Article Text

Abstract
OBJECTIVE To determine the frequency of the use of primary angioplasty in patients with acute myocardial infarction and the factors influencing its indications in hospitals with the facilities to perform this treatment.
DESIGN Data from the maximal individual therapy in acute myocardial infarction (MITRA) trial were analysed, concerning the effects of the decisions of individual hospitals, the time of admission of patients, and the effects of patient characteristics on the selection of reperfusion treatment.
PATIENTS Between June 1994 and January 1997 eight hospitals treated 1532 patients with acute myocardial infarction. 418 (27.3%) were treated conservatively, 641 (41.8%) were treated using intravenous thrombolysis, 387 (25.3%) were treated using primary angioplasty, and 86 (5.6%) received a combination of thrombolysis and angioplasty.
RESULTS The proportion of patients treated with primary angioplasty varied from 1.8% to 57.7% among the eight hospitals. The use of primary angioplasty during non-office hours also showed wide variation, ranging from 20% to 54% between centres. The use of thrombolysis was comparatively evenly distributed during the non-office hours, ranging from 50–69%. Four hospitals with a primary angioplasty use rate > 30% showed no difference in the proportion of patients with contraindications for thrombolysis, high risk patients, or a combination of both, when compared with four hospitals with a lower rate of primary angioplasty use (98/322 (30.4%)v 19/65 (29.2%), respectively, p = 0.847).
CONCLUSIONS In hospitals with the facilities for performing primary angioplasty the most important factors influencing its use were the discretion of the individual hospital and the time of patient admission. Characteristics of patients did not influence the choice of reperfusion treatment
- acute myocardial infarction
- primary angioplasty
- reperfusion treatment
Statistics from Altmetric.com
Primary angioplasty has been proven to be an effective treatment for patients with acute myocardial infarction presenting with ST segment elevation.1 It may be considered as an alternative to thrombolytic treatment for these patients.2-6 For patients with a high risk of hospital death, primary angioplasty may even be superior to thrombolysis.3 For patients with contraindications to thrombolysis primary angioplasty is the method of choice to achieve reperfusion7-9 and to reduce hospital mortality, as opposed to conservative treatment.10
However, primary angioplasty can only be performed in hospitals with a cardiac catheterisation laboratory, by specialised physicians trained in angioplasty. Less than 20% of the hospitals in the US11 and less than 10% in the UK12 are able to perform primary angioplasty. Not even all of these can do so on an emergency basis 24 hours a day, seven days a week. Also, the promising results from highly specialised centres2-4 were attenuated when primary angioplasty was performed on a broader basis.13-17 This indicates a special learning curve for primary angioplasty, even for physicians with experience in conventional angioplasty,18 ,19 as well as the need for an institutional effort to optimise clinical logistics.20
Despite our knowledge regarding the results of primary angioplasty, little is known about daily practice concerning the use of primary angioplasty and about the factors influencing the indications for primary angioplasty in hospitals with the facilities to perform it.
We therefore used data from the southwest German maximal individual therapy in acute myocardial infarction (MITRA) trial21 to analyse the effects of the decision of the individual hospital, the time of admission of the patients to the hospital, and the effects of patient characteristics on the choice of reperfusion treatment.
Methods
MITRA is a German prospective multicentre observational study of the current treatment of acute myocardial infarction.21Fifty four hospitals in the southwest of Germany participated in the study, including university hospitals, tertiary care centres, and smaller hospitals. All patients presenting within the first 96 hours of the onset of pain were registered prospectively, as soon as the diagnosis of acute myocardial infarction had been made.
Acute myocardial infarction was diagnosed in the presence of at least two of the three following signs: persistent angina pectoris for ⩾ 20 minutes; ST segment elevation of ⩾ 1 mm in at least two standard leads or ⩾ 2 mm in at least two contiguous precordial leads; or increased enzyme concentrations (creatine kinase and its MB isoenzyme, aspartate aminotransferase, lactic dehydrogenase) to twice the normal upper range. Acute myocardial infarction was also diagnosed by the presence of left bundle branch block and persistent angina pectoris for ⩾ 20 minutes. Final diagnosis of acute myocardial infarction, as well as the decision regarding the type of treatment, was left to the discretion of the treating physician and not to the study protocol.
