infusion of dobutamine at 5 or 10 μg/kg/min resulted either in improvement of wall motion/thickening of at least 1 point (inotropic contractile reserve) or deterioration of at least 1 point (ischaemia). In a random subset of 10 patients (160 segments), the interobserver and intraobserver agreements were assessed using the κ agreement test: interobserver κ = 0.82 (95% CI 0.69 to 0.95); intraobserver κ = 0.90 (95% CI 0.80 to 1.00).
PET-FDG—Measurement of the rate of myocardial glucose utilisation (MRG) was carried out during hyperinsulinaemic euglycaemic clamp as described previously.19 Briefly, MRG was measured with the glucose analogue FDG, 185 MBq of which were infused intravenously over two minutes. A 36-frame dynamic PET scan was performed over 65 minutes. Sinograms were corrected for tissue attenuation and reconstructed by computer using standard reconstruction algorithms. Images were re-sliced in the short axis view and the LV was divided into basal, mid, and apical regions. To define 16 LV segments in the PET images, comparable to the ones used for the echo analysis,18 a radial divider comprising eight angular sectors of 45° each, was superimposed on the short axis images and centred in the left ventricular cavity. The basal and mid-LV portions were divided into six segments (anterior and posterior septum, anterior, lateral, posterior, and inferior) and the apical portion was divided into four segments (anterior, lateral, inferior, and septum). A dysfunctional segment (hypokinetic or akinetic at echocardiography) was considered viable if the FDG uptake was ⩾ 0.25 μmol/min/g—that is, the mean myocardial tracer uptake minus 1 SD measured in normally contracting regions as reported previously.19 ,20
CABG
Surgery was performed by one surgeon using cardiopulmonary bypass, mild hypothermia (32–34°C), and intermittent ischaemic arrest. The median number of grafts was three (range 1–5), the cardiopulmonary bypass time was 51 (14) minutes and the aortic clamp time 25 (6) minutes.
STATISTICAL ANALYSIS
The analysis was performed using a commercially available computer program (Arcus Quickstat; Research Solution, Cambridge, UK). Continuous data were expressed as mean (1 SD). Positive and negative predictive values, sensitivity, specificity, and accuracy were based on standard definitions.21 Comparison of paired data was made with the paired t test. Categorical data were compared with the χ2 or Fisher’s exact test as appropriate. Simple linear regression analysis with Pearson’s correlation coefficient was performed to investigate the relation between two continuous variables. Improvement in global LV function was defined as an increase of > 5% points in LVEF,4 ,22 a value that constitutes the recognised variability in calculating EF with radionuclide ventriculography. Stepwise logistic regression analysis was performed to identify independent predictors of functional LV recovery. A backward-stepwise algorithm was used. Receiver operator characteristics (ROC) curve was derived according to the method described by Metz.21 When comparing ROC curves the area under the curve was used as the discriminator.21 A p value < 0.05 was considered significant.
Results
BASELINE CHARACTERISTICS
Of 480 LV segments, 27 (5.6%) could not be assessed by either PET (13 segments) or DE (14 segments). Of the 453 segments assessed by both techniques, 28 were subtended by a normal and 425 by a stenotic (> 70%) coronary artery that was revascularised. Of these 425 segments, 89 (21%) had normal baseline wall motion and 336 (79%) were dysfunctional (180 hypokinetic and 156 akinetic). The mean number of dysfunctional segments for each patient was 11 (3) (range 7–15). The baseline LVEF was 25(7)% and the WMSI was 2.18 (0.3).
FUNCTIONAL OUTCOME
Six months after CABG there was an improvement in NYHA class in all patients (table 1), there was no recurrent angina, and no patient required hospitalisation for heart failure. To minimise the effects of medical treatment on the results, the heart failure medications (ACE inhibitors restarted three to seven days after CABG) were maintained unchanged throughout the study period with the exception of diuretics, the dose of which was reduced in eight patients. Antianginal medications were withdrawn at the time of CABG and no patient required antianginal treatment during follow up.
One patient was excluded from follow up radionuclide ventriculography as he manifested a predominant ventricular paced rhythm. In the remaining 29 patients LVEF increased to 32(9)% (p < 0.0001 vbaseline). Of the 336 dysfunctional segments, 192 (57%) (91 hypokinetic and 101 akinetic) improved function of at lest 1 point, 141 were unchanged (42%), and 3 deteriorated (1%). The WMSI improved to 1.7 (0.3) (p < 0.0001 v baseline). A significant linear correlation was found between the number of dysfunctional segments improving wall motion (hibernating myocardium) in each patient and the changes in LVEF (r = 0.76, p < 0.0001) and between the reduction (improvement) in WMSI and the changes in LVEF (r = −71, p < 0.0001).
