Article Text

Abstract
Objective To study underlying vascular responses in chronic heart failure in patients without ACE inhibitor treatment, and to compare them with age matched controls.
Design Forearm blood flow was studied using venous occlusion plethysmography in patients with chronic heart failure (n = 12) and matched controls (n = 13), after infusion of L-NMMA (a nitric oxide synthase inhibitor), glyceryl trinitrate (an endothelium independent vasodilator), and serotonin (an endothelium dependent vasodilator).
Results L-NMMA produced significant vasoconstriction in normal subjects (forearm blood flow reduced by 24%), but not in patients (6%; difference between groups p < 0.03). The vasodilator responses to glyceryl trinitrate were impaired in patients (p < 0.02). In normal controls, serotonin produced initial dilatation, followed by vasoconstriction at high doses. In patients, no vasodilator responses were observed, only late vasoconstriction (p < 0.03).
Conclusions The vascular responses of patients are confirmed as being abnormal. The lack of response to L-NMMA suggests that nitric oxide does not contribute to basal vascular tone in patients with chronic heart failure. The responses to glyceryl trinitrate and to serotonin suggest that there is both smooth muscle and endothelial dysfunction in patients with chronic heart failure.
- heart failure
- endothelium
- nitrates
- serotonin
Statistics from Altmetric.com
Vascular homeostasis is maintained by a complex interaction of sympathetic and parasympathetic influences acting on the vascular smooth muscle, and locally by release of endothelium derived relaxing factor (EDRF), now known to be nitric oxide (NO).1 ,2 There is evidence of endothelial dysfunction in hypertension,3hypercholesterolaemia,4 and atherosclerosis.5In chronic heart failure, neuroendocrine changes occur in an attempt to maintain central arterial pressure6 by increasing total peripheral resistance and hence reducing limb blood flow.7 ,8 In dogs with pacing induced heart failure it has been shown9 that there is decreased responsiveness to vasodilators as well as to β agonists in the peripheral circulation, which contributes to the circulatory abnormalities. In addition, the effect on the failing heart is increased when large conduit vessels are unable to dilate normally in response to increased circulatory demands, with a further fall in cardiac output.
The endothelial dysfunction in chronic heart failure responsible for these abnormal responses may be caused by several different factors, and has been shown in both the coronary and peripheral circulation. We initially wished to establish whether basal NO production is altered in patients with chronic heart failure, as previous studies had given conflicting results.10-12 This was achieved by assessing the effect of infusing N-monomethyl-L-arginine (L-NMMA), a competitive inhibitor of NO synthase in the vascular wall, on forearm blood flow.
Previously the most commonly reported abnormality of endothelial function in chronic heart failure has been impaired dilatation in response to infusion of acetylcholine,10 ,13 ,14 which is dependent on both an intact endothelium and normal smooth muscle function. It is difficult to assess the contribution of the endothelium if smooth muscle function is impaired. Some studies have suggested that this is the case in chronic heart failure,8 ,14 but this has not always been confirmed.10 One of the aims of the present study therefore was to observe the effects of glyceryl trinitrate, an endothelium independent vasodilator acting directly on smooth muscle, on the vascular bed of the human forearm. Finally, we studied for the first time the effects of serotonin (5-hydroxy-tryptamine, 5HT) on endothelial function in chronic heart failure. Serotonin at low doses produces NO mediated vasodilatation,15 ,16 but at high doses it causes smooth muscle constriction.
It is difficult to evaluate the underlying circulatory abnormalities in chronic heart failure when patients are receiving potent vasodilator drugs such as angiotensin converting enzyme (ACE) inhibitors. Even diuretics have vascular effects.17 However, since the publication of CONSENSUS I18 and subsequent trials showing the therapeutic benefit of ACE inhibitors, it is increasingly difficult to find patients who are not taking such drugs. Furthermore, it is possible that modification of the vascular responses by ACE inhibition could persist longer than direct vasodilator effects. We therefore studied patients with chronic heart failure who had never taken an ACE inhibitor or angiotensin II receptor antagonist.
