Article Text

Abstract
A 2 year old girl is reported in whom deployment of the Amplatzer ductal occluder caused significant aortic obstruction, requiring surgical removal of the device. This case emphasises the need for careful echocardiographic and angiographic assessment of the position of the Amplatzer ductal occluder before and after detaching the device from its delivery system, with particular emphasis on the position of the aortic retention ring. Careful assessment of ductal anatomy must guide case selection.
- interventional catheterisation
- Amplatz ductal occluder
- coarctation of the aorta
- congenital heart disease
Statistics from Altmetric.com
- interventional catheterisation
- Amplatz ductal occluder
- coarctation of the aorta
- congenital heart disease
A female infant born at 28 weeks’ gestation was noted to have a murmur on discharge from the neonatal unit. Although her initial echocardiogram showed a patent arterial duct (PDA), she was asymptomatic and treatment was deferred. She was admitted for transcatheter PDA occlusion at 2 years of age (body weight 12.3 kg). On examination, there was a grade 3/6 continuous murmur at the upper left sternal edge and a mid-diastolic apical flow murmur with bounding peripheral pulses. Echocardiography showed a moderate sized PDA. Detailed ductal morphology could not be assessed because of poor image quality. There was mild left ventricular volume overload with no evidence of significant pulmonary hypertension.
At cardiac catheterisation, aortography demonstrated a long PDA with a narrowing at the pulmonary artery end remote from the anterior border of the trachea (PDA type E according to the classification adopted by Krichenko and colleagues1). The duct joined the aorta at a more acute angle than usual (fig 1A). The PDA was 11.6 mm in length and had a diameter of 3–4 mm at the aortic end; the diameter of the narrowest point at the pulmonary artery end was 2 mm. Later in the procedure, angiography showed ductal spasm, which indicated that the minimum diameter was variable. There was no gradient between the ascending and descending aorta, and pulmonary artery pressures were normal. The pulmonary to systemic flow ratio (Qp/Qs) was 1.3.

(A) Aortogram in the lateral projection demonstrating the PDA. The angle between the isthmus and the PDA (arrow) is more acute than usual (PA, pulmonary artery; DAo, descending aorta). (B) The Amplatzer ductal occluder has been deployed across the duct and remains attached to its delivery wire. There is no residual left to right shunt and the device appears to be in an acceptable position. (C) Repeat aortogram after detaching the device from the delivery wire. The more proximal position of the catheter results in better opacification of the space anterior to the aortic retention disc (arrowhead) demonstrating that the device has tilted out into the aorta and is causing obstruction.
The procedure used for implanting an Amplatzer ductal occluder (fig 2) has been detailed in a recent publication.2 In this case, the duct was crossed from the venous side and a 6–4 mm Amplatzer ductal occluder was placed in such a way that the aortic retention disc was within the body of the PDA rather than at the aortic ampulla, owing to the anatomy of the ductus. However, the device used was too small and was easily pulled into the pulmonary artery without resistance. It was then successfully withdrawn. An 8–6 mm Amplatzer ductal occluder was then placed across the PDA, with the aortic retention disc snug against the aortic end of the ductal ampulla. The postocclusion aortogram showed no residual left to right shunting and the device seemed to be in a satisfactory position (fig 1B). The Amplatzer ductal occluder was released from its delivery system and remained in a stable position. Echocardiography showed the device in situ with no residual shunting and no obstruction to the left pulmonary artery. Unfortunately, Doppler studies of the descending aorta revealed a peak velocity of 2.6 m/s with a small but definite delay in diastolic decay, suggesting aortic obstruction. Repeat aortography with a pigtail catheter in the proximal transverse aortic arch showed that the superior rim of the aortic retention disc projected into the aortic lumen, obstructing approximately half its diameter (fig 1C). Catheter withdrawal across the site of the narrowing showed a gradient of 28 mm Hg. Attempts to retrieve the device with a 10 mm gooseneck snare were not successful because the screw by which the device was attached to the delivery system was recessed (in accordance with its design), leaving no projection that could be securely gripped by the snare. The patient had surgery to retrieve the Amplatzer ductal occluder from the ductus without difficulty, and the PDA was successfully ligated without complication.