The following protocols for intravenous thrombolysis were suggested: intravenous application of 1.5 million units of streptokinase over one hour or tissue plasminogen activator at a dose of 100 mg over one and a half hours intravenously. Angioplasty was performed according to the standard protocol of each centre.
DEFINITIONS
Postinfarction angina was diagnosed in the presence of new angina pectoris within two weeks after myocardial infarction. Reinfarction was defined as recurrent chest pain lasting more than 20 minutes with new ST segment elevation and either emergency angiographic confirmation of an occluded vessel or recurrent increases in cardiac enzymes. Minor stroke was defined as a transient cerebral ischaemia, and major stroke as a persistent cerebral ischaemia. A combined clinical end point was defined by the occurrence of death, reinfarction, postinfarction angina, stroke, or heart failure of New York Heart Association class III or above.
For this analysis we selected the patients who arrived at the hospital within 12 hours of the onset of symptoms or those for whom prehospital delay times were missing. Only eight of 54 participating hospitals had the facilities necessary to perform primary angioplasty, as defined by the presence of a catheterisation laboratory and the performance of regular angioplasties.
We analysed three possible factors influencing the selection of a reperfusion treatment.
- (1)
- The decision of the individual hospital to perform primary angioplasty.
- (2)
- The time of admission to the hospital. We looked for differences in treatment during office hours (time of admission of patients between 08:00 and 17:00 from Monday to Friday) and non-office hours (17:00 until 08:00 from Monday to Friday, as well as the whole weekend).
- (3)
- Characteristics of the patients. The following two groups of patients, who would probably benefit most from primary angioplasty, were defined as: (a) a high risk group—heart rate ⩾ 100 beats/min on admission, cardiogenic shock, the presence of left bundle branch block, resuscitation, or systolic blood pressure < 100 mm Hg; and (b) patients with at least one of the following contraindications for thrombolytic treatment—active bleeding, recent (< 3 months) cerebral infarction, recent (< 14 days) surgery or trauma, or a history of ulcer disease.
STATISTICS
Data concerning the prehospital period and the early intrahospital period (first 48 hours) were collected within the first two to three days in the intensive care unit. Clinical events afterwards were registered on a separate record form on hospital discharge. Every participating centre had committed by written consent to include each patient with acute myocardial infarction during the study period. The patients gave informed consent for processing their anonymous data. All data sheets were sent to the central data processing centre (department of cardiology, Herzzentrum Ludwigshafen) for uniform monitoring and registration.
Absolute numbers and percentages were computed to describe the patient population. Categorical values were compared using χ2. All p values are two tailed; p < 0.05 was considered significant. The tests were performed using the SAS statistical package, version 6.12 (Cary, North Carolina).