Methods
SUBJECTS
Twelve patients with compensated chronic heart failure were studied. The mean duration of symptoms was 18.2 months (range 4 to 96) but all patients had been clinically stable for at least three months before study. Five were in New York Heart Association (NYHA) symptom grade II, six in grade III, and one in grade IV. All had a history of hospital admission for pulmonary oedema on at least one occasion and had a mean left ventricular ejection fraction (LVEF) of 26.6% (range 8% to 40%), as measured by echocardiography or radionuclide angiography. Cardiothoracic ratio on a chest radiograph was greater than 0.5 in all cases. The aetiology of chronic heart failure was ischaemic heart disease in eight, valvar heart disease in one (mitral regurgitation), and idiopathic dilated cardiomyopathy in three. Five patients were in sinus rhythm at the time of study and seven in atrial fibrillation with a relatively constant ventricular response. All were on treatment with loop diuretics (mean dose of frusemide or equivalent 60 mg daily, range 40 to 160 mg). In addition eight were taking digoxin, six aspirin, six nitrates, and one diltiazem. Both aspirin and long acting nitrates were omitted for 48 hours before study and digoxin for 24 hours. No patients were taking ACE inhibitors or angiotensin II receptor antagonists. All drugs were withheld on the morning of study. Subjects were excluded if there was a history of diabetes (fasting glucose > 7.8 mmol/l), hypercholesterolaemia (cholesterol > 6.2 mmol/l), or hypertension (blood pressure > 160/90 mm Hg).
Thirteen healthy volunteers acted as controls and were considered to be normal on the basis of history, examination, ECG, routine laboratory analysis, and cardiopulmonary exercise testing. All subjects gave written informed consent for all procedures. The study was approved by the local ethics committee of the Queens University of Belfast. Table 1summarises the clinical characteristics of patients and controls.
Characteristics of patients and controls; peakV˙o 2 available in 11 patients only
PROCEDURES
Studies were carried out in the morning in a temperature controlled laboratory (24–26°C). Following an overnight fast, during which alcohol and caffeine containing beverages were prohibited, subjects were asked to rest supine with the experimental arm on a support slightly above the level of the heart.
Subjects underwent cannulation of the non-dominant brachial artery using a 27 gauge steel needle (Cooper’s Needle Works, Birmingham, UK) connected to an 18 gauge epidural line under local anaesthesia (1% lignocaine, Antigen Pharmaceuticals, Roscrea, Republic of Ireland). After a period of 30 minutes during which physiological saline was infused at a rate of 0.5 ml/min to allow blood flow to stabilise, resting forearm blood flow was measured using venous occlusion plethysmography. An indium–gallium strain gauge was placed around the widest part of the forearm (approximately two thirds of the distance from the wrist to the elbow). An occlusion cuff was placed at the wrist and a congestion cuff above the elbow. The wrist cuff was inflated to above systolic pressure (200 mm Hg) for 30 seconds before the measurements. The congestion cuff was inflated rapidly to a pressure between venous and arterial (40 mm Hg) during each measurement (between five and 10 seconds). The average of five consecutive measurements was used and the tracings were analysed by an independent observer without knowledge of the clinical status of the subject. Forearm blood flow was expressed as ml/min/100 ml forearm volume.
Drugs were infused into the study arm using a constant rate infuser (Braun Perfusor pump, Melsungen, Germany). Forearm blood flow was measured at baseline and then immediately after drug infusion. Drugs were given in random order and were prepared on the morning of study, using sterile physiological saline. Between different doses and drugs the drug infusion set was flushed with saline, and sufficient time was allowed for the forearm blood flow to return to baseline (glyceryl trinitrate 20 minutes, serotonin and L-NMMA 30 minutes).
Glyceryl trinitrate (Nitrocine, Schwarz Pharma, UK) was infused at concentrations of 3, 6, 9, and 12 nmol/min at each dose for two minutes in all patients. Serotonin (creatinine sulphate complex, Sigma, Poole, UK) was dissolved and infused at doses of 0.017, 0.17, 1.70, 17.0, and 170 μmol/min each for two minutes. L-NMMA (Clinalfa AG, Basel, Switzerland) was infused at 8 μmol/min for five minutes.