MYOCARDIAL VIABILITY
PET
Blood glucose concentration measured before the beginning of the hyperinsulinaemic euglycaemic clamp was 6.27 (2.6) mmol/l (range 4–14), and 5.0 (1.8) (range 3–10) during clamp (p < 0.0001). Plasma insulin concentration was 13 (10) mU/l at baseline, and 70 (27) during clamp (p < 0.0001). The MRG for all dysfunctional segments was 0.41 (0.16) μmol/g/min (range 0.05–1.0). The MRG was significantly higher in hypokinetic (0.43 (0.16)) than in akinetic (0.38 (0.15)) segments (p = 0.002). A total of 286 (85%) dysfunctional segments were PET viable—that is, had MRG ⩾ 0.25 μmol/min/g. Viability was detected in 167/180 (93%) hypokinetic and in 123/156 (79%) akinetic segments (p = 0.004). The mean number of PET viable segments for each patient was 9 (4) (range 0–15).
Dobutamine echocardiography
During the DE study, the mean (SD) patients’ heart rate was 86 (10) beats/min at baseline and 99 (12) at peak dobutamine infusion (p < 0.0001). Systolic blood pressure was 116 (14) mm Hg at baseline and 119 (11) at peak infusion (NS). Rate–pressure product was 10 081 (1640) at baseline and 11 756 (2081) at peak infusion (p < 0.0001). Five patients developed ventricular bigemini rhythm at dobutamine infusion of 10 μg/kg/min. A total of 171 (51%) dysfunctional segments were DE viable (166 manifesting inotropic contractile reserve and 5 ischaemia). Viability was detected in 104/180 (57%) hypokinetic and 67/156 (43%) akinetic segments (p = 0.009). The mean number of DE viable segments per patient was 6 (3) (range 0–11) (p = 0.0002 v PET).
PREDICTION OF LV FUNCTIONAL RECOVERY
Segment by segment analysis
PET—Of the 286 PET viable segments, 190 improved function following CABG (positive predictive value 66%) and of the 50 deemed non-viable, two improved function (negative predictive value 96%). Ninety one of the 163 hypokinetic PET viable segments improved function (positive predictive value 56%) compared with 99 of the 124 PET viable akinetic (positive predictive value 80%, p < 0.0001v hypokinetic) (fig 1). None of the 17 hypokinetic non-viable segments improved function (negative predictive value 100%) compared with two of the 32 akinetic non-viable segments (negative predictive value 94%, NS) (fig 1). A significant linear correlation was found between the number of dysfunctional PET viable segments in each patient and the changes in LVEF (r = 0.65, p = 0.0001) (fig 2).

(A) Positive and (B) negative predictive values of PET and DE in hypokinetic (Hypo) and akinetic (Aki) left ventricular segments. Note in particular that the negative predictive value of DE decreases in the more dysfunctional segments.

Linear relation between the number of PET viable left ventricular segments and the changes in left ventricular ejection fraction (δ-EF) following coronary revascularisation.