{kind=link}
{kind=link}
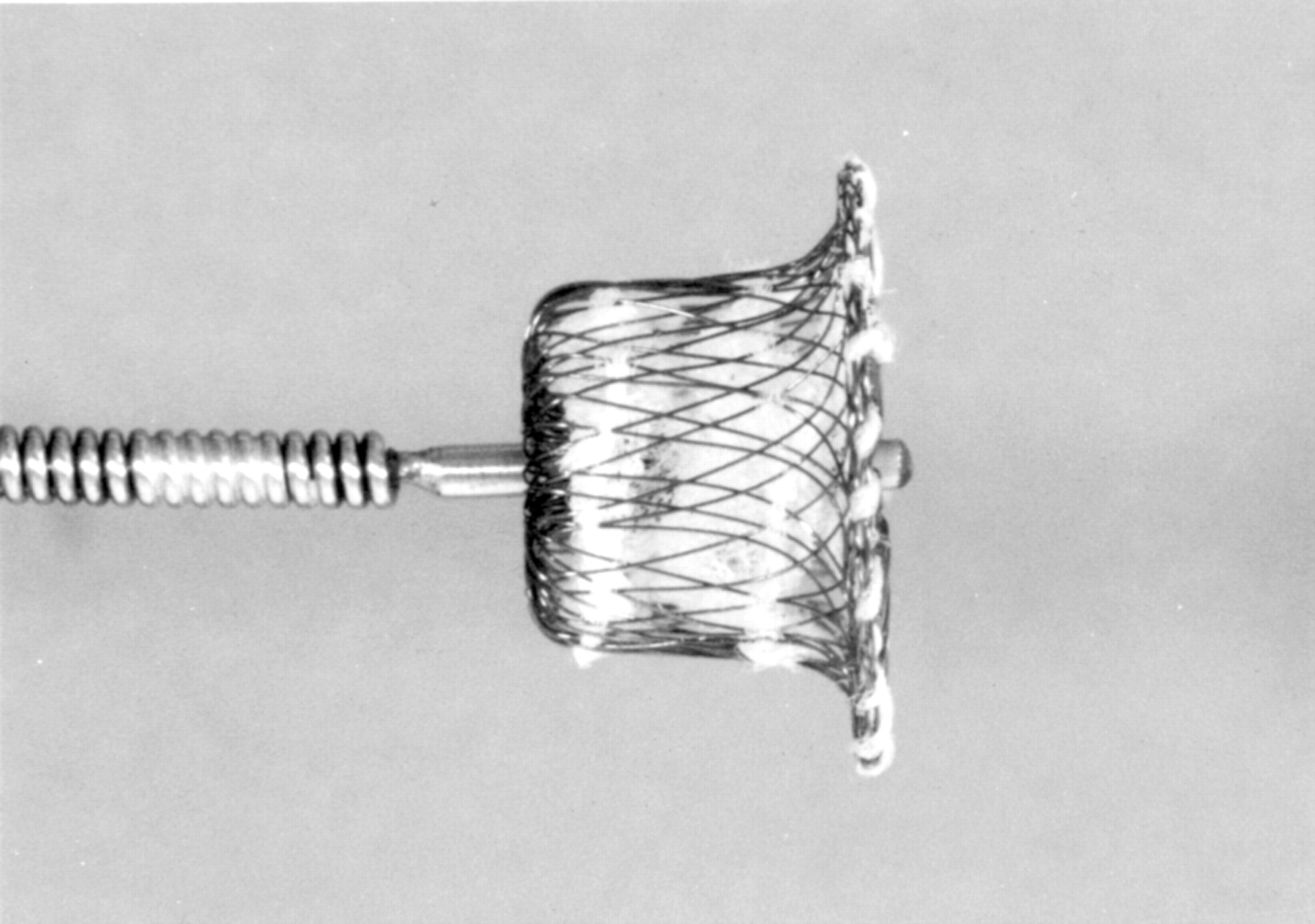
Amplatz ductal occluder device.
Discussion
Transcatheter occlusion of a moderate or large sized patent arterial duct (⩾ 3 mm) is often technically demanding when using multiple coils or a Rashkind PDA occluder. The incidence of residual shunting is high with the Rashkind device3 and there is high risk of embolisation with multiple coils.4 ,5 The Amplatzer ductal occluder is a new device that is designed to improve occlusion rates and avoid the problems of earlier techniques. It is a self expanding mushroom shaped device made from Nitinol wire mesh, with a thin aortic retention disc designed to secure positioning in the aortic ampulla. It was initially developed in a canine model with encouraging results.6 The first series of patients in which the Amplatzer ductal occluder was used to close moderate to large sized PDAs was reported recently.2 Experience with the device is still limited and complications have not been documented.
Our case shows that it is possible for the aortic retention disc to project into the descending aorta, causing aortic obstruction. It should be noted that, in our patient, the ductus was long and unusually configured; the angle between the ductus and the aorta proximal to the ductus was far more acute than usual, tilting the superior rim of the aortic retention disc into the distal aortic arch as the device was pulled back into the duct (fig 1C). We suggest that it is this ductal angulation, rather than any problem with the size of the device, that causes iatrogenic aortic coarctation. The device should not be used where the duct joins the aorta at a particularly acute angle, or, in such cases, the entire device (including the aortic retention disc) should be deployed within the body of the duct.
This case also emphasises the need for careful assessment of device position before and after release. In our view, device insertion should be followed by aortography which is best performed with the pigtail catheter in a proximal position in the aortic arch. More distal catheter positions do not opacify the space between the superior rim of the aortic disc and the anterior wall of the aorta, masking the full extent of incursion of the aortic retention disc into the aortic lumen. Therefore, it is imperative that a full assessment of the placement of the device is made before release from the delivery system as the design makes subsequent retrieval extremely difficult.