STATISTICS
Patient and control characteristics were compared using independent Student’s t tests. Statistical analysis of forearm blood flow was performed using repeated measures analysis of variance (anova) for between group effects and Dunnett’s test for multiple comparisons for within group effects. A probability (p) value of < 0.05 was considered significant and a value of < 0.01 as highly significant. The results of forearm blood flow are expressed as change in forearm blood flow from baseline (mean (SEM)).
Results
There were no significant differences between baseline characteristics of patients and controls with the exception of systolic and diastolic blood pressure and peak achieved oxygen consumption (V˙o 2, ml/min/kg) on treadmill testing which showed a highly significant difference (table 1).
In response to infusion of L-NMMA, vasoconstriction (a 24% reduction in forearm blood flow) was seen in the control group (p = 0.01) but no significant changes were seen in the patients (6% reduction), the difference between the groups being significant (p = 0.03) (table2).
Forearm blood flow (FBF) before and after L-NMMA infusion
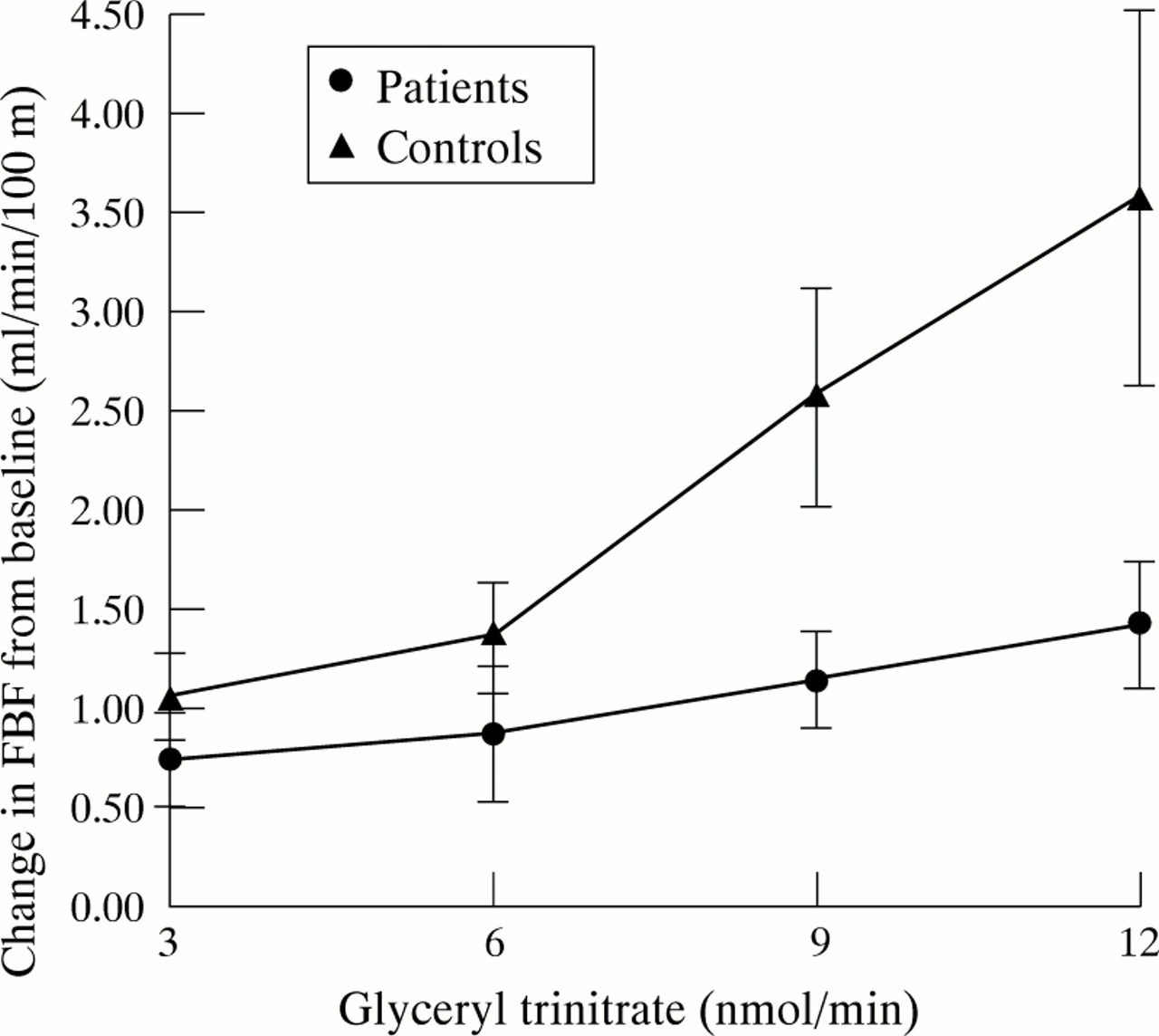
In response to infused glyceryl trinitrate, vasodilatation was noted in both patients and controls (p < 0.05), with a significant difference between the two groups (p = 0.02). The responses in the patients were attenuated compared with controls (fig 1).

