Article Text

Abstract
Objective To evaluate whether nurse run clinics in general practice improve secondary prevention in patients with coronary heart disease.
Design Randomised controlled trial.
Setting A random sample of 19 general practices in northeast Scotland.
Patients 1173 patients (685 men and 488 women) under 80 years with working diagnoses of coronary heart disease, but without terminal illness or dementia and not housebound.
Intervention Nurse run clinics promoted medical and lifestyle aspects of secondary prevention and offered regular follow up.
Main outcome measures Components of secondary prevention assessed at baseline and one year were: aspirin use; blood pressure management; lipid management; physical activity; dietary fat; and smoking status. A cumulative score was generated by counting the number of appropriate components of secondary prevention for each patient.
Results There were significant improvements in aspirin management (odds ratio 3.22, 95% confidence interval 2.15 to 4.80), blood pressure management (5.32, 3.01 to 9.41), lipid management (3.19, 2.39 to 4.26), physical activity (1.67, 1.23 to 2.26) and diet (1.47, 1.10 to 1.96). There was no effect on smoking cessation (0.78, 0.47 to 1.28). Of six possible components of secondary prevention, the baseline mean was 3.27. The adjusted mean improvement attributable to intervention was 0.55 of a component (0.44 to 0.67). Improvement was found regardless of practice baseline performance.
Conclusions Nurse run clinics proved practical to implement in general practice and effectively increased secondary prevention in coronary heart disease. Most patients gained at least one effective component of secondary prevention and, for them, future cardiovascular events and mortality could be reduced by up to a third.
- coronary heart disease
- secondary prevention
- randomised controlled trial
- nurse led clinics
Statistics from Altmetric.com
Secondary prevention in patients with coronary heart disease aims to prevent further events after coronary heart disease has manifested itself. Several measures have proved in clinical studies to be effective as secondary prevention.1 “Medical” measures include aspirin treatment,2 and blood pressure3 and lipid control4 ,5; “lifestyle” measures include increased exercise,6healthy diets,7 and smoking cessation.8
Current secondary preventive treatment and practices are, however, suboptimal. Studies in general practice9 and hospital10 settings have reported considerable potential to increase secondary prevention through medical and lifestyle interventions. Most patients with coronary heart disease are looked after in primary care, so general practitioners have been urged to make secondary prevention a priority.1 However, the task of implementing a comprehensive package of effective measures to large numbers of patients (up to 5% of patients on general practitioners’ lists have coronary heart disease) has been described, rightly, as “daunting”.1 It is, therefore, important to develop implementation strategies that are practical and effective.
In Grampian, nurse led clinics in primary care were designed to promote secondary prevention. This study aimed to evaluate whether they achieved this by testing the hypothesis that such clinics would increase effective secondary prevention among patients with established coronary heart disease in general practice. A secondary analysis compared effects between practices with high and low levels of baseline performance.
Methods
This was a randomised controlled trial, set in 19 general practices in northeast Scotland. The study was granted ethical approval by the Grampian Health Board and University of Aberdeen joint ethics committee.
STUDY POPULATION
The procedure used to select general practices and patients has been described previously9 and is summarised in fig 1. General practices were selected randomly from all practices in northeast Scotland. Patients were included if they had a working diagnosis of coronary heart disease which was documented in their general practice case notes. They were excluded if they were terminally ill, had dementia, were housebound, or at the request of their general practitioner.

Selection of general practices and patients for the study.
INTERVENTION
The intervention consisted of nurse run clinics in general practice. The clinics ran for one year, and attempts were made to invite all patients to attend for a first visit during the first three months. Follow up was encouraged, with timing determined by clinical circumstances, but usually every two to six months.
Clinic visits had four stages. First, symptoms were reviewed in an attempt to identify poor control and refer appropriately. Second, drug treatment was reviewed to encourage aspirin use (when not contraindicated) and identify possible drug side effects. Third, blood pressure and lipids were assessed with reference to British Hypertension Society guidelines11 and local lipid management guidelines.12 If drug treatment was indicated, referral was made to a general practitioner. Finally, behavioural risk factors (exercise, diet, smoking) were assessed and, if appropriate, behavioural change was negotiated. Each clinic visit concluded with feedback, goal planning, and an agreed action plan, which were outlined on a take home form. First visits took around 45 minutes (30 minutes to one hour) and follow up visits around 20 minutes (10 to 30 minutes).
