Article Text

Abstract
Aim To determine whether measurement of serum troponin T concentration after first acute myocardial infarction can be used to identify patients with a left ventricular ejection fraction of < 40%, who have an adverse prognosis.
Methods Troponin T concentration was measured, and coronary and left ventriculography performed in 50 consecutive patients with acute myocardial infarction. Angiographic left ventricular ejection fraction was compared with serum troponin T concentration. Patients with previous myocardial infarction were excluded.
Results There was a strong negative correlation between left ventricular ejection fraction and troponin T concentration. Spearman’s rank correlation coefficient (corrected for ties) was −0.72 (95% confidence intervals (CI) −0.55 to −0.83; p < 0.0001). Analysis by receiver operator characteristic curve produced an area under the curve of 0.9773 (95% CI 0.9409 to 1.0136). A troponin T concentration of > 2.8 μg/l predicted a left ventricular ejection fraction of < 40% with a sensitivity of 100% (CI 84.6 to 100.0) and specificity of 92.9% (CI 76.5 to 99.1). Exclusion of patients who did not receive thrombolytic treatment did not significantly affect the results.
Conclusion Serum troponin T concentration measured 12–48 hours after admission for first myocardial infarction is a reliable, simple, quick, inexpensive, non-invasive method for identifying patients with a left ventricular ejection fraction of < 40% for whom there is a poor prognosis.
- troponin T
- acute myocardial infarction
- angiotensin converting enzyme inhibitors
- left ventricular function
Statistics from Altmetric.com
- troponin T
- acute myocardial infarction
- angiotensin converting enzyme inhibitors
- left ventricular function
Left ventricular function is the best individual predictor of mortality after acute myocardial infarction.1 Late mortality and morbidity after myocardial infarction are improved by treatment with angiotensin converting enzyme (ACE) inhibitors in patients whose infarction is complicated by heart failure2 and in patients whose ejection fraction is < 40%.3 Long term treatment (1–4 years) with ACE inhibitors has decreased mortality in clinical trials in which postinfarction patients were selected on the basis of clinical heart failure (27% decrease in the acute infarct ramipril efficacy study)2 or impaired left ventricular function (19% decrease in the survival and ventricular enlargement trial).3 These studies also showed a decrease in progression to heart failure and in hospitalisation for severe heart failure or further ischaemic events. In contrast, trials in which ACE inhibitors were given to all patients after myocardial infarction were much shorter (between 30 days and 6 months), produced conflicting results on mortality risk reduction (9% increase in the cooperative new Scandinavian enalapril survival study II,4 7% decrease in the fourth international study of infarct survival,5 12% decrease in GISSI-3,6 and no change in the Chinese captopril study7), and showed no evidence of benefit to patients who did not have heart failure.
Measurement of left ventricular ejection fraction is therefore important for prognosis and for identification of patients who would benefit from long term ACE inhibitors because their left ventricular ejection fraction is < 40% but who do not have heart failure. Estimation of left ventricular ejection fraction requires echocardiography or contrast or radionuclide left ventriculography. Echocardiography is probably the most widely available of the three methods but echocardiograms good enough for ejection fraction measurement are not possible in all patients. Contrast and radionuclide left ventriculography are more expensive and are not widely available in district hospitals.
Biochemical markers of myocardial damage have long been used to estimate infarct size and closely correlate with five year mortality.8 Infarct size can be estimated from creatine kinase MB9 and myoglobin,10 ,11 but repeated estimations are required during a small time window. Moreover, it is infarct size rather than residual left ventricular function that is measured, although they are related. Furthermore, thrombolytic treatment profoundly alters the kinetics of conventional cardiac markers.12 ,13 The increased release of creatine kinase after reperfusion is such that peak creatine kinase activity after thrombolysis can no longer be used as even an approximate indicator of myocardial infarct size. While infarct size will affect left ventricular function, the direct relation between creatine kinase or myoglobin and left ventricular ejection fraction has not been assessed.
Recently, serum troponin T has emerged as a specific indicator of myocardial damage in acute myocardial infarction.14-16Cardiac troponin T release closely relates to infarct size,17 but its relation to left ventricular ejection fraction has not been determined. Unlike creatine kinase and myoglobin,12 ,13 its concentration is unaffected by thrombolysis after the first 12 hours, following which it shows a stable plateau for about 48 hours.14 ,18 Serum troponin T concentration may therefore inversely correlate with left ventricular ejection fraction as a consequence of the inverse relation between infarct size and left ventricular ejection fraction. This study investigated the value of a single troponin T concentration, estimated 12–48 hours after admission, to provide an integrated measurement of the degree of cardiac damage following first acute myocardial infarction, as a method of identifying patients with a left ventricular ejection fraction of < 40%.