Results
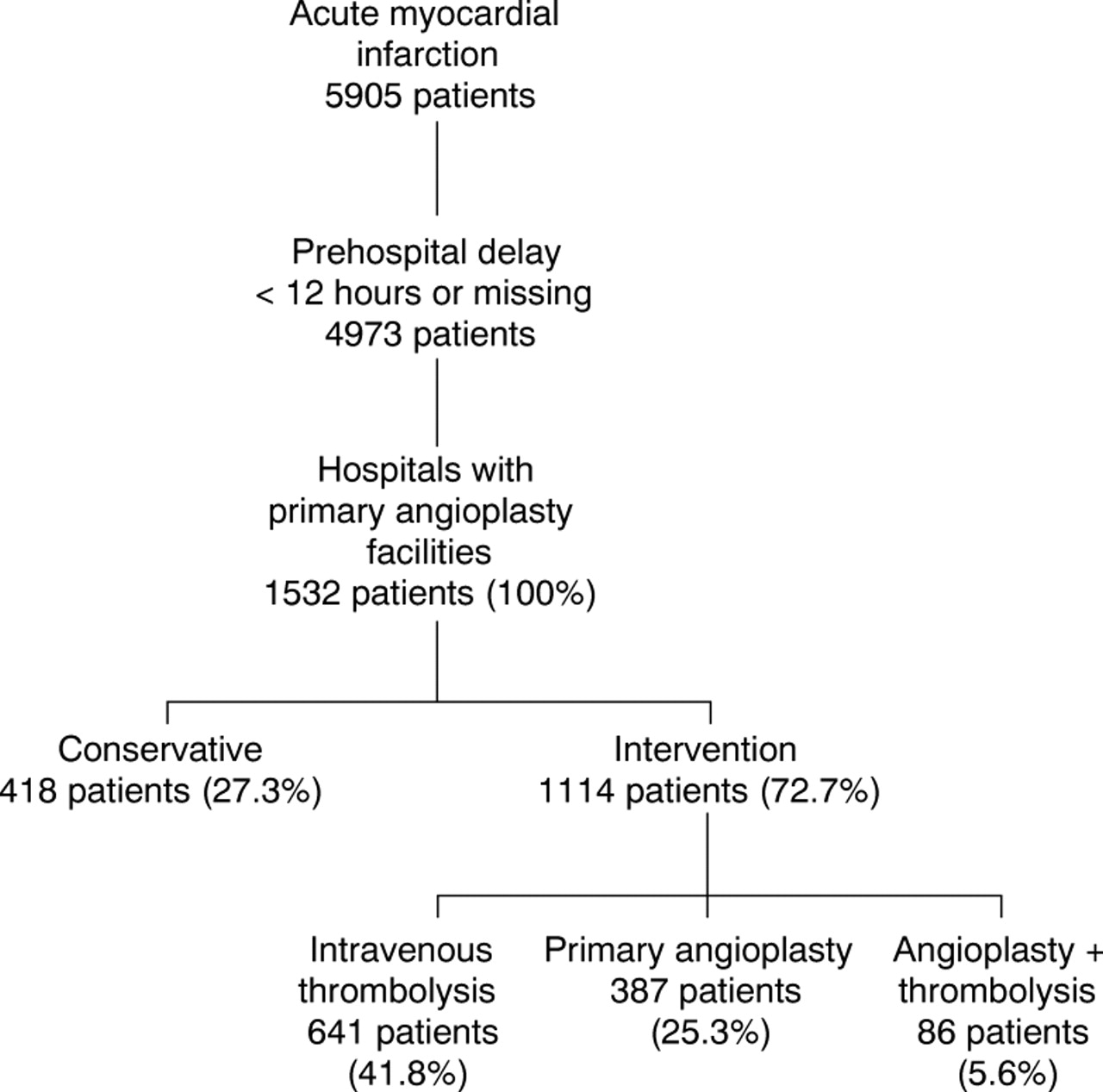
Between June 1994 and January 1997 5905 patients with acute myocardial infarction were registered (fig 1). Of those, 4973 patients had either a prehospital delay time < 12 hours or the time between the onset of symptoms until admission at the hospital was unknown. The eight hospitals with the facility to perform primary angioplasty treated 1532 (30.8%) of these patients. Of these 1532 patients, 418 (27.3%) were treated conservatively and 1114 (72.7%) received a reperfusion treatment: 641 patients (41.8%) were treated with intravenous thrombolysis, 387 patients (25.3%) underwent primary angioplasty, and 86 patients (5.6%) received a combination of angioplasty and thrombolysis. The prehospital delay was unknown in 122 of the 1532 patients (8%).

Selection of patients from the MITRA trial.
The clinical events occurring in each of the four therapeutic groups during the hospital stay are shown in table 1. Patients treated conservatively had the worst clinical outcome, whereas patients treated with primary angioplasty had the lowest complication rate. Patients treated with thrombolysis or the combination of angioplasty and thrombolysis had an intermediate complication rate.
Clinical events during hospitalisation according to the type of treatment administered
INFLUENCE OF HOSPITAL ON THE TYPE OF REPERFUSION TREATMENT
As shown in table 2, there were big differences regarding the selection of the various therapeutic options in the eight hospitals. The rate of conservative treatment ranged from 10.7–35.2%, and the use of primary angioplasty ranged from 1.8–57.7%.