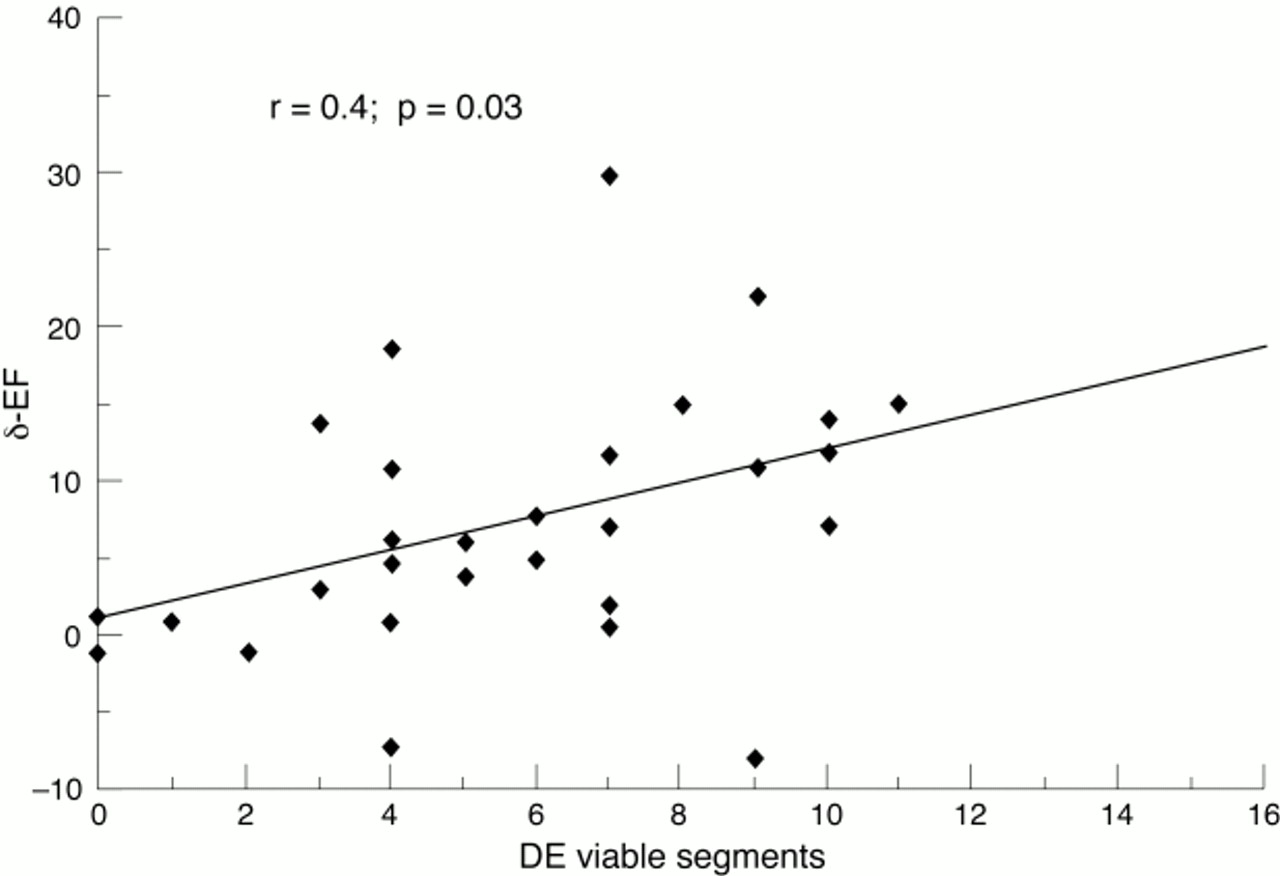
Dobutamine echocardiography—Of the 171 DE viable segments 117 improved function following CABG (positive predictive value 68%, NS v PET) and of the 165 segments deemed non-viable 75 improved function (negative predictive value 54%, p < 0.0001 v PET). Sixty two of the 104 hypokinetic viable segments improved function (positive predictive value 60%) compared with 49 of 67 akinetic segments (positive predictive value 73%, NS) (fig 1). Twenty nine of the 76 DE non-viable hypokinetic segments improved function (negative predictive value 62%), compared with 52 of 89 akinetic segments (negative predictive value 41%, p = 0.01) (fig 1). A weak but significant correlation was found between the number of dysfunctional DE viable segments in each patient and the changes in LVEF (r = 0.39, p = 0.03) (fig 3). Figure 4 shows the sensitivity, specificity, and accuracy of PET and DE.

Linear relation between the number of dobutamine viable (DE) left ventricular segments and the changes in left ventricular ejection fraction (δ-EF) following coronary revascularisation.

Comparison of overall sensitivity, specificity, and accuracy of PET and DE.
