Article Text

Abstract
OBJECTIVE To assess the pressure and flow velocity relations and respiratory variability of the systemic venous and hepatic venous return in patients with univentricular circulation.
PATIENTS 15 selected patients who had undergone cavopulmonary anastomosis (10) or atriopulmonary anastomosis (5). Mean age at operation was 55.1 months (range 9 to 145). Studies were done at 75.5 (32.6) months (mean (SD)) after the operation.
SETTING Tertiary referral centre.
METHODS Patients were studied using simultaneous recordings of ECG, pressure trace, respirometer trace, and pulsed Doppler echocardiography. Mean systemic venous pressure and pulmonary vascular resistance did not differ significantly between the two patient groups.
RESULTS After total cavopulmonary anastomosis, systemic venous pressure tracings showed a flattened pressure curve without any dependence on cardiac or respiratory cycle. After atriopulmonary anastomosis, right atrial pressure tracings showed a significantly higher “a” wave corresponding to atrial contraction, without any respiratory variability. Pulsed Doppler examination of the superior and inferior caval vein and hepatic vein after total cavopulmonary anastomosis did not show a reverse flow after atrial contraction. The inspiratory to expiratory velocity ratio of antegrade flow revealed a significant dependence of flow on changes in intrathoracic pressure in the intra-atrial tunnel, caval veins, and hepatic vein. During expiration, decrease or cessation of antegrade hepatic venous flow was documented. After an atriopulmonary anastomosis, there was a biphasic antegrade venous flow pattern without significant respiratory variation.
CONCLUSIONS After total cavopulmonary anastomosis, there was marked respiratory dependence of systemic and hepatic venous return, whereas after an atriopulmonary anastomosis venous flow pattern varied according to cardiac cycle and pressure trace. The effects of total cavopulmonary anastomosis on venous return might counteract its other haemodynamic advantages.
- Fontan operation
- Doppler echocardiography
- systemic venous flow pattern
Statistics from Altmetric.com
Several modifications of the Fontan-type operation have been developed for the management of univentricular circulation. There are conflicting reports about the contribution of right atrial contraction to supporting forward flow within the pulmonary arteries after atriopulmonary anastomosis, and about uncompromised passive streaming in a total cavopulmonary connection.1-3 Doppler echocardiographic evaluation after an atriopulmonary anastomosis has shown that pulmonary blood flow is biphasic and related to both atrial and ventricular contraction.4 ,5 The act of breathing provides an additional energy supply to pulmonary blood flow, accelerating the blood by inspiratory suction as documented by the increase in forward flow with inspiration during atrial contraction.6-8 In contrast, after total cavopulmonary anastomosis evaluation of pulmonary artery flow showed a continuous flow pattern with mild biphasic pulsation and peak flow at systole.9-11 When the right heart is completely bypassed, as in patients with left atrial isomerism after the total cavopulmonary shunt procedure, the pulmonary blood flow is exclusively dependent on changes in intrathoracic pressure, as shown by Doppler echocardiography.12 ,13 In this situation with complete loss of pulsatility in the pulmonary arterial flow, long term effects on the pulmonary vasculature and the development of arteriovenous malformations remain an important possibility.2 ,14
Although the potential implications of the type of Fontan procedure on the systemic venous and hepatic venous blood flow have been discussed,4 ,11 the blood flow patterns have not been formally assessed and compared in total cavopulmonary anastomosis and atriopulmonary anastomosis. Our aim in this study was to assess the pressure and flow velocity relations and respiratory variability of the systemic venous and hepatic venous return in patients with univentricular circulation.
Methods
STUDY GROUP
We studied 15 selected patients from a group of 60 patients who underwent postoperative cardiac catheterisation for various indications. Patients were studied 75.5 (32.6) months (mean (SD)) after Fontan-type procedure. Written informed consent was obtained from the patients’ parents and the study was approved by the scientific committee of children’s hospital. None of the patients included in this study had clinical signs of compromised systemic ventricular function, significant interatrial right to left shunting, or atrioventricular valve incompetence of more than mild degree on echocardiography. All patients were in sinus rhythm during the measurements.
Patterns of venous blood flow and pressure recordings were documented simultaneously during spontaneous respiration for assessment of respiratory variation of the velocity flow profiles and pressure traces. Table 1 summarises the patient data, including diagnosis, preoperative haemodynamic data, and surgical procedures. A total cavopulmonary anastomosis was performed in 10 patients (cases 1–10). Five patients underwent an atriopulmonary anastomosis (cases 11–15).