Reperfusion treatments in different hospitals with the facility to perform primary angioplasty (sorted according to the case load of the hospitals)
INFLUENCE OF TIME OF ADMISSION
The influence of the time of admission on the choice of the reperfusion treatment is shown in fig 2; 697/1532 (45.5%) of patients were admitted to the hospitals during office hours and 835/1532 (54.5%) were admitted during non-office hours. In relation to all the patients treated with thrombolysis at each centre, the proportion of patients receiving thrombolysis during non-office hours was relatively equally distributed (range 50–69%). However, there were large differences among the hospitals in the use of primary angioplasty during non-office hours (range 20–54%).

Comparison of treatment with thrombolysis and treatment with primary angioplasty in different hospitals during non-office hours.
INFLUENCE OF PATIENT CHARACTERISTICS ON TYPE OF REPERFUSION
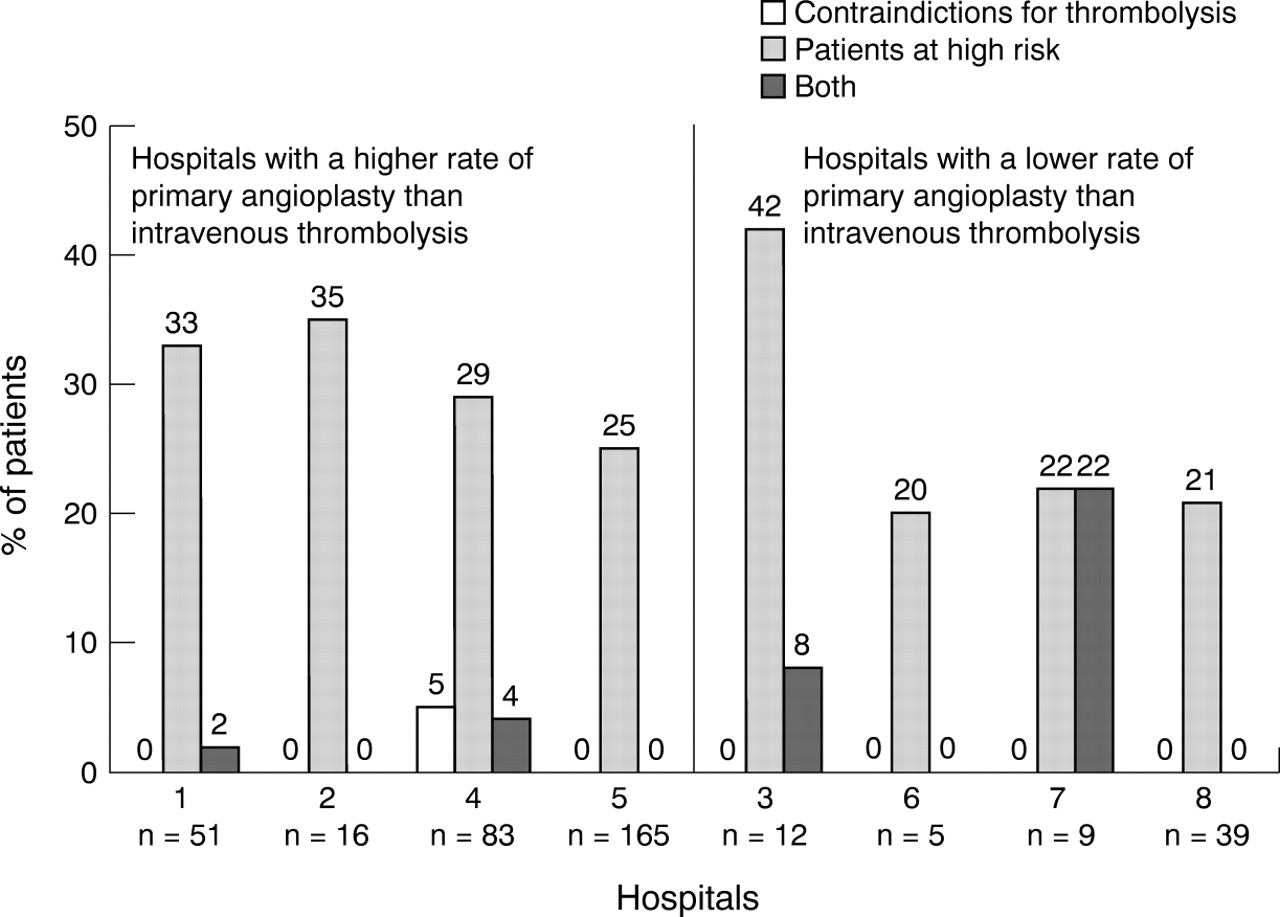
Hospital mortality in high risk patients was 168/527 (31.9%) compared to 72/1005 (7.2%) in patients without these risk factors (p = 0.001). Of 387 patients who were treated with primary angioplasty, 113 (29.2%) were high risk patients. Eleven patients (2.8%) had contraindications to thrombolysis, seven (1.8%) had either contraindications or were high risk, and 270 (71.8%) belonged to none of these groups. Figure 3 shows the proportion of patients belonging to these groups in each hospital. Although there are differences between the hospitals, these are difficult to judge because of the small number of patients in some hospitals. We