To run the clinics, one or two health visitors, district nurses, or practice nurses (28 in all) were nominated from the primary care teams of participating practices. Clinics were fitted into their usual working routine, which included care for all patients on the practice list. Training in clinic protocols and techniques to facilitate behavioural change were provided during a study day before intervention and a half day during the intervention year. A clinic coordinator (JT) provided support by phone. Clinic protocols were detailed in a manual, and client record cards were provided. “One Step at a Time” leaflets (Grampian Healthcare Community Dietitians) were provided to help with dietary modifications and “Stepping Out” programmes13 to promote physical activity.
OUTCOME MEASURES
Data were collected before intervention and at one year. Clinical data—including details of blood pressure and lipid management—were collected by audit of medical records. Data about aspirin use, diet, smoking, and exercise were collected by postal questionnaire. Diet was assessed using the DINE score,14 a validated instrument for use in primary care which measures total dietary fat. Smoking and exercise were assessed using the health practices index,15validation of which showed striking relations to mortality, independent of baseline health or economic status. Criteria used to define “appropriate secondary prevention” were:
- (1)
- Aspirin taken (or contraindicated by allergy or peptic ulceration)
- (2)
- Blood pressure managed according to British Hypertension Society guidelines11
- (3)
- Lipids managed according to Grampian general practice lipid management guidelines12
- (4)
- Moderate physical activity (index of physical activity > 4)15
- (5)
- Low fat diet (DINE diet score < 30)14
- (6)
- Not currently smoking.
Blood pressure was accepted as being managed according to British Hypertension Society recommendations if the last blood pressure (recorded within three years) was less than 160/90 mm Hg or receiving attention (treated, checked within three months, or referred to a specialist clinic).11 Lipids were managed according to Grampian general practice lipid management guidelines if the last cholesterol (recorded within three years) was 5.2 mmol/l or less, or receiving attention (treated, checked within three months, or referred to a specialist clinic).12 To ensure that any differences were not simply a result of referral or increased checking, secondary analyses were conducted on general practitioner managed patients in which managements were “unacceptable” for patients whose sole qualifications were checks within three months.
To provide an estimate of overall secondary prevention, a cumulative score was generated by counting the number of appropriate treatments and behaviours for each patient.
PROSPECTIVE SAMPLE SIZE CALCULATION
An absolute improvement in the proportion of patients receiving “appropriate” secondary prevention (for each component) by 10% was considered important and it was calculated that a sample of 808 subjects would have 80% power to detect this at the 5% significance level. Allowing 10% loss to follow up due to death, serious illness, or flitting and 70% response to the outcome survey, an initial sample size of 1300 was required.
STATISTICAL ANALYSES
