Article Text

Abstract
Torsade de pointes in the congenital long QT syndrome (LQTS) is often pause dependent. Thus, the main goal of pacemaker treatment in the LQTS may be the prevention of pauses that facilitate the onset of torsade de pointes. A pause prevention pacing algorithm (rate smoothing) was used for arrhythmia prevention in a 14 year old girl with congenital LQTS. By temporarily increasing the pacing rate after spontaneous premature beats, rate smoothing down of 18% prevented postextrasystolic pauses, pause related T-U changes, and recurrence of pause induced torsade de pointes. Rate smoothing is a potentially useful tool that ought to be evaluated for the prevention of torsade de pointes in the LQTS.
- long QT syndrome
- torsade de pointes
- ventricular fibrillation
- ventricular tachycardia
- pacing
Statistics from Altmetric.com
Permanent pacing, in conjunction with β blockers is an established mode of treatment for patients with the congenital long QT syndrome (LQTS).1-3 However, the mechanism underlying the beneficial effects of cardiac pacing and the optimal pacing modality are not fully understood. Indeed, syncope and sudden death have been reported despite combined β blocker and pacemaker treatment.3
We recently showed that torsade de pointes in the congenital LQTS is often pause dependent.4 Our data suggest that the main goal of pacemaker treatment in the LQTS is the prevention of pauses that facilitate the onset of torsade de pointes. We describe the use of a pause prevention pacing algorithm for arrhythmia prevention in a young patient with congenital LQTS and documented pause dependent torsade de pointes.
Case report
A 14 year old girl was hospitalised for abdominal surgery (choledochal cyst). On the night before the scheduled hospital discharge, several episodes of syncope and seizures occurred. Torsade de pointes was documented during one syncopal episode and the patient was transferred to our department. Her past medical history was unremarkable, but there was a history of recurrent seizures and sudden death in a maternal aunt and a maternal uncle at age 38 and 52 years, respectively. Cardiac examination, echocardiography, and blood tests were normal (except for transient increase in liver enzymes). Electrocardiogram showed R-R, QT, and QTc intervals of 720, 460, and 542 ms, respectively. The estimated QT score was 5.5 points, suggesting a high probability of LQTS.5
Despite treatment with intravenous and oral β blockers, lidocaine, diazepam, potassium, and magnesium, recurrent episodes of torsade de pointes occurred. The episodes were invariably pause dependent (fig 1). Therefore, a temporary pacing electrode was placed transvenously in the right ventricle and VVI pacing at 100 beats/min was initiated. During the following week, the patient remained free from sustained arrhythmias. However, despite treatment with atenolol (200 mg daily), multiple extrasystoles and occasional short bursts of torsade de pointes occurred whenever the pacing rate was decreased to 80 beats/min or when loss of capture occurred during estimation of ventricular pacing threshold. A permanent pacemaker with a rate smoothing algorithm was implanted.

Representative example of pause dependent torsade de pointes. The R-R intervals (shown in milliseconds) gradually increase due to sinus arrhythmia until a sinus cycle of 790 ms is followed by the first premature depolarisation. This extrasystole generates a longer pause (a postextrasystolic pause of 960 ms), which is followed by a sinus complex with postextrasystolic U wave augmentation (arrow) and a new premature depolarisation. The long–short sequence is perpetuated, leading to longer and faster runs of torsade de pointes. Fortuitously, the longest run is followed by a relatively short sinus cycle (arrowhead) and the vicious cycle (long–short sequence) terminates.
Methods
Rate smoothing is a pacing algorithm that prevents sudden changes in paced heart rhythm. When rate smoothing is programmed on, each R-R interval (whether sensed or paced) is taken as reference value and the next R-R cannot vary by more than the programmed percentage from the reference. Rate smoothing down and rate smoothingup, which may be programmed independently, dictate the maximal increment and decrement possible in successive R-R intervals, respectively.
We implanted a DDDR permanent pacemaker (Vigor DR 1230; Cardiac Pacemakers Inc, St Paul, Minnesota, USA). Rate smoothing up was programmed off and rate smoothing down was programmed on with values of 15–18%. These values were selected based on: the coupling interval of recorded spontaneous extrasystoles (which on multiple occasions initiated short–long sequences culminating in torsade de pointes); and the QT interval of the extrasystoles. Lower values were not used because rate smoothing down of less than 10% would lead to ventricular pacing that was too close to the T wave of the preceding extrasystole. Such aggressive pacing could, in theory, provoke polymorphic ventricular arrhythmias.6 When rate smoothing down values of more than 20% were used, the intervals that followed spontaneous extrasystoles were long, postextrasystolic U wave changes were not prevented, and further arrhythmias were triggered. An upper rate limit of 120 beats/min was programmed. This relatively slow rate limit was selected to limit the rate of pacing triggered by rate smoothing down in the event of spontaneous ventricular couplets or triplets.