Characteristics of the patients, preoperative haemodynamic data, and surgical techniques
CARDIAC CATHETERISATION
Cardiac catheterisation was performed to evaluate the postoperative state. Cardiac output was measured using the Fick principle. Pressures were recorded through a fluid filled catheter connected to a strain gauge. Measurements were obtained for the mid-portion of the intra-atrial tunnel in patients after total cavopulmonary anastomosis or the right atrium in patients after atriopulmonary anastomosis for calculation of mean pressure, the “a” wave, and the “v” wave separately for inspiration and expiration. As pressure traces of the superior and inferior caval veins mirror right atrial pressure events, pressure tracings in these vessels were analysed in the same way as the atrial pressure tracings for mean pressure, “a” wave, and “v” wave. A stenosis at the anastomosis between the functionally right atrium and pulmonary artery system was ruled out by pressure measurements of the proximal right and left pulmonary artery, as well as by selective angiography.
DOPPLER ECHOCARDIOGRAPHY
The Doppler echocardiographic study was performed with a Hewlett-Packard Sonos 1000 ultrasound system (Hewlett-Packard Inc, Andover, Massachusetts, USA), using a 3.5 MHz or 2.5 MHz transducer. The examinations were performed with the patients supine and breathing quietly with simultaneous systemic venous/right atrial pressure recordings. The subxyphoid position of the transducer was chosen to record the pulsed Doppler flow signal from the inferior caval vein and hepatic vein, from different levels of the intra-atrial tunnel and right atrium, respectively. Guided by colour flow mapping, the sample volume was positioned at the centre of the colour signal so as to select the smallest angle of incidence between blood flow and Doppler beam. The pulsed Doppler flow signal was recorded from the inferior caval vein (approximately 1–2 cm distal to its junction with the right atrium), and the hepatic vein (at 1 cm distal to its junction with the inferior caval vein). A sample volume as large as one third of the vessel’s diameter ensured that the lumen of the hepatic vein remained within the “gate” throughout the respiratory cycle. Suprasternal transducer positions were chosen for examination of the distal part of the superior caval vein or the corresponding segment near the cavopulmonary anastomosis. Velocity reversals at the time of atrial contraction were calculated from recordings of the caval veins and the hepatic vein.
Measurements on echocardiograms were made with a simultaneous ECG, pressure recording, and respiratory motion trace. Recordings were made at a paper speed of 50 or 100 mm/s. Peak forward flow velocity during inspiration and expiration was determined for further analysis of respiratory variability. Measurements were obtained over four to six cardiac cycles (two to three during inspiration and expiration, respectively). In patients with a total cavopulmonary anastomosis only the maximum velocity of forward flow in the caval and hepatic veins was analysed, depending on the respiratory cycle, as there was only slight pressure undulation and no fixed relation to the cardiac cycle. In patients who underwent an atriopulmonary anastomosis, maximum velocity of forward flow in the superior and inferior caval vein and the hepatic vein during inspiration or expiration could be calculated separately for systole and diastole. Peak forward flow velocity at systole was chosen for further analysis.
STATISTICAL ANALYSIS
Data are expressed as mean (SD) where appropriate. All data were analysed using SPSS statistical software. Numerical data were analysed with the unpaired Student’s t test. A probability (p) value of < 0.05 was considered significant.
Results
STUDY GROUP CHARACTERISTICS
Patients who received a total cavopulmonary anastomosis for definitive palliation of univentricular circulation were younger at operation (mean 36 (19) months v 93 (31) months, p = 0.001) and had a shorter postoperative follow up (mean 57 (21) months v 112 (12) months, p < 0.001) compared with patients who had an atriopulmonary anastomosis. The cardiac index ranged from 2.5 to 4.2 l/min/m2 (mean 3.4 (0.5) l/min/m2) in patients after a total cavopulmonary anastomosis, and from 2.0 to 3.1 l/min/m2 (mean 2.4 (0.4) l/min/m2) in patients after an atriopulmonary anastomosis (p = 0.005) (table 2). The mean systemic venous pressure (10.0 (1.7)v 10.8 (2.8) mm Hg, p = 0.511) and the pulmonary vascular resistance (1.79 (0.6) v1.74 (1.0) U/m2, p = 0.912) did not differ between the two patient groups, nor did the arterial oxygen saturation (94.5 (2.1)% v 94.4 (2.3)%, p = 0.934) or mean systemic ventricular end diastolic pressure (4.1 (1.2)v 5.0 (2.0) mm Hg, p = 0.293).