Standard statistical techniques were used on an intention to treat basis and analyses facilitated using SPSS for Windows version 6.1.3. Analyses of binary outcomes were conducted by logistic regression adjusting for baseline performance, age, sex, and practice. The changes in cumulative rating between baseline and outcome were analysed using the independent samples t test and adjusted using analysis of covariance.
ASSIGNMENT
Patients were randomised by the researchers after giving informed consent and before intervention. Eligible patients were stratified by age (less or more than 65 years), sex, and general practice, and randomised (by individual) using tables of random numbers. Before clinics began, the clinic nurses were supplied with lists of intervention group patients. Control group patients were identified after collection of outcome data.
Results
STUDY PROGRESS
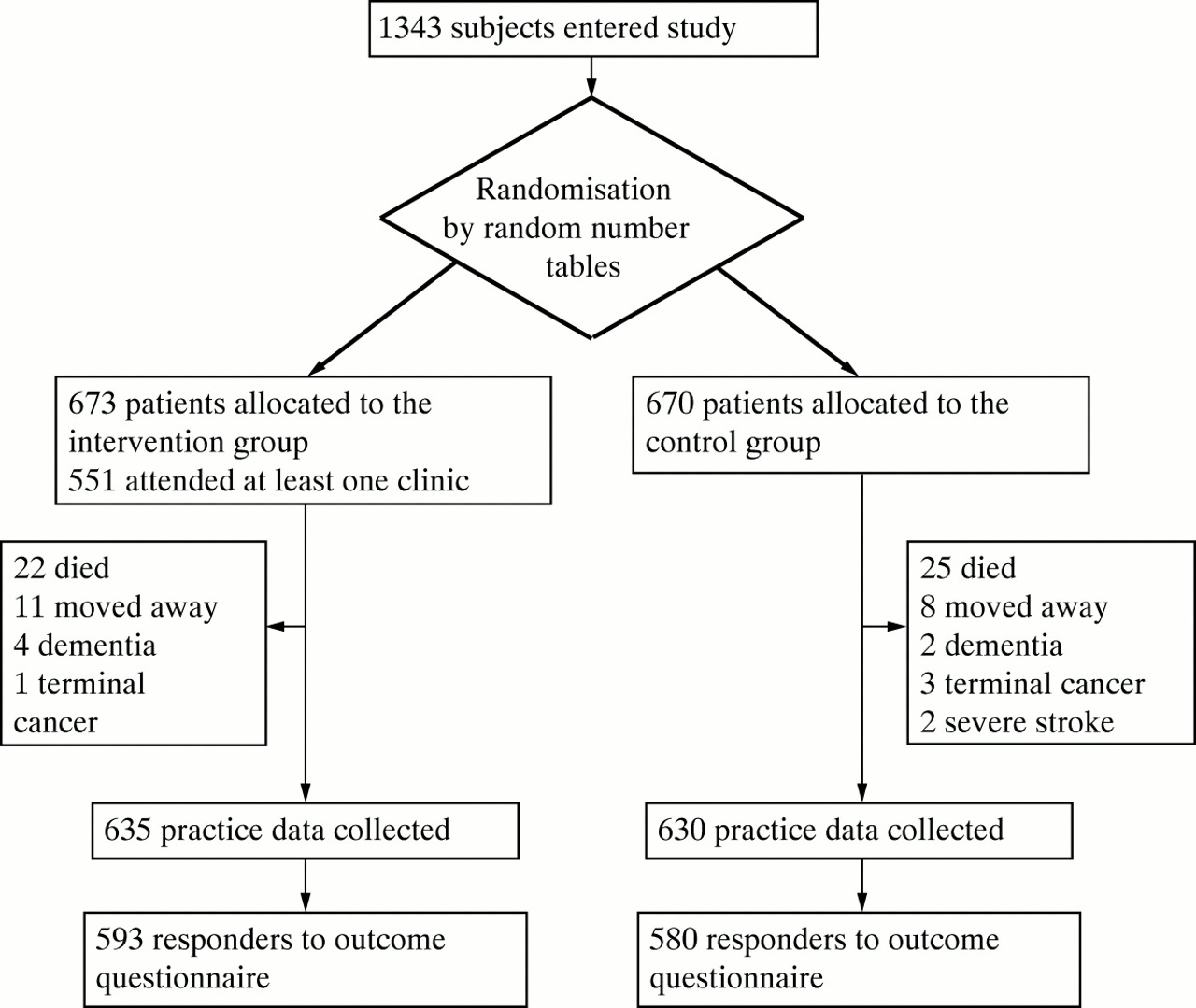
Figure 2 shows the trial profile. Of intervention group patients, 82% attended at least one clinic. In all, nurses and health visitors spent 915 hours running the clinics, which represented one hour and 22 minutes per patient per year.
{kind=link}
{kind=link}
Trial profile.
There were similar numbers of withdrawals in control and intervention groups. Of 1265 subjects at outcome, 92 failed to respond to the final questionnaire (7%). Their baseline characteristics and those of the population available for analysis are described in table 1. The numbers failing to respond at follow up were small, and most differences were non-significant, although they probably included more smokers. At completion of the study, there were no significant differences in age, sex, and general practice distributions, nor in prevalence of angina and previous myocardial infarction between patients from control and intervention groups.
Baseline characteristics of trial subjects who responded and failed to respond to the final questionnaire
COMPONENTS OF SECONDARY PREVENTION
The intervention improved all aspects of secondary prevention except smoking (table 2). Table 3 provides estimates of effect sizes on each secondary preventive measure, expressed as odds ratios after using logistic regression to adjust for baseline performance, age, sex, and practice.
“Appropriate” secondary prevention at baseline and outcome
Effect size of the intervention on aspects of “appropriate” secondary prevention (expressed as odds ratios, adjusted for baseline performance, age, sex, and practice)
The effects on blood pressure and lipid managements were reanalysed to determine whether they were due only to increased referral and checking, or showed better all round management. At outcome, few patients were being treated at specialist hypertension clinics (20 (3%) of 593 intervention group patients and 21 (4%) of 580 control group patients). Of 573 intervention group patients managed in general practice, 475 (83%) at baseline and 524 (91%) at outcome had blood pressures less than 160/90 mm Hg or were treated. Corresponding figures for 559 control group patients were 475 (85%) at both baseline and outcome. The adjusted odds ratio for better management with intervention was 2.52 (95% confidence intervals 1.63 to 3.90). There were similarly few patients treated at specialist lipid clinics (12 (2%) of 593 intervention group patients and 10 (2%) of 580 control group patients). Of 581 intervention group patients managed in general practice, 40 (7%) at baseline and 169 (29%) at outcome had cholesterol levels of 5.2 mmol/l or less or were treated. Corresponding figures for 580 control group patients were 47 (8%) and 91 (16%). The adjusted odds ratio for better management with intervention was 2.62 (1.90 to 3.61).