therefore compared hospitals with a rate of primary angioplasty > 30% (hospitals 1, 2, 4, 5—group 1) to hospitals with a lower rate (hospitals 3, 6, 7, 8—group 2). There was no difference in the proportion of patients having contraindications to thrombolysis, high risk patients, or the combination of both, between the two groups (98/322 (30.4%) in group 1 v19/65 (29.2%) in group 2, p = 0.847).

Patients treated with primary angioplasty at different hospitals—frequencies of patients with contraindications for intravenous thrombolysis, high risk patients, or the combination of both.
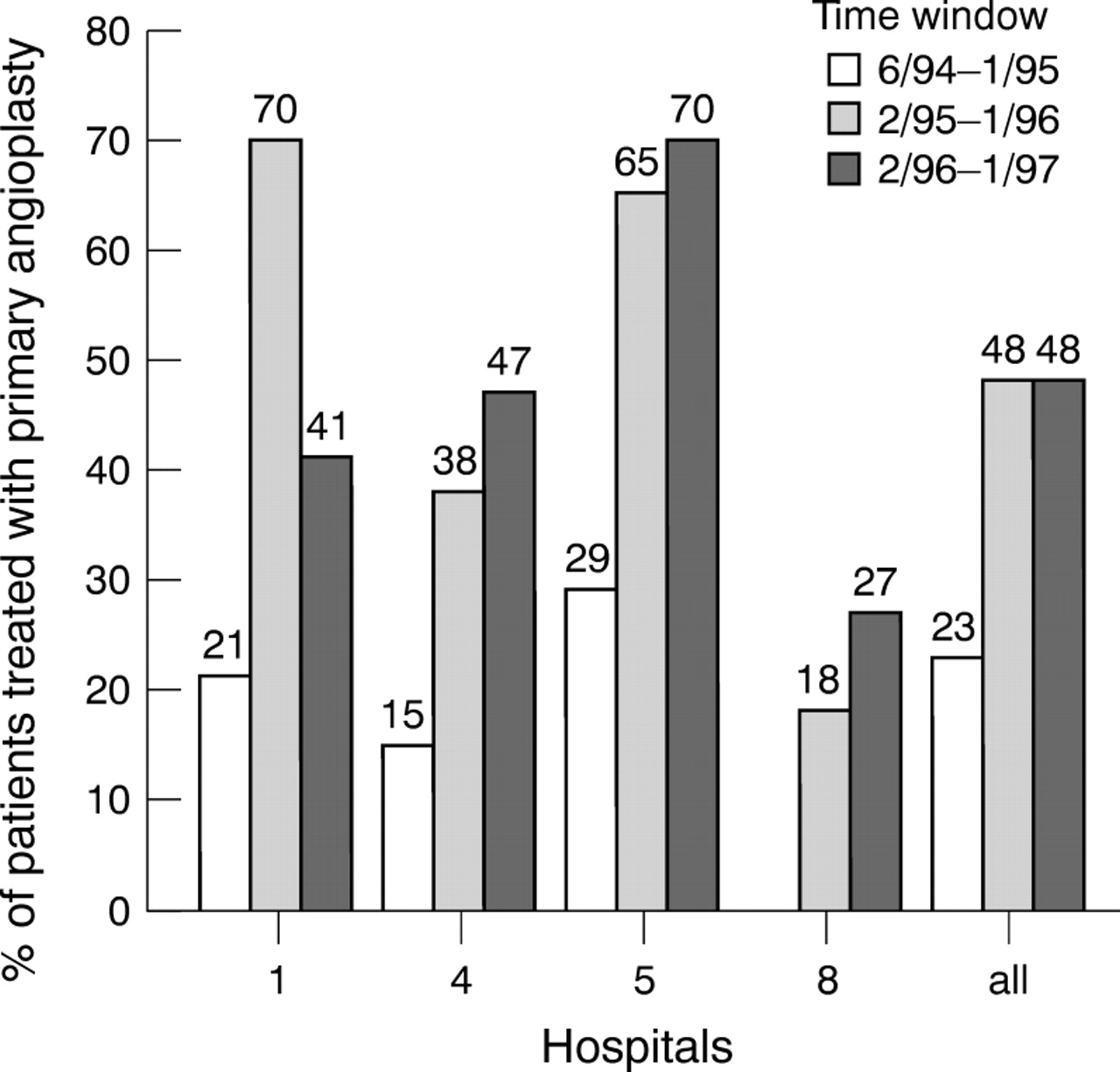
The rate of primary angioplasty use in patients with acute myocardial infarction during the study period is shown in fig 4 for hospitals 1, 4, 5, and 8. The other hospitals were not included in this figure because the number of cases was too low. In the hospitals analysed there was an overall increase in the use of primary angioplasty from 23% in 1994 to 48% in 1995 and 1996. In hospital 1 a reduction from 70% in 1995 to 41% in 1996 occurred. All other hospitals showed an increase in their primary angioplasty rates over the time of the study.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Development in the rate of primary angioplasty use in the treatment of patients with acute myocardial infarction in four different hospitals.
Discussion