Change in forearm blood flow (FBF) in response to intra-arterial infusion of glyceryl trinitrate. Values are means, error bars = SEM. *p < 0.05, patients v controls in response to 9 and 12 nmol/min glyceryl trinitrate.
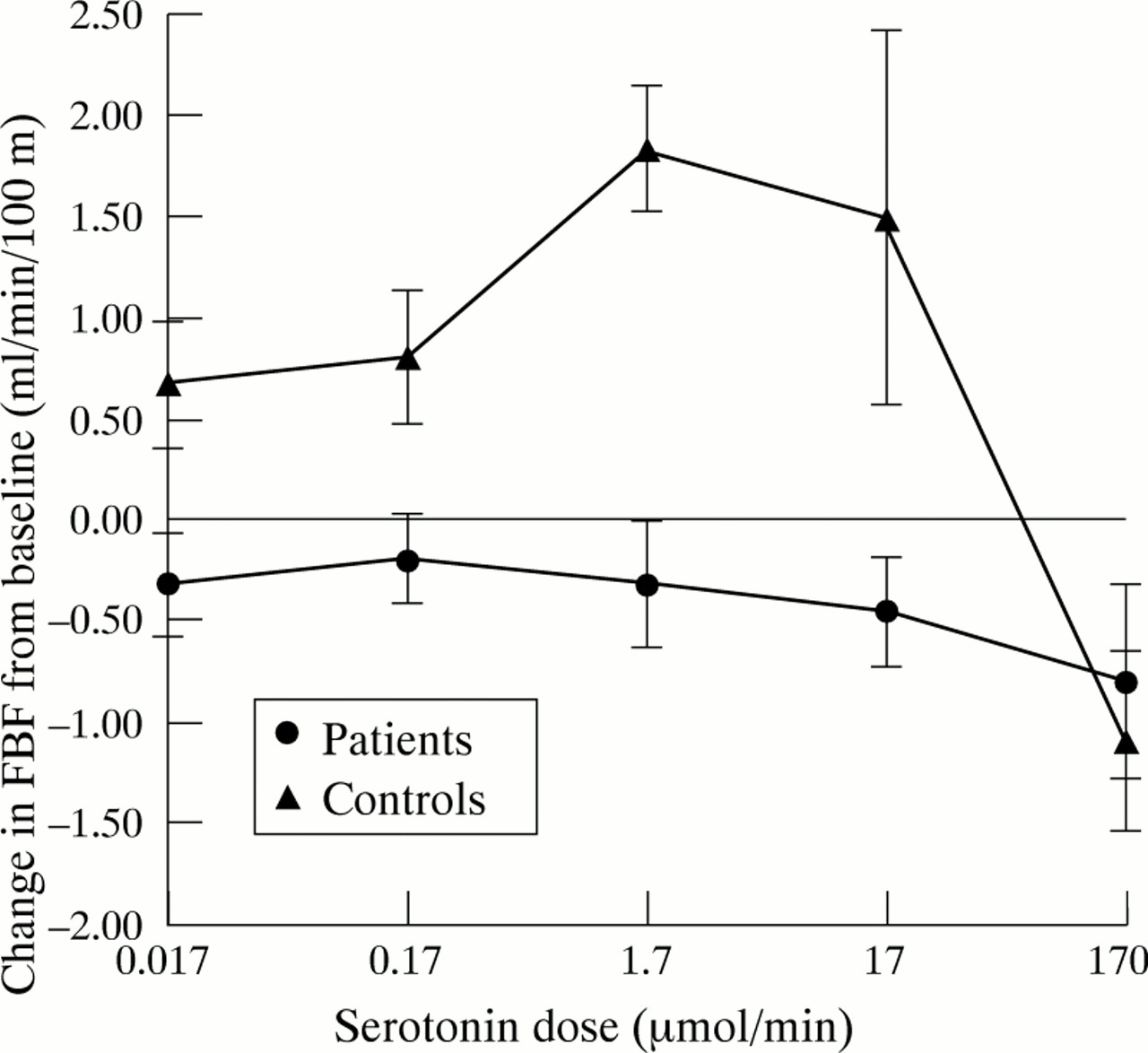
A biphasic response to infused serotonin was observed in controls, with vasodilatation at low doses and vasoconstriction at high doses. In patients, no vasodilatation was noted, although significant (p = 0.04) vasoconstriction occurred at high doses. A difference in the response to serotonin infusion (p = 0.03) was observed between the two groups (fig 2).