Haemodynamic measurements and simultaneous pulsed wave Doppler flow measurements at rest during quiet respiration
POSTOPERATIVE CATHETERISATON DATA
In patients after a total cavopulmonary anastomosis (n = 10), pressure tracings from the caval veins and intra-atrial tunnel showed a flat curve (fig 1), without significant pressure differences allowing for differentiation between the “a” wave and the “v” wave. Pressure tracings from the proximal pulmonary arteries were comparable, showing no differences during systole and diastole. A slight pressure decrease during inspiration resulted in an inspiratory to expiratory mean pressure ratio ranging from 0.72 to 1.08 (mean 0.88 (0.1)) (table2).

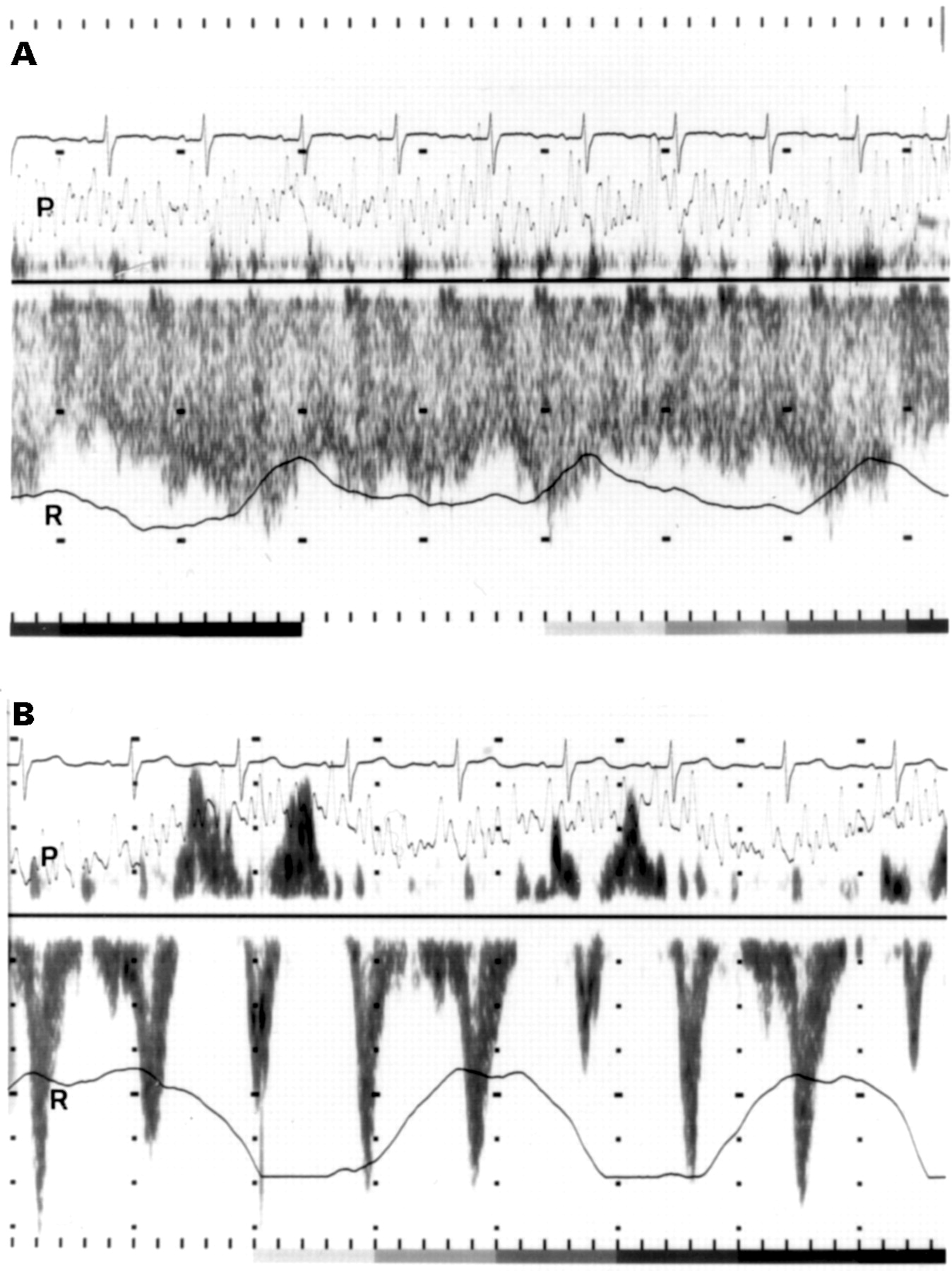
Pulsed Doppler recording from the superior caval vein (A) and hepatic vein (B) in a patient after total cavopulmonary anastomosis. The pressure trace within the intra-atrial tunnel showed a flattened curve. The superior caval vein flow profile had some pulsatility with respiratory variability. The hepatic venous flow mirrors respiratory dependence, with cessation or even reversal of flow at expiration.