CUMULATIVE SCORE OF SECONDARY PREVENTION
Mean cumulative score for the intervention group was 3.31 at baseline and 3.89 at one year. For the control group, it was 3.23 at baseline and 3.29 at one year. The mean change in score was 0.59 for the intervention group and 0.06 for the control group (p < 0.001). Using analysis of covariance, adjusting for baseline performance, age, sex, and practice characteristics (size and location), we found the adjusted difference to be 0.55 (0.44 to 0.67) in favour of the intervention group (p < 0.001).
EFFECT OF PRACTICE BASELINE PERFORMANCE
Practices were divided into quartiles according to baseline performance for secondary analysis. There were significant improvements with intervention in all practice quartiles (table 4). Analysis of covariance with practice quartile as an additional factor found no significant interaction between the effect of intervention and practice quartile (F = 1.40, p = 0.241). However, the estimated difference in effect between bottom and top quartiles was 0.31 (−0.001 to 0.628), which approached significance (p = 0.051).
Change in cumulative secondary prevention score (baseline to outcome) grouped by practice baseline performance quartile
Discussion
“MEDICAL” COMPONENTS OF SECONDARY PREVENTION
The clinics improved all “medical” components of secondary prevention that we studied: aspirin, blood pressure, and lipid management. The benefits of aspirin and blood pressure treatment have been reported in meta-analyses: aspirin reduced vascular events by 33% in patients with angina2; blood pressure control as primary prevention reduced stroke by 42% and coronary heart disease by 14%16 and improved total mortality in subgroups with previous myocardial infarction.3 Both aspirin and blood pressure management are well established treatments and this was, perhaps, reflected in our study by the control group’s stability over the year. Aspirin management had more room to improve, as only two thirds used it at baseline; this starting point was not low, however, compared with other reports.17 The improvement in blood pressure management was more surprising, given the high performance at baseline. Our secondary analysis showed that the improvement was mostly the result of treatment and control, not just checking and referral.
By comparison, lipid lowering is a new intervention. Two large randomised trials—the 4S study in 1994 and the CARE study in 1996—reported that reductions in cardiovascular mortality of 42% and 20% could be achieved in coronary heart disease patients with raised and average cholesterol levels respectively.4 ,5 In the current study, baseline uptake of lipid lowering was low and there was a considerable increase over the study year in the control group, as might be expected when a new intervention is being disseminated. However, the study clinics led to a substantially more rapid uptake of this “new” component of secondary prevention.
“LIFESTYLE” COMPONENTS OF SECONDARY PREVENTION
Healthy behaviour promises considerable benefits to patients with coronary heart disease. After myocardial infarction, healthy diets (low in fat and high in fruit and vegetables) have significantly reduced cardiovascular mortality in randomised trials7 and exercise regimens have reduced sudden deaths by 36% and total mortality by 20% in a meta-analysis of randomised trials.6 In this study, the intervention group patients improved their physical activity and dietary habits significantly. Physical activity improved against the background of deterioration in the control group that might be expected with increasing age. Using the logistic regression equation to compare effects (odds ratios in table3), the clinics can be shown to have had the same effect as an age reduction of 17 years. The improvements we found in diet are in line with previous primary and secondary prevention studies.18 ,19 Our study has shown that dietary change can be achieved in a study population mostly over 65 years and independent of age.
One disappointing result was the absence of any effect on smoking cessation. Our sample size was not large enough to detect a small effect, but our finding adds to an increasing number of studies in general practice, mostly primary18 ,20 but also secondary19 prevention, that have failed to achieve significant benefit. Even pooling data on more than 16 000 subjects from 23 trials detected only a small effect.21 Our study suggests patients who continue to smoke despite a diagnosis of coronary heart disease may be as resistant to change as most other smokers have proved to be.