Patient by patient analysis
Patients were prospectively divided into two groups: group A (17 patients) in whom there was an increase in LVEF > 5% points (mean 13(6)% points), and group B (12 patients) in whom there was an increase in LVEF ⩽ 5% points or a deterioration. Patients in group A had a higher incidence of viable dysfunctional segments compared with group B both at PET, (12(3) v 6(4); p < 0.05) and DE (7(3) v 4(3); p < 0.05). Stepwise logistic regression identified the number of PET viable segments as the only predictor of increase in LVEF > 5% points (p = 0.005) whereas the number of DE viable segments, baseline WMSI, and baseline LVEF were not predictive. To determine the number of PET and DE viable segments in each patient required to obtain an improvement of > 5% points in LVEF, ROC analysis was performed. This identified eight segments as the best discriminator for PET (sensitivity 88%, specificity 75%, area under the curve 75%) and seven segments for DE (sensitivity 47% specificity 91%, area under the curve 0.69) (fig 5). By using these as cut off points to identify patients likely to have an improvement in LVEF, retrospective analysis demonstrated that PET had identified 15 and DE had identified 8 of the 17 patients with LVEF increase > 5% points (p = 0.02).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
ROC curves demonstrating the sensitivity-specificity pairs for the number of PET viable (solid line) and DE viable (broken line) segments required to obtain improvements in LVEF > 5% points following CABG. The arrows indicate the operator point for each test associated with the best trade-off between sensitivity and specificity. This was eight for PET (sensitivity 0.88, specificity 0.75) and seven for DE (sensitivity 0.47, specificity 0.91). Note the better performance of PET (area under the curve 0.75) compared with DE (area under the curve 0.69).
Discussion
In the present study the positive predictive values of PET and DE were comparable, although our figures are lower than those reported by others.9 The latter finding could be explained by a number of factors. We studied patients with multiple vessel CAD, severe dysfunction in most LV segments, evidence of Q wave myocardial infarction, and symptoms of heart failure. There was a high incidence of akinetic segments (46% of all dysfunctional segments), which may have more fibrosis, cellular dedifferentiation, and loss of contractile elements23 ,24 than less dysfunctional myocardium. It is possible, therefore, that such segments may require longer times for functional recovery following revascularisation25 and our single postoperative study at six months may have underestimated the amount of recoverable LV dysfunction. In studies where only patients with severe impairment of LVEF were considered,4 the positive predictive value of PET was comparable to that found in the present study. The spatial resolution of current PET scanners precludes the assessment of the distribution of a given tracer across the LV wall and it is possible that regions with significant degrees of subendocardial scarring may still show viability with no prospect of recovery of resting contractile function.26 In addition, we assessed only the improvement in resting LV function, and it is possible that viable segments not improving resting contractile function may still contribute to the LV function during stress.27 Finally, functional recovery following revascularisation may be influenced by both loading conditions and factors influencing coronary flow reserve such as recurrence of stenosis in native vessels and graft patency, which were not addressed in our study.
A significant number of dysfunctional LV segments manifested preserved glucose uptake but did not improve function, thus contributing to the overestimation of viability (low specificity) by PET. This could be explained by the fact that some myocardial regions may retain islands of viable myocardium, but are intermixed with significant amounts of fibrosis and will not improve function after revascularisation. However, in our study the amount of PET viable myocardium in each patient correlated with the improvement in LVEF. Furthermore, even in the absence of improved contractile function, the revascularisation of viable dysfunctional myocardium may attenuate remodelling and LV dilatation, may reduce the propensity to arrhythmia, and may even convey a prognostic benefit.5 ,7 ,27-29
Importantly in this study a significant number of “truly hibernating” myocardial segments (39% of all recovering segments) did not exhibit inotropic contractile reserve but manifested preserved exogenous glucose uptake, thus the negative predictive value of PET was significantly higher than that of DE. This suggests that in these hibernating segments, while the response to inotropic stimulation was lost, other basic cellular functions involved in FDG uptake and phosphorylation by hexokinase were preserved.30 In addition, the negative predictive value of DE decreased significantly in the more dysfunctional segments (akinetic vhypokinetic) and this finding is in agreement with other studies comparing DE with nuclear techniques.10 ,12 ,31 ,32 Other workers have reported that the overall predictive accuracy of DE in identifying hibernating myocardium appears comparable to that of nuclear imaging techniques9; however, the severity of regional and global LV dysfunction appears to reduce the diagnostic accuracy of DE.12-14 The presence of viable dysfunctional myocardium constitutes an unstable substrate for further cardiac events6 and its revascularisation may improve the outcome of patients with severe LV impairment.6 ,7 ,28 Thus the underestimation of viability by DE may lead to overlooking patients who might benefit from coronary artery revascularisation.