Rate smoothing down of 18% dictates that whenever a spontaneous extrasystole occurs, regardless of the programmed lower rate limit, a few beats of relatively fast pacing will occur. The first paced interval will be 18% longer than the coupling interval of the extrasystole. Successive paced intervals will increase by 18% until the lower rate limit is reached or a spontaneous rhythm is sensed (fig2). Therefore, the sudden changes in cycle length that usually occur after extrasystoles (the short–long sequence) are prevented and postextrasystolic T-U changes are absent or minimal (fig2).

{kind=link}
{kind=link}
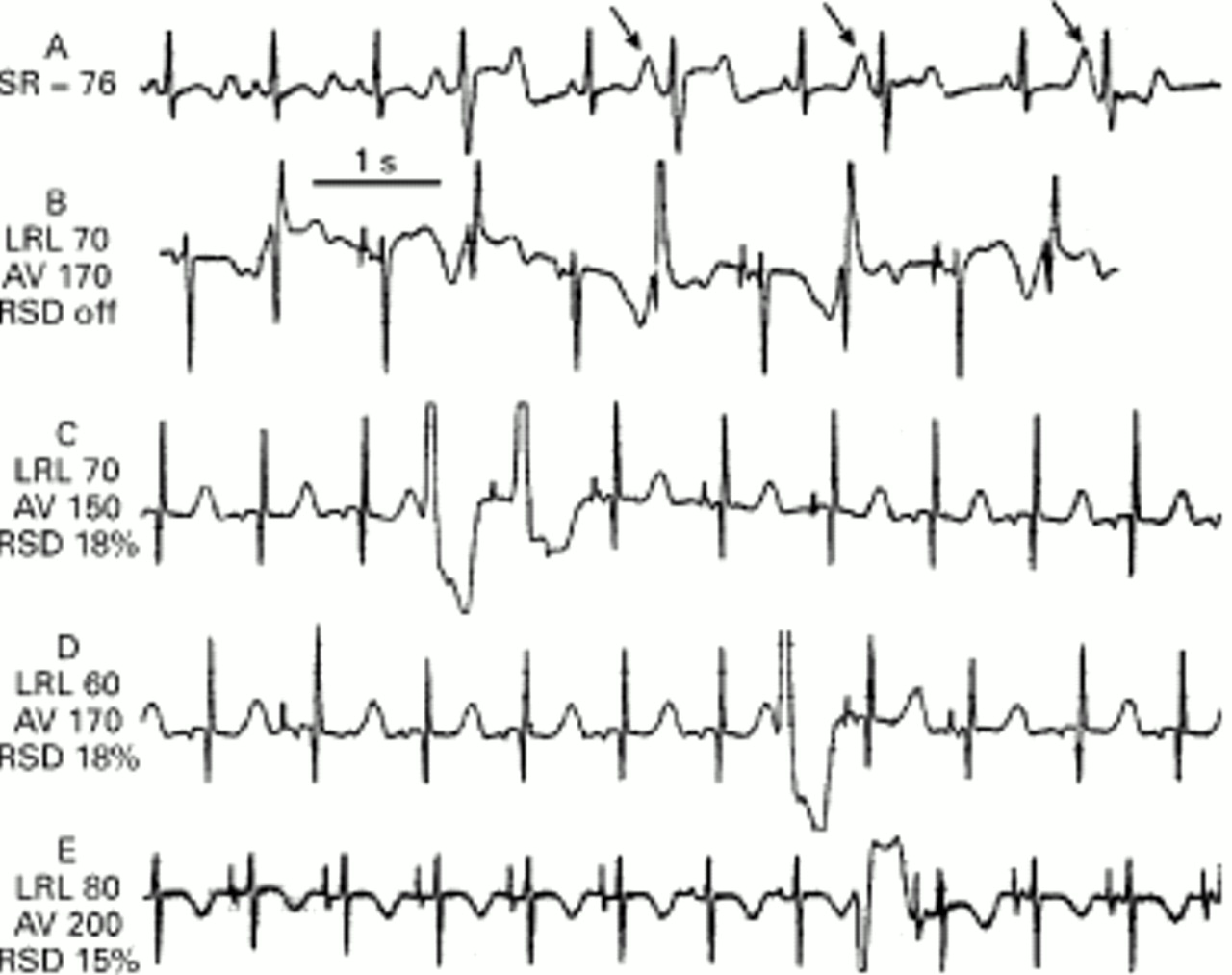
Electrocardiograms following implantation of a permanent DDDR pacemaker with rate smoothing algorithm. SR, sinus rate; LRL, AV, and RSD, programmed lower rate limit (beats/min), AV delay (in milliseconds), and rate smoothing down values (expressed as percentage of the previous R-R interval), respectively. (A) Sinus rate 76 beats/min; a premature complex is followed by a postextrasystolic pause. The ensuing sinus complex has marked post-pause U wave changes (arrow). Ventricular bigeminy (long–short sequence) supervenes. (B) DDD pacing (atrial capture with atrioventricular conduction). Rate smoothing is off. Spontaneous extrasystoles are sensed appropriately, resetting the pacemaker and causing short–long sequences that are perpetuated as ventricular bigeminy. Note the marked postextrasystolic T-U changes after each long interval. (C) Rate smoothing down of 18% during pacing with a relatively slow lower rate limit. After three sinus complexes there is a spontaneous extrasystole. Due to rate smoothing, DDD pacing occurs at a rate faster than the programmed lower rate limit: the first paced cycle is 18% longer than the coupling interval of the extrasystole. There is no atrial capture and there is retrograde conduction from the paced ventricular complex. The next three complexes show atrial pacing and capture with normal atrioventricular conduction. Each paced cycle is 18% longer than the previous one until sinus rhythm ensues. Note the absence of pauses and the absence of T-U changes. (D) Another example of rate smoothing down during DDD pacing with a slow lower rate limit (60 beats/min). An extrasystole triggers atrial pacing (with atrioventricular conduction) and the rate decreases by 18% each cycle. (E) Pacing at 80 beats/min and rate smoothing down of 15%. An extrasystole is followed by more rapid pacing. The first paced complex shows atrial capture and ventricular pseudofusion.
