Article Text

Abstract
OBJECTIVE To examine the management and outcome of an unselected consecutive series of patients admitted with acute myocardial infarction to a tertiary referral centre.
DESIGN A historical cohort study over a three year period (1992–94) of consecutive unselected admissions with acute myocardial infarction identified using the HIPE (hospital inpatient enquiry) database and validated according to MONICA criteria for definite or probable acute myocardial infarction.
SETTING University teaching hospital and cardiac tertiary referral centre.
RESULTS 1059 patients were included. Mean age was 67 years; 60% were male and 40% female. Rates of coronary care unit (CCU) admission, thrombolysis, and predischarge angiography were 70%, 28%, and 32%, respectively. Overall in-hospital mortality was 18%. Independent predictors of hospital mortality by multivariate analysis were age, left ventricular failure, ventricular arrhythmias, cardiogenic shock, management outside CCU, and reinfarction. Hospital mortality in a small cohort from a non-tertiary referral centre was 14%, a difference largely explained by the lower mean age of these patients (64 years). Five year survival in the cohort was 50%. Only age and left ventricular failure were independent predictors of mortality at follow up.
CONCLUSIONS In unselected consecutive patients the hospital mortality of acute myocardial infarction remains high (18%). Age and the occurrence of left ventricular failure are major determinants of short and long term mortality after acute myocardial infarction.
- myocardial infarction
- mortality
- thrombolysis
Statistics from Altmetric.com
Although the mortality from acute myocardial infarction is declining, it remains a leading cause of mortality and morbidity in most industrialised nations. The decline in mortality has been ascribed to a combination of community-wide preventive strategies and improved treatment.1 Recent large scale randomised controlled thrombolytic trials have reported 30 day mortalities of 6–10% with mortality as low as 2.5% in trials of primary angioplasty.2 However, these trials have enrolled a highly selected group of patients and have mostly excluded the elderly. In clinical practice, many patients do not receive optimal treatment, including thrombolysis. Series from North America and Europe suggest that thrombolysis rates are in the region of 25%.3 In addition many patients are not managed in coronary care units and many are elderly.4-6 Thus the hospital mortality of unselected patients with acute myocardial infarction may be considerably higher than suggested by the results of large scale trials of thrombolysis and primary angioplasty.
In this study we examined the short and long term mortality of a consecutive unselected series of patients admitted to a tertiary referral centre with acute myocardial infarction and we identified clinical predictors of hospital mortality in this group. We also determined the hospital mortality of a series of patients admitted to a non-tertiary referral hospital during an overlapping time period.
Glossary of acronyms
- ICD:
- International classification of diseases
- ISIS:
- International study of infarct survival
- GUSTO:
- Global utilisation of streptokinase and tissue plasminogen activator for occluded coronary arteries
- MONICA:
- Multinational monitoring of trends and determinants in cardiovascular disease
- OASIS:
- Organisation to assess strategies for ischemic syndromes
- TAMI:
- Thrombolysis and angioplasty in myocardial infarction
- TIMI:
- Thrombolysis in myocardial infarction
- VANQWISH:
- Veterans Affairs non-Q wave infarction strategies in hospital
Methods
Patients were identified for inclusion using the HIPE (hospital inpatient enquiry) database, which includes demographic, diagnostic, and procedural data information coded according to ICD-9. All patients admitted between June 1992 and December 1994 with a diagnosis of acute myocardial infarction were included for medical record review. Patients were excluded if there was an obvious coding error as determined by medical record review, if transferred from another hospital (to avoid tertiary referral bias), or if myocardial infarction developed following coronary bypass grafting (CABG) or invasive cardiac procedures. Patients were not excluded if they developed myocardial infarction while in hospital for another reason, but were excluded if the index admission had been a tertiary referral.
Using identical methods, all patients admitted to a county hospital without cardiac catheterisation facilities during the year 1994 were included in a separate database. Inclusion and exclusion criteria, where relevant, were similar.