Patients and methods
Patients admitted with first acute myocardial infarction between February and December 1994 were identified retrospectively. Myocardial infarction was diagnosed if at least two of the following were present: cardiac chest pain; ST segment elevation of at least 2 mm in chest leads or 1 mm in limb leads, or new Q waves in at least two contiguous leads; and raised creatine kinase activity to at least twice the upper limit of the reference range. Patients with significant renal impairment (creatinine more than 220 μmol/l) and a history of heart failure and myocardial infarction were excluded. Troponin T concentration was estimated in 50 patients (44 men) 12–48 hours after admission who had undergone coronary and left ventricular angiography for either postinfarction angina or assessment of prognosis. The mean age of patients was 62 (range 38–85) years. Four patients (8%) had non-insulin dependent diabetes mellitus, and eight (16%) had mild hypertension. Eighteen patients (36%) did not receive thrombolytic treatment. Coronary angiography was performed a mean of 4.8 weeks after infarction (range 2 days to 32 weeks). Left ventricular ejection fraction was estimated from standard left ventriculograms, in the right anterior oblique view using Snow’s method,14 by an investigator blinded to troponin T concentration. Troponin T was estimated by enzyme linked immunosorbent assay as previously described.19
The relation between left ventricular ejection fraction and troponin T concentration was studied using Spearman’s correlation coefficient and by systematic analysis of sensitivity and specificity. A receiver operator characteristic (ROC) curve was constructed to examine the relation between cardiac troponin T concentration and ejection fraction. In this technique, the patients were initially categorised into two datasets, those with an ejection fraction of < 40% and those with an ejection fraction of ⩾ 40%. This produced an initial binary classification. This ejection fraction value was based on previous clinical trials as having prognostic significance. The ability of cardiac troponin T to assign patients accurately into the two groups was determined by calculating the sensitivity and specificity of troponin T (the numeric variable) at progressively increasing cut off concentrations of troponin T. Sensitivity was plotted against 1−specificity to give the ROC plot. The nearer the curve to the top left corner of the graph, the better the test. The point of inflection of the ROC curve allows selection of the best trade off between sensitivity and specificity. The data were initially analysed for the 50 patients who had suffered their first myocardial infarct. The effect of thrombolysis was assessed by repeating the analysis after excluding patients who did not receive thrombolytic treatment (n = 18).
Results
In the 50 patients suffering their first myocardial infarct, there was a strong negative correlation between left ventricular ejection fraction and troponin T concentration (fig 1). Spearman’s rank correlation coefficient (corrected for ties) was −0.72 (95% confidence interval (CI) −0.55 to −0.83; p < 0.0001).

Relation between troponin T concentration and left ventricular fraction.
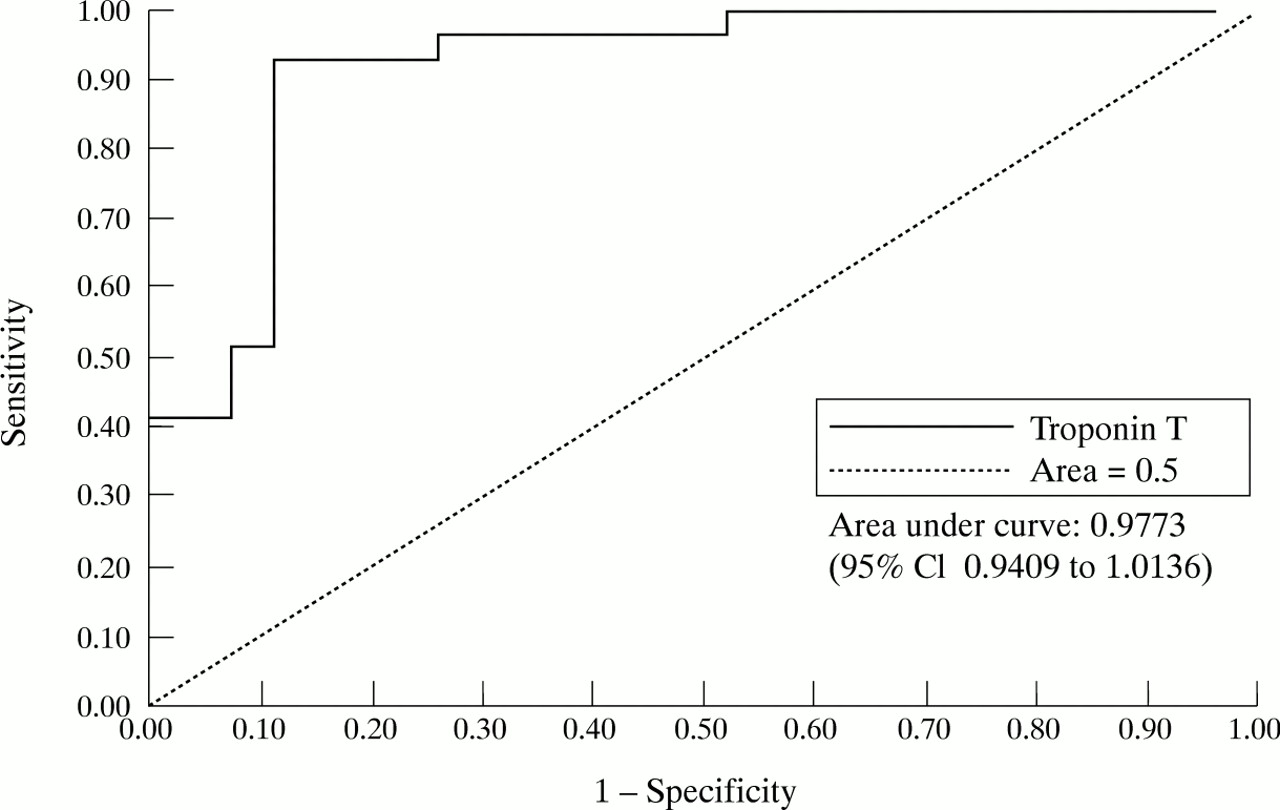