{kind=link}
{kind=link}
Change in forearm blood flow (FBF) in response to intra-arterial infusion of serotonin. Values are means, error bars = SEM. *p < 0.05, patients v controls at 0.017–1.7 μmol/min serotonin.
Discussion
We have shown several abnormalities in the peripheral vascular responses in patients with chronic heart failure. First, there were differences between control and patient groups in response to L-NMMA. This is an analogue of L-arginine, the substrate required for production of NO, and as such acts as a competitive inhibitor of NO synthase, the enzyme converting L-arginine to NO. As shown here and in previous work,19 ,20 L-NMMA causes a reduction in basal NO production resulting in vasoconstriction in normal controls. Results of previous studies in patients with chronic heart failure have been variable, with both an enhanced10 and a decreased11 vasoconstrictor effect, or a similar response to normal controls.12 It has been suggested that an enhanced vasoconstrictor response may result from a paradoxical increase in production of NO in chronic heart failure.21It has also been shown that plasma nitrate, an end product of NO metabolism, can be increased in chronic heart failure,22although this cannot be directly attributed to increased NO production as there may be other reasons for the increased levels, such as sepsis and high dietary nitrate intake.
Our results confirm previous observations12 that L-NMMA does not change basal blood flow in patients with chronic heart failure, suggesting that NO does not contribute to vascular tone in these subjects, in contrast to the findings in normal subjects. In chronic heart failure it has been established that there is an increase in circulating vasoconstrictors23 ,24 and a reduction in vasodilators such as prostacyclin (PGI2),25resulting in an increase in the overall resting vasomotor tone. It has also been suggested that endothelial damage could result in a reduction in availability of endothelium derived NO from either decreased production or increased breakdown of NO. Decreased production may in part be a result of downregulation of the mRNA for the two enzymes required for the production of endothelium derived vasodilators.26 This downregulation appears to be a specific defect secondary to chronic heart failure, rather than a complex neurohormonal interaction. The rapid inactivation of NO may be caused by increased free radical production, as previous work has shown inhibition of endothelium dependent vasodilatation by oxygen derived free radicals.27 It is also thought that cell surface receptor abnormalities or changes at the G protein level may account for loss of effect of free NO, as has been shown in atherosclerosis and hypercholesterolaemia.28 In addition, previous work in our department investigating the inflammatory response in chronic heart failure by measurement of cytokine activity has suggested that although there is evidence of a generalised activation of inflammatory mediators, this may not be as marked as was previously thought.29 In view of the presence of this preconstricted vasculature and low levels of circulating NO, there is less possibility of further constriction.
Our patients differed from those studied previously in that they were identified before being given ACE inhibitor treatment. There is evidence that treatment with ACE inhibitors can improve peripheral vascular function in chronic heart failure through an improvement in endothelial function.30-32 Recent results from the TREND (trial on reversing endothelial dysfunction) study33 in patients with coronary artery disease (but not chronic heart failure) showed that treatment with quinapril can improve endothelial function. The mechanism of the change in endothelial function was thought to be an increase in circulating bradykinin and a decrease in angiotensin II. Both of these have been shown to occur in patients with chronic heart failure treated with ACE inhibitors. Therefore it may be that the patients in previous studies had some improvement of their endothelial function as a result of their treatment, which could affect their responses to L-NMMA.