In patients with severe LV dysfunction and heart failure the lack of response to dobutamine stimulation, despite preserved glucose uptake in myocardium that recovers function following CABG, could be explained by one of the following: (1) the severity of cardiomyocyte alterations (loss and damage of myofibrils and increase in interstitial fibrosis); (2) the extent of impairment of coronary flow reserve; (3) the downregulation of β receptors in patients with severe heart failure.9 ,14 ,23 ,24 ,33 ,34
Severe damage and loss of myofibrillar components and increase in interstitial fibrosis have been demonstrated in patients in whom contractile function improved after coronary revascularisation.23 ,34 ,35 These changes may be more pronounced in more dysfunctional myocardial segments and could correlate with the lack of contractile reserve on dobutamine stimulation.34 Hibernating myocardium is characterised by an impaired coronary vasodilator reserve,36 and under these circumstances even the smallest increase in oxygen requirement, such as that demanded by low dose dobutamine infusion, could not be met in some patients,9 thus resulting in ischaemia and inability to increase contractile function.9 ,37 Finally, patients with severe LV dysfunction and heart failure undergo neurohormonal changes that result in downregulation of myocardial β1 adrenoreceptors33 and this could potentially reduce the myocardial sensitivity to dobutamine response.
CLINICAL IMPLICATIONS
Because global LV function is an important prognostic indicator in patients with ischaemic heart failure,38 we sought to identify the predictors of meaningful improvements in LVEF on a patient by patient basis. The amount of PET viable myocardium was the only independent predictor of improvement in LVEF > 5% points. DE missed nine (patients with < 7 DE viable segments) of the 17 patients who had significantly improved LVEF and eight of these patients were correctly identified by PET (had > 8 PET viable segments). However, eight of the nine patients with significant viability (> 7 segments) at DE had a significant improvement in LVEF. On the basis of these results we propose a strategy for the investigations of patients with postischaemic heart failure and CAD amenable to CABG. DE should be used as the first screening test for the presence of significant viability. However, because of the high false negative rate shown by this technique, PET should be performed in patients with negative DE. As the number of patients studied is relatively small, the indications provided by our study should be interpreted with the necessary caution. Finally, both DE and PET indicated that a significant mass of viable myocardium is required to achieve a significant improvement in LVEF following CABG. This finding underlines the importance of accurate preoperative assessment of viability particularly in patients with very poor LV function who have the highest perioperative risk.39
STUDY LIMITATIONS
We used a low dose dobutamine protocol and higher doses may have unveiled more ischaemia, which has been shown to be a strong predictor of recovery of function.40 Despite achieving a significant increase in the patient’s heart rate and rate–pressure product, which are determinants of myocardial oxygen demand, we detected ischaemia in five of 336 (1.5%) dysfunctional segments. However, the 5 and 10 μg/kg/min protocol adopted in our study is widely used12 ,18 ,22 ,41 thus allowing meaningful comparison of results. One study comparing different doses of dobutamine40 demonstrated that most (94%) dysfunctional segments manifesting biphasic response at dosages > 10μg/kg/min demonstrate contractile reserve at dosages between 5 and 7.5 μg/kg/min. Finally, there was a high incidence of complications with dobutamine at 10 μg/kg/min—17% of patients developed significant ventricular arrhythmias.
We did not use a digitised technique for the analysis of the echo images and this could have led us to overlook subtle changes in wall motion during dobutamine infusion. However, the diagnostic accuracy of the digitised analysis appears comparable to that of the videotape approach.42
The impact of revascularisation of viable myocardium on long term prognosis was not addressed by this study, and therefore indications on the appropriate treatment of patients with postischaemic heart failure cannot be extrapolated from our results. However, LVEF has been demonstrated to be a strong prognostic determinant in patients with CAD and heart failure and it could be that its improvement may be associated with prognostic benefits.
Acknowledgments
This paper was presented at the American College of Cardiology meeting, Anaheim, California, USA, 16–19 March 1997.
D Pagano is supported by a Sheldon Clinical Research Fellowship of the West Midlands Health Authority. The authors express their gratitude to Miss T Ryan for the acquisition of the echocardiograms, to the staff of the Nuclear Medicine Department of the Queen Elizabeth Hospital for the acquisition and analysis of the radionuclide ventriculography tests, to Dr P Jordan and Dr M Pitt for their help in the analysis of the echo images, to the radiochemists and the radiographers of the MRC Cyclotron Unit for their help in the acquisition of the positron emission tomography data. Special thanks to Ms H Boyd for the help and expertise in the analysis of the PET data and to Dr P Davies from the school of Mathematics and Statistics of the University of Birmingham for advise in the statistical analysis of the data.