In patients after an atriopulmonary anastomosis (n = 5), the pressure tracings of the right atrium and of the superior and inferior caval vein all showed a prominent “a” wave corresponding to atrial contraction, without any respiratory variability (fig 2). The inspiratory to expiratory mean pulmonary artery pressure ratio ranged between 1.0 and 1.07 (mean 1.0 (0.03)), indicating less respiratory variability than in patients after total cavopulmonary anastomosis (p = 0.03) (table 2). The pulmonary artery pressure tracing showed a decrease during ventricular systole with an increase and maximum pressure in diastole.

{kind=link}
{kind=link}
Pulsed Doppler recording from the superior caval vein (A) and hepatic vein (B) in a patient after an atriopulmonary anastomosis. Simultaneous right atrial pressure curves (P) and respiratory traces (R) are illustrated. Venous flow pattern showed two flow peaks at systole and diastole, with regurgitant peak flow after the P wave on the ECG.
Comparing both surgical techniques (table 2), the inspiratory to expiratory pressure ratio for the mean pulmonary artery pressure and the mean inferior caval vein pressure were lower in patients after total cavopulmonary anastomosis (p = 0.03 and p = 0.01, respectively). During inspiration the “a” wave of the right atrial, superior and inferior caval vein pressure trace (p < 0.03) and the diastolic pulmonary artery pressure (p = 0.03) were lower in patients after total cavopulmonary anastomosis.
DOPPLER ECHOCARDIOGRAPHY
Analysis of caval vein velocities after total cavopulmonary anastomosis (table 2) showed a retrograde flow after atrial contraction in only two patients during expiration. In the other patients flow patterns of the caval veins did not show any reverse systemic venous flow related to atrial contraction. In six of the 10 patients retrograde flow in the hepatic veins was predominantly observed during expiration.
The inspiratory to expiratory velocity ratio calculated from the peak flow velocity during each respiratory cycle showed an increase during inspiration within the intra-atrial tunnel as well as in the systemic and hepatic venous return. At maximum this ratio was 5.0 for the intra-atrial tunnel, and 2.0 and 3.0 for the superior and inferior caval vein, respectively; this mirrors the marked respiratory dependence of blood flow, which was associated with only small simultaneous pressure changes. The flow profile of the superior caval vein was continuous, the Doppler shift never reaching baseline (fig1A). During expiration, a decrease (eight patients) or cessation (two patients) of antegrade hepatic vein flow was documented (fig 1B). At maximum, the inspiratory to expiratory velocity ratio for the hepatic vein was 4.0.
After an atriopulmonary anastomosis, atriocaval retrograde flow of variable significance occurred during atrial systole (fig 2A); peak reverse velocity of flow within the superior and inferior caval vein varied from 0.06 to 0.40 m/s (table 2). Analysis of the caval vein velocity profiles showed a biphasic flow pattern with peak systolic velocity greater than peak diastolic velocity. Determination of maximum velocities during ventricular systole revealed an inspiratory to expiratory velocity ratio of less than 1.5. The hepatic venous flow pattern showed a reverse velocity peak at atrial contraction (table 2). Cessation of antegrade flow or low velocity antegrade flow was documented during diastole, leading to a greater peak velocity during systole (fig 2B).
Comparing the two surgical techniques, the inspiratory/expiratory ratio of antegrade peak flow velocities was significantly higher in patients after total cavopulmonary anastomosis within the right atrium/intra-atrial tunnel (p = 0.007), hepatic vein (p = 0.001), and to a lesser degree the inferior caval vein (p = 0.03).
Discussion
In recent years definitive palliation for patients with functionally univentricular hearts has changed from atriopulmonary anastomosis to total cavopulmonary anastomosis. Postoperative morbidity has mainly been focused on late arrhythmias, risk of right atrial thrombi, and the development of protein losing enteropathy. In addition there is concern about the effect of chronically elevated right atrial and systemic venous pressure on hepatic and renal function. Despite the use of various modifications of the Fontan procedure and recent clinical studies investigating postoperative haemodynamic data with regard to postoperative morbidity,15 ,16 simultaneous assessment of flow patterns, respiration, and pressure events have not been performed.