We have also shown abnormal smooth muscle function in our study in the responses to glyceryl trinitrate, which is an endothelium independent vasodilator acting directly on the vascular smooth muscle. The previous evidence for smooth muscle dysfunction is conflicting. Dilatation in response to endothelium independent vasodilators of the external iliac artery,8 the radial artery,10 and the femoral artery14 in chronic heart failure has been shown to be reduced. The first study used papaverine and the other two used glyceryl trinitrate. In the second study the same patients showed preserved responses of the forearm resistance vessels. This suggested that perhaps the origin of the endothelium and the size of the vessel affected its response to exogenous vasodilators. In contrast, other work in patients with chronic heart failure has shown that there is significantly reduced vasodilatation in forearm resistance vessels in response to local infusion of glyceryl trinitrate,13 which is in keeping with our findings. A recent study of patients with chronic heart failure secondary to valvar and congenital heart disease also revealed impaired endothelium independent as well as endothelium dependent vasodilatation.34 The abnormalities in smooth muscle function may result from alterations in smooth muscle responsiveness or impaired diffusion of NO through the arterial wall. There is also some evidence that over a period of time changes occur in the vessel wall that could result in decreased arterial compliance.35 ,36 The impaired smooth muscle responsiveness is thought to be partly the result of alterations in intracellular cyclic guanosine monophosphate function.37The importance of demonstrating impaired smooth muscle responsiveness in chronic heart failure cannot be underestimated, as many current treatments available depend on functioning smooth muscle, and these findings may also in part explain the nitrate resistance seen in some patients with chronic heart failure. These findings also have implications for abnormal endothelium dependent responses in chronic heart failure, such as to acetylcholine, which would now appear to be caused in part by reduction in the smooth muscle effector mechanism.
Finally, we have shown for the first time that there are abnormal vascular responses to infused serotonin in chronic heart failure. It has been found that serotonin is closely involved in the early stages of atherogenesis when it is released from aggregating platelets, and there is evidence that it may cause endothelial cell damage at this stage, in conjunction with thromboxane A2.38 Infusion of serotonin causes vasodilatation at low doses and vasoconstriction at high doses when infused into the forearm of normal volunteers.39 ,40 The vasodilator response appears to be mediated by NO through stimulation of 5HT-like receptors,15 ,16 and has been shown in coronary arteries41-43 both in vitro and in vivo. The doses used in our study produce a serum concentration of serotonin approximating that produced by platelet aggregation in vivo.41 These studies also show that in the absence of the endothelium, or in the presence of damaged endothelium as in coronary artery disease, serotonin has a vasoconstrictor response as a result of a direct effect on the vascular smooth muscle. This vasoconstrictor response appears to be enhanced by threshold levels of endothelin-1,44 which may contribute to the systemic vasoconstriction seen in chronic heart failure. In our study we showed the predicted biphasic response in control subjects, but in the patients no vasodilatation was observed, and enhanced vasoconstriction was noted. This provides further evidence for abnormal endothelial function and enhanced responsiveness to certain vasoconstrictors in chronic heart failure. In this case the vasoconstrictor response does not appear to be mediated through the endothelium, and so does not contradict our previous findings with L-NMMA.
The observed responses to serotonin are important, as serotonin is an endogenous substance closely involved in the changes in vessels occurring in the early stages of chronic heart failure caused by ischaemic heart disease. Our study provides further information on the function of the endothelium and the vascular smooth muscle in chronic heart failure, as both sites can be investigated together; it therefore increases our knowledge of the early vascular adaptations involved in chronic heart failure.
Acknowledgments
We thank Sister E Crawford and Mrs A Fairweather for their help with patient care, and the Pharmacy Department of the Belfast City Hospital and Mrs Sophia Copeland for drug preparation. SMM was in receipt of a Royal Victoria Hospital Research Fellowship.