At those hospitals with the facilities to perform primary angioplasty, intravenous thrombolysis was more frequently used (641/1114, 57.5%) than primary angioplasty (380/1107, 34.7%) for patients presenting with acute Q wave myocardial infarction. We observed a broad spectrum in the use of primary angioplasty, ranging from 1.8–57.7% in the eight participating hospitals. The most important factor influencing the decision to perform primary angioplasty was the discretion of the individual hospital. The next most important factor was the admission time of a patient with acute myocardial infarction. Patients admitted during non-office hours were less likely to be treated with primary angioplasty. Characteristics of patients did not influence the choice of reperfusion treatment. There was an overall increase in primary angioplasty from 23% in 1994 to 48% in 1995 and 1996. The decrease in primary angioplasty at hospital 1 in 1996 was caused by the loss of one catheterisation laboratory.
The overall event rates in our study were high when compared to randomised studies.2-4 However our study represents consecutive unselected patients with acute myocardial infarction, in which mortality is usually higher. The distribution of the event rates in the four therapeutic groups were also as we had expected. Patients treated conservatively showed the worst clinical outcome, whereas patients treated with primary angioplasty had the lowest complication rate. Patients treated with thrombolysis or a combination of angioplasty and thrombolysis had an intermediate complication rate. These differences were most probably the result of a mixture of patient selection, different adjunctive medical treatment in the groups, and different kinds of reperfusion treatment. However, the aim of the present study was not to analyse these differences in detail.