CUMULATIVE IMPACT
Overall, nurse led clinics increased secondary prevention in general practice. Within one year, most patients gained at least one effective component of secondary prevention, most often lipid, aspirin, or blood pressure treatment. Based on previous randomised trials and meta-analyses, cardiovascular events and mortality in these patients should be reduced by up to a third.2-7 ,16 These benefits are in marked contrast to the findings of two large randomised trials of primary coronary prevention in general practice, the British family heart study20 and OXCHECK,18 in which there was little benefit despite unrealistically heavy nurse commitment. There are, however, key differences between primary and secondary prevention. First, the former relies heavily on modifying lifestyle, whereas secondary prevention includes a large component of medical treatment; we found that medical treatment was easier to change than lifestyle. Secondly, the absolute benefits of any changes are greater in secondary prevention because the target population is at higher risk. Small changes are therefore more important. Both of the large primary prevention studies reported more benefit for higher risk patients.18 ,20
LIMITATIONS AND RELEVANCE
Data on behavioural practices were collected by self completion questionnaires and entered blind to group allocation to avoid interviewer or researcher bias. In order to obtain assessments that were as accurate as possible, we used instruments that have been validated previously.14 ,15 There remains, however, the possibility of self report bias; patients who attended the clinics may have reported preventive behaviour without practising it. Our failure to show any reduction in smoking, however, provides persuasive evidence that significant self report bias was unlikely. Our findings on behaviour were also consistent with a previous randomised trial in primary care in Belfast that reported improved diet and physical activity but no effect on smoking from health promotion to patients with angina.19
To avoid the problems associated with cluster randomisation (especially if practice performances at baseline are variable), we randomised by individual rather than practice. There may, therefore, have been some effect on control group patients by the presence of the intervention within their general practice: either dilution of effect by contamination, or exaggeration of effect if usual treatment was deliberately withheld from non-intervention group patients. Previous study of primary coronary prevention clinics suggests that the effect, if present, was more likely to be contamination, but that it was unlikely to have been substantial.20
Practices were recruited from a stratified random sample of all general practices in northeast Scotland and the recruitment rate was 68%.9 Of patients with identifiable coronary heart disease in general practice, 71% agreed to take part. Characteristics of respondents and non-respondents to the initial study invitation have been reported previously. Non-respondents were slightly less likely to have had aspirin or β blockers prescribed or their blood pressure or cholesterol levels checked in the past three years, but these differences were modest.9 Of those who agreed to take part in the study, there were few withdrawals. We believe, therefore, that the study practices and patients were reasonably representative of northeast Scotland.
In other areas, local factors could affect the performance of replicated clinics. We found that the most influential confounding variable was baseline performance: if this was already high then patients had less to gain. Baseline United Kingdom data on secondary prevention, however, were reported in the ASPIRE study and presented a similar suboptimal picture to the baseline position in northeast Scotland.9 ,10 In an attempt to assess the importance of baseline performance at the general practice level, we divided study practices into quartiles. Patients were found to benefit in all groups of practices, although most improvement probably occurred in those with the lowest starting point. It seems likely, therefore, that the results of this study will be relevant to other areas.
CONCLUSION
In view of the prevalence of coronary heart disease, most patients will continue to rely on general practitioners for day to day care, including secondary prevention.1 Our findings show that nurse led clinics in primary care can improve both medical and lifestyle components of secondary prevention effectively. They support the view that coronary prevention in general practice should focus on patients with manifest coronary heart disease in whom medium to long term mortality reductions of up to a third should be achievable.
Acknowledgments
Thanks to Sandra Skilling and Janis Bryant for help with data collection and Jeremy Grimshaw for help with study design.
Participating health visitors, practice nurses, and district nurses: June Anderson, Liz Brown, Mary Brown, Linda Bruce, Jas Burnett, Liz Clouston, Ann Darnley, Mary Duguid, Sheena Durno, Sandra Farquharson, Cath Gilbert, Gillian Grant, Linda Harper, Fiona Leitch, Heather MacAskill, Susan McSheffrey, Kirsten Masson, Pat Murray, Lynn Phillips, Hilary Plenderleith, Sheila Rattray, Marjorie Smith, Beth Struthers, Margo Stuart, Lynette Sykes, Fiona Travis, Ann Williams, Jean Wood.
Participating general practices: Aboyne Medical Practice, Benreay Practice, Dr Crowley, Danestone Medical Practice, Elmbank Group, Dr Grieve and Partners, Kemnay Medical Practice, Kincorth Medical Practice, King Street Medical Practice, The Laich Medical Practice, Dr MacFarquhar and Partners, Drs Mackie and Kay, Old Machar Medical Practice, Rubislaw Medical Group, Seafield Medical Practice, Skene Medical Practice, Spa-Well Medical Group, Turriff Medical Practice, Victoria Street Medical Group.
The study was funded by the Health Services and Public Health Research Committee of the Chief Scientist Office at the Scottish Office and Grampian Healthcare Trust.