This was a historical cohort study. Demographic, clinical, management, and survival data were obtained through the hospital computer system and through detailed medical record review identifying 78 variables of interest. Follow up data were obtained by a combination of repeat medical record review, tracking of admission/outpatient and accident and emergency visits through the hospital computer system, and contacting general practitioners regarding patients who had ceased to attend the hospital. The primary end point was that the patient was discharged alive from hospital at the end of the relevant admission. Secondary end points were age and sex distribution, risk factor distribution, management, use of thrombolysis and other evidence based medications, resource utilisation, and survival for a follow up period of up to four years.
Reliability of HIPE data was assessed by analysis of 100 randomly selected eligible cases from each series according to the MONICA manual criteria for definite or probable acute myocardial infarction.
STATISTICAL ANALYSIS
All data were transferred from precoded data sheets to a computer database for analysis using SAS for PC.7 Predictors of mortality were identified using parametric and non-parametric tests as appropriate (Student’s t, χ2, and Fisher’s exact test) and multivariate analysis using a logistic regression model. Life table methods were used to produce survival curves for follow up data.
Results
During the study periods, 1059 eligible patients were admitted to the tertiary centre and 100 to the non-tertiary centre (1994 only). Reliability of HIPE data was high, with 91% and 95% fulfilling criteria for definite or probable myocardial infarction among the tertiary and non-tertiary centre patients, respectively.
TERTIARY CENTRE RESULTS
Table 1 summarises clinical and demographic features, complication rates, and outcomes of patients admitted with acute myocardial infarction. Overall hospital mortality was 18%. Thirty per cent of patients were over 75 years and 30% were not admitted to coronary care. The mean age of patients managed outside the CCU was 72.5 years,v 65 years among those admitted to the unit (p < 0.001). The overall thrombolysis rate was 28%, the majority (85%) receiving streptokinase. Left ventricular failure (defined for this study as the documentation of the presence of bibasal crepitations or a third heart sound) occurred in 44% of patients. Ventricular arrhythmias (ventricular fibrillation, sustained ventricular tachycardia, or recurrent non-sustained ventricular tachycardia requiring treatment) occurred in 18% of cases.
Demographic data, risk profile, and complications
The rate of predischarge coronary angiography was comparatively high (32%), with a further 5.2% scheduled to have angiography as outpatients. Patients managed outside the CCU were less likely to undergo subsequent angiography (17.6% v38.4%, p < 0.001), echocardiography (13.5%v 28.4%, p < 0.001), and revascularisation (20.2% v 10.2%, p < 0.001). Of patients undergoing angiography, 42% had a patent infarct related artery, 79% had multivessel disease, and 4% had left main stem disease. Twenty seven per cent of patients undergoing angiography were recommended for percutaneous revascularisation and 30% for coronary bypass grafting.
NON-TERTIARY CENTRE RESULTS
During 1994, 100 patients were admitted with acute myocardial infarction. Mean age was 64 years (v 67 years in the tertiary centre series). In 85% of cases (v 44% of cases from the tertiary centre series) the index infarct was a first infarct, 77% were managed in CCU, and 30% were given thrombolysis. Sixteen were referred for coronary angiography. Overall hospital mortality was 14%.
Distribution of risk factors
Smoking history (63%), diabetes mellitus (28%), family history (22%), and hypertension (32%) did not differ significantly from the tertiary centre series. The occurrence of left ventricular failure (33%), ventricular arrhythmias as defined above (11%), and postinfarction angina or reinfarction (15%) were lower than in the tertiary centre (45%, 18%, and 34%, respectively).
PREDICTORS OF HOSPITAL MORTALITY
These are shown in table 2. The mean age of patients dying was 73 years v 67 years in patients surviving. Among the tertiary centre patients age was a predictor of mortality in hospital in both univariate (p < 0.001) and multivariate analysis (p < 0.001). Other predictors of hospital mortality by univariate analysis included sex, the use of thrombolysis, and the occurrence of left ventricular failure, cardiogenic shock, ventricular arrhythmias, and heart block requiring temporary pacing. Other independent predictors of mortality following multivariate analysis were left ventricular failure, shock, ventricular arrhythmias, management outside the CCU, and the development of reinfarction.