Clinical and experimental studies examining the importance of atrial contraction in patients after a modified Fontan operation produced conflicting results and focused on pulmonary circulation: in patients with an atriopulmonary anastomosis, pulmonary arterial forward flow was augmented at the time of atrial contraction, so that the atrial contribution to total flow was similar during inspiration and expiration.5 ,6 ,13 However, these studies lacked corresponding pressure measurements and the characteristics of the pressure curve. With introduction of the total cavopulmonary anastomosis, the debate focused on the problem of whether an operation designed to provide an arterial pulse into either a Glenn or a Fontan pulmonary circulation was physiologically preferable to non-pulsatile flow after total cavopulmonary anastomosis, and whether it would prevent the development of arteriovenous malformations.1 ,2 Another haemodynamic aspect was considered in an experimental animal study: it was confirmed that there was a significant correlation between a pulsatile pulmonary blood flow and a lower pulmonary vascular resistance, in contrast to the situation with a non-pulsatile flow after a superior vena cava to right pulmonary artery anastomosis.17 ,18
The clinical importance—or even potentially adverse effects—of pulsatility of the systemic venous and hepatic venous flow for organ function and of the respiratory variability of the flow patterns have not been mentioned or investigated in recent reports on the sequelae and late postoperative morbidity after the Fontan operation.
Pressure tracings after total cavopulmonary anastomosis showed minimal pulsation or only oscillation, with identical pressure measurements in the caval veins and the intra-atrial tunnel, while neither significant respiratory variability nor any relation to the cardiac cycle was observed in our study. A more flattened right atrial pressure curve was documented in some patients with protein losing enteropathy, suggesting that congestion in the superior caval vein and thoracic duct might be a contributing pathophysiological factor.15 Examination of the Doppler flow profile in the superior and inferior caval vein after total cavopulmonary anastomosis showed the dependence of antegrade flow on changes in intrathoracic pressure. However, there is still transmission of the arterial pulse, indicating that blood is pulled through the lungs in addition, as observed in patients after a total cavopulmonary shunt during respiratory arrest.13 Potential long term consequences of the predominantly respiration dependent and less pulsatile systemic venous flow for the thoracic duct drainage, for the risk of development of protein losing enteropathy, or for the development of systemic venous to pulmonary venous collaterals might be expected and will be the subject of further experimental investigation.
After atriopulmonary anastomosis, pressure tracings with tall “a” waves had previously been documented for the right atrium and pulmonary artery. These findings were thought to be almost entirely a function of atrial contraction and relaxation.1 ,17 ,18 However, the pulsatile chamber might transmit the systolic work in both directions: forward to the pulmonary arteries and backward into the distended systemic veins, with raised internal pressure and diminished venous vascular capacitance.19 These conditions are supposed to cause alterations in the function of organs drained by the portal system.15 Cavopulmonary anastomosis excluding the portal venous return was therefore recommended for patients with protein losing enteropathy secondary to atriopulmonary anastomosis.20 However, this procedure carries the risk of the development of an intrahepatic collateral circulation with consecutive progressive cyanosis.20
In patients who had had an atriopulmonary anastomosis a biphasic antegrade systemic venous flow pattern with minimal respiratory variation was obtained. The first phase during early systemic ventricular diastole and atrial contraction was followed by a second phase of antegrade flow; this was caused by right atrial relaxation and left atrial filling from the pulmonary venous bed and suction of the dominant ventricle.19 Despite this, the atriopulmonary anastomosis was thought to be of poor hydrodynamic design: flow disturbances at the inlet and outlet of the atrial cavity and at the level of the atriopulmonary anastomosis, exaggerated by pulsation, were supposed to cause energy losses.1
Doppler waveforms in the hepatic veins are inversely related to right atrial pressure events and to the result of variations in central venous pressure during the cardiac cycle.21 After a total cavopulmonary anastomosis, hepatic venous drainage was predominantly maintained only during inspiration. This extreme dependence on respiration in the presence of a constantly raised systemic venous pressure might affect hepatic perfusion and alter liver function. On the other hand, it has been proposed that the reduced pulsatility of the hepatic portal venous flow after total cavopulmonary anastomosis, compared with that after atriopulmonary anastomosis, might be protective of liver function.11
CONCLUSIONS
While pressure tracings after the total cavopulmonary anastomosis revealed a flat and nearly constant systemic venous profile, without any relation to the cardiac cycle, venous Doppler flow patterns showed a marked respiratory dependence of systemic venous and hepatic venous return. The hydrodynamic advantage of total cavopulmonary anastomosis might be neutralised by the pronounced respiratory dependence of the venous return flow. The potential effects on postoperative morbidity, including liver dysfunction and protein losing enteropathy, need to be determined in comparison with the situation after atriopulmonary anastomosis, where there is preserved right atrial contraction and pulsatility reflecting the cardiac cycle.