Analysis by ROC curve produced an area under the curve of 0.9773 (95% CI 0.9409 to 1.0136) at a cut off left ventricular ejection fraction of 40% (fig 2). A troponin concentration of > 2.8 μg/l predicted a left ventricular ejection fraction of < 40% with a sensitivity of 100% (CI 84.6 to 100.0) and specificity of 92.9% (CI 76.5 to 99.1).
{kind=link}
{kind=link}
Receiver operator characteristic curve showing sensitivity and specificity of troponin T.
The result of re-analysis to examine the effect of reperfusion by excluding 18 patients who did not receive thrombolysis was no different from analysis of all patients.
Discussion
Serum troponin T is accepted as a highly reliable biochemical marker14-16 for detecting myocardial damage, and its use in the diagnosis of acute myocardial infarction is increasing. Data show that serum troponin T is related to the amount of myocardial damage,17 but the relation between serum troponin T and impairment of left ventricular function after acute myocardial infarction has not been examined. This study shows a strong negative correlation between serum troponin T concentration measured 12–48 hours postmyocardial infarction and angiographic left ventricular ejection fraction (p < 0.0001). Analysis of the relation between troponin T and angiographic left ventricular ejection fraction by ROC curve shows that a troponin T concentration of > 2.8 μg/l is a sensitive (100%) and specific (92.9%) indicator of a left ventricular ejection fraction of < 40% after a first myocardial infarction. Re-analysis without 18 patients who did not receive thrombolytic treatment showed no difference from analysis of data from all patients, which is consistent with this finding.
Troponin T has practical advantages over other markers in the assessment of left ventricular ejection fraction. After acute infarction, troponin T has a peak value at 12 hours from the onset of pain, if successful reperfusion has occurred,14 ,18corresponding to washout of the cytoplasmic fraction. The plateau phase of troponin T, however, lasts up to 48 hours and represents an integrated estimate of myocyte necrosis. The peak value will therefore be missed in samples taken 12–48 hours after admission but there is a large time window. This makes repeated sampling unnecessary and represents a cost and time effective method of diagnosis and quantification. This is in contrast to creatine kinase MB or myoglobin for which multiple measurements are required to identify the peak value, or to integrate the area under the curve.
Only 50 of 261 patients admitted with acute myocardial infarction during the study period were eligible for entry. Furthermore, left ventricular ejection fraction was estimated 4.8 weeks after infarction. A larger prospective study in which other factors such as left ventricular hypertrophy are examined is therefore required.
CONCLUSION
Serum troponin T concentration has a strong negative correlation with left ventricular ejection fraction after a first acute myocardial infarction. This marker offers a simple, inexpensive, quick, non-invasive method of identifying patients with a left ventricular ejection fraction of < 40%. Estimation of troponin T can also be used to identify those patients who may benefit from other treatments—for example, ACE inhibitors.