Predictors of early mortality
FOLLOW UP DATA
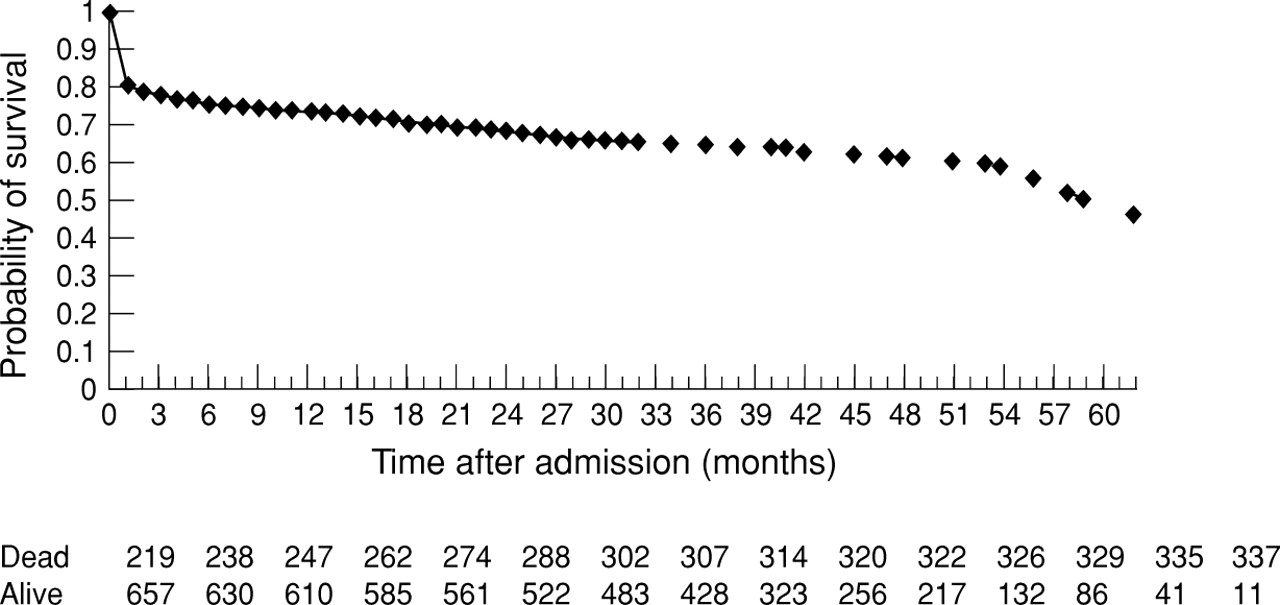
Follow up data were obtained for 99.5% of patients surviving to hospital discharge. Median duration of follow up was 36 months, the longest follow up period being 64 months. Kaplan–Meier curves were constructed for patient survival using life table analysis. Probability of survival at six months was 75%, at one year 73%, at two years 69%, and at five years 52% (fig 1). Factors associated with mortality at follow up in univariate analysis were female sex, previous myocardial infarction, age, absence of a smoking history, absence of a family history, presence of diabetes mellitus, lack of thrombolysis, the occurrence of left ventricular failure, ventricular arrhythmias, heart block, and not being discharged on aspirin treatment (table 3). Following multivariate analysis only age (p < 0.001) and left ventricular failure (p < 0.01) were predictive of mortality at follow up. Five year survival and the effect of left ventricular failure on survival are shown in figs 1 and 2, respectively.