To test the ability of rate smoothing for preventing pause induced arrhythmias, the patient was monitored using a lower rate limit, below her spontaneous sinus rate. Spontaneous extrasystoles occurred but long–short sequences were prevented by rate smoothing. Before hospital discharge the lower rate limit and rate smoothing down values were programmed to 85 beats/min and 15%, respectively. The patient has been asymptomatic and free from arrhythmias on repeated Holter monitoring and exercise stress testing during an eight month follow up period.
Discussion
In pause dependent torsade de pointes, an escalating sequence of events occurs7 ,8: (1) a premature beat generates a postextrasystolic pause; (2) the sinus beat that follows the pause shows marked postextrasystolic T-U changes from which a subsequent ventricular extrasystole originates; (3) this extrasystole generates a new pause, which in turn is followed by more bizarre T-U changes from which progressively longer and faster runs of torsade de pointes originate. Experimental data suggest that the postextrasystolic T-U changes are the electrocardiographic representation of early afterdepolarisations and that the post-pause ventricular extrasystoles, including those initiating torsade de pointes, originate when the early afterdepolarisations are sufficiently large to depolarise the cell membrane.7 ,9 Although pause dependent torsade de pointes has been considered the hallmark of the acquired LQTS,8 recent data suggest that this long–short sequence also plays an important role in the genesis of torsade de pointes in the congenital LQTS.4 ,10 ,11 Accordingly, we believe that the main role of cardiac pacing in the congenital LQTS is the prevention of sudden pauses that facilitate the onset of torsade de pointes.4 In particular, prevention of postextrasystolic pauses is important to interrupt the escalating short–long sequence that culminates in torsade de pointes.
One way of achieving this goal is to increase the programmed lower rate limit. Based on the cycle length of the pauses leading to torsade de pointes observed in consecutive patients with congenital LQTS, we recommended a minimal pacing rate of 80 beats/min.4However, the optimal pacing rate remains to be defined. More rapid pacing will shorten postextrasystolic pauses, potentially reducing the risk of pause induced torsade de pointes. However, the potential detrimental effects on left ventricular function of years of pacing at fast rates are not completely understood.12 Certainly, pacing rates that prevent drug induced pause dependent torsade de pointes (100–140 beat/min)13 are too fast to be of practical use for long term management. Indeed, one case of dilated cardiomyopathy ascribed to 12 years of cardiac pacing at rates of 110 beats/min in a young child with congenital LQTS has recently been reported.14
An alternative method for preventing torsade involves use of pause prevention pacing algorithms, like rate smoothing. When rate smoothing down is programmed on, an R-R interval cannot increase by more than a programmable percentage from the previous cycle. Thus, whenever a spontaneous extrasystole occurs, pacing at a relatively fast rate for a few beats will occur and the pacing rate will gradually decrease until the lower rate limit is reached or a spontaneous rhythm is sensed (fig2). Two characteristics make rate smoothing particularly suitable for patients with congenital LQTS. Extrasystoles in the LQTS generally have relatively large coupling intervals4; thus, pacing triggered by rate smoothing will not be too rapid. The intact atrioventricular conduction of these patients allows programming a relatively slow upper rate limit. This will limit the pacing rate triggered by rate smoothing—following the eventual occurrence of non-sustained ventricular tachycardia—to tolerable rates.
Our limited experience precludes making general recommendations. Documentation of repeated events of pause induced torsade de pointes may identify patients likely to benefit from pause prevention pacing algorithms and may help select the appropriate pacing settings. In addition, we believe that β blocker treatment is mandatory in conjunction with pacing. Finally, the availability of the rate smoothing algorithm in some implantable cardioverter defibrillators may promote the evaluation of this treatment for the long term prevention of torsade de pointes.
Acknowledgments
The authors thank Albert Maarse (Guidant/CPI-Research, Brussels, Belgium) and Oren Karassik for their technical advice. Dr Viskin was a recipient of a training grant from the Israel Pacing Foundation