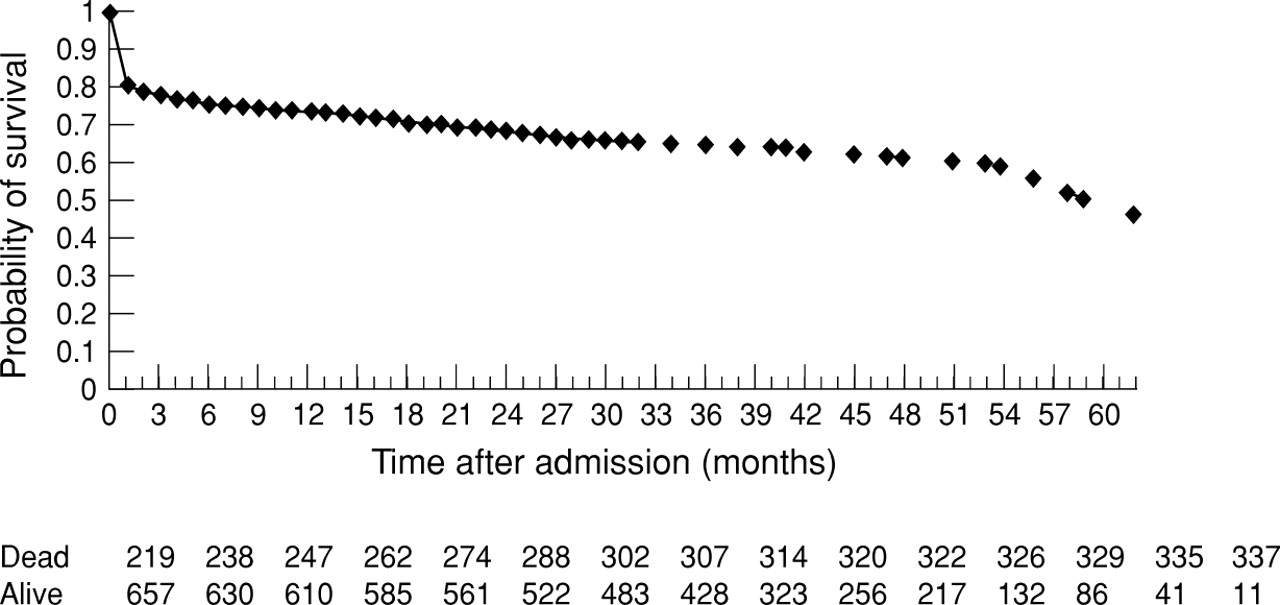
Kaplan–Meier curve indicating probability of survival following admission for acute myocardial infarction.
Univariate and multivariate predictors of death at follow up

{kind=link}
{kind=link}
Kaplan–Meier curve indicating effect of left ventricular failure (LVF) on probability of survival.
Discussion
In this study of unselected patients from a centre with coronary intervention facilities, the hospital mortality of acute myocardial infarction was 18%. This is a reflection of the design of the study which included all ages and all hospital cases of acute myocardial infarction, not simply those admitted to coronary care. Accordingly 30% of patients were over 75 years and mortality in this group was 30%, as opposed to 14% in those under 75. Other studies reporting the hospital mortality of acute myocardial infarction since the introduction of thrombolysis have produced disparate results, with hospital mortalities ranging from 8.4% to 23%. This disparity is determined by differences in study populations, with studies limited to younger ages1 or coronary care cases8-12showing lower mortality than studies of unselected cases.13-17 The present study is a relatively large all inclusive study of acute myocardial infarction in the thrombolytic era, which shows that even in a tertiary referral centre with a high intervention rate acute myocardial infarction continues to carry a poor short and long term prognosis.
In this study we identified univariate and multivariate predictors of hospital and follow up mortality. The poor prognosis associated with left ventricular failure, cardiogenic shock, and ventricular arrhythmias is well recognised. Similarly, consistent with these results, advanced age is a recognised independent predictor of mortality following acute myocardial infarction4 ,18-20as well as being associated with undertreatment in terms of thrombolysis4 ,5 and admission to coronary care.4 The issue with regard to sex is more complex. Many of the available reports date from the prethrombolytic era or come from randomised treatment trials and are conflicting over whether female sex is an independent risk factor for mortality following acute myocardial infarction.21 ,22 The results of this study in unselected patients are similar to recent reports from the GUSTO, TAMI, and ISIS investigators in that female sex was not an independent predictor of mortality following multivariate analysis.23
Treatment outside coronary care was associated with reduced survival in univariate and multivariate analysis. Patients managed outside the CCU were older and were not given thrombolysis, but the increased mortality persisted after adjustment for these variables. Although potential contributors to a higher mortality outside CCU—such as uncertainty regarding the diagnosis and delayed presentation—were not measured, these data raise the possibility that overall outcome following acute myocardial infarction could be improved by increasing the rate of management in CCU. Such an improvement has been shown in a study examining the effects of a policy encouraging admission to CCU on rates of thrombolysis and outcomes among elderly patients.24
Thrombolytic treatment was associated with improved outcome in univariate but not multivariate analysis. While the overall rate of thrombolysis of 25% was low, it compares favourably with North America and Europe, where reported rates for a similar time period have ranged from 13% to 52%.25 It is estimated that the maximum rate of thrombolysis is about 55%, allowing for delays of presentation and difficulties of early diagnosis.3 The major influences on the rate of thrombolysis are the presence of ECG criteria for thrombolysis and the time of presentation with acute myocardial infarction. Among this population, ECG criteria (ST elevation or bundle branch block) were present in only 42.8% of patients. It is not known what proportion of these presented within the time window for thrombolysis. Clearly the proportion of unselected patients presenting with standard criteria is low. The use of thrombolysis did not contribute significantly to the stroke rate of 3.6% as only 16% of all strokes occurred in patients who had been given thrombolysis.
There was also evidence for underutilisation of other drug treatments. The rate of aspirin use was 83%, which is comparable with data from other centres26 but suboptimal given the low risk and potential benefits of aspirin therapy. The rate of early β blocker prescription (15%) compares poorly with North American surveys27 and the rate of angiotensin converting enzyme (ACE) inhibitor use (20% at discharge), although higher, was also suboptimal given the number of survivors with clinically documented heart failure following acute myocardial infarction (44%). The rate of early use of cholesterol lowering treatment was low (3.6%) but this study predated the publication of the first trial of statin therapy in secondary prevention of acute myocardial infarction,28 and no data are available on prescription of statins at follow up.
Cigarette smoking was a univariate predictor of lower hospital mortality. This phenomenon has been observed in several large thrombolytic trials29 and may reflect younger age at presentation in smokers (mean age of smokers in this study was 65 yearsv 70 years in non-smokers), a lower prevalence of other risk factors,30 a higher proportion of arrhythmic deaths before reaching hospital,31 reversal of risk following cessation of smoking during the hospital admission,32 or a better response to thrombolysis owing to the predominantly thrombotic nature of the lesion.33 A family history of premature coronary disease was also associated with a better outcome. Again this reflects the younger age of patients with a family history (mean age 62 years v 70 years in the remaining population), and may be a result of earlier presentation in patients with a family history or of more difficulty in eliciting a family history from elderly patients.
The observation of a higher hospital mortality in the tertiary referral centre, where the coronary intervention rate was high, might be construed as evidence against the benefits of coronary interventions in acute myocardial infarction. Recent reports from the VANQWISH34 and OASIS35 trials, and previously from trials such as TIMI II, have questioned the benefit of coronary interventions in acute coronary syndromes and acute myocardial infarction.36 ,37 However, data from the GUSTO trial suggest higher morbidity among patients undergoing fewer interventions,38 and a study of varying practices in 16 Kaiser Permanente hospitals showed a significant inverse correlation between higher intervention rates and mortality.39 In the present study, the apparent paradox of a higher mortality in the centre with the higher intervention rates may be explained by a bias in demographics. The non-tertiary centre patients were considerably younger, they had fewer comorbidities, and more of these patients were managed in coronary care and received thrombolysis. The non-tertiary centre served a partly rural catchment area where greater distances and differing practices may have resulted in fewer older patients with acute myocardial infarction being sent to hospital. Furthermore the greater distances involved may have resulted in fewer patients with acute myocardial infarction reaching hospital alive, ultimately lowering the hospital mortality. The greater age of the tertiary hospital patients may also reflect the demographics of the catchment area, which has the highest proportion of residents over 65 years in the country (data not shown), or it may reflect differences in case finding or coding practices between the two hospitals. Thus the higher mortality in the centre with higher intervention rates is primarily evidence of the effect of age on the hospital mortality of acute myocardial infarction.
In conclusion, despite advances in the treatment of acute myocardial infarction, in unselected consecutive patients the hospital mortality remains high. Age is a major baseline determinant of short and long term mortality after acute myocardial infarction.
Acknowledgments
We thank Bernadette Egan, Jackie Brennan, and Anna Hennessey for assistance with data collection and coding, and Dr Mark M Gallagher for critically reviewing the manuscript.