The observed range of 1.8–57.7% for the use of primary angioplasty in the eight hospitals shows that the decision of the individual hospital was the most important factor for the choice of this treatment. This rate was not dependent on the case load of acute myocardial infarctions or the case load of elective procedures in the hospitals. All four hospitals with a primary angioplasty rate < 30% mainly performed primary angioplasty during regular working hours as they had not installed a 24 hour, seven days a week service. The studies by Garot and colleagues22 and McNamara and colleagues23 showed that primary angioplasty during the “off” hours can be performed safely and show comparable results to those performed during “on” hours. However, the implementation of such a “round the clock” service is expensive and requires many experienced personnel. Interviews of the physicians responsible showed that the single most important reason for not establishing such a service was that they were not convinced of the superiority of primary angioplasty over intravenous thrombolysis for patients with acute myocardial infarction. Economic reasons or the lack of experienced personnel played only a minor role.
Even at the four hospitals with a high rate of primary angioplasty use, there is still a tendency towards less use of primary angioplasty during the non-office hours. This is mainly because of the changing use of primary angioplasty over time. The steady increase in the use of primary angioplasty in hospitals 4 and 5 was associated with the introduction of standby catheterisation and angioplasty facilities.
All four hospitals with a primary angioplasty rate < 30% showed a rate of conservative treatment > 30%. In the four hospitals with a rate of primary angioplasty > 30% the proportion of conservative treatment ranged from 10.7–29.4%. The decision to perform primary angioplasty as the method of choice seems to be associated with the desire to treat more patients with any reperfusion treatment. The reason for this association might be that more patients are eligible for primary angioplasty than for thrombolysis—for example, patients with contraindications for thrombolysis. However, accepting only strong contraindications, as advised by scientific committees,24-26 only about 6% of patients presenting with acute myocardial infarction are not eligible for intravenous thrombolysis.
To achieve reperfusion is of particular importance in patients with acute myocardial infarction and contraindications for thrombolytic treatment. In these patients primary angioplasty is feasible7-9 and life saving.10 A previous analysis of the MITRA data showed an independently lower in-hospital mortality for patients with contraindications for thrombolysis treated with primary angioplasty as opposed to patients treated conservatively (odds ratio 0.46, p = 0.023).10 Primary angioplasty may also be superior to thrombolysis in high risk patients, as shown by the primary angioplasty in myocardial infarction (PAMI) group3and perhaps also in patients presenting with cardiogenic shock.16 ,27 ,28 However, hospitals with a low overall rate of primary angioplasty did not use primary angioplasty mainly in high risk patients or patients with contraindications for thrombolysis. The proportion of such patients treated with primary angioplasty was virtually identical in these hospitals (19/65, 29.2%) compared to hospitals with a high rate of primary angioplasty (98/322, 30.4%).
A study by Juliard and colleagues29 showed that up to 98% of all unselected patients with acute myocardial infarction can be treated with a reperfusion treatment, in contrast to 73% of patients observed in our study. However, in an unselected population with acute myocardial infarction at 128 hospitals, Rustige and colleagues reported the use of reperfusion treatment in only 53% of patients.30 The recently published data from the national registry of myocardial infarction 2 showed that 24% of patients eligible for thrombolysis received no reperfusion treatment.31 There were great differences among the eight hospitals participating in our study, with a range of reperfusion treatment between 65–89%. This indicates that even in clinical practice in hospitals with the facilities necessary to perform primary angioplasty, up to 90% of patients with acute myocardial infarction can be treated with some kind of reperfusion. There are always patients—for example, with terminal cancer or other limiting diseases—where no reperfusion treatment will be initiated. Therefore a reperfusion rate of about 90% of patients with acute myocardial infarction seems to be a realistic goal in such hospitals.
As already known from regular coronary angioplasty,32 ,33there is also accumulating evidence showing better results for primary angioplasty in high volume centres compared with low volume centres.18 ,19 Continuous quality control can also improve outcome of primary angioplasty as shown by Caputo and colleagues.20 Restricted financial resources in most countries means that an increase of centres with the facilities to perform angioplasties and primary angioplasties seems to be unlikely.
With the goal of reperfusing up to 90% of patients with acute myocardial infarction and a pre-hospital delay ⩽ 12 hours after onset of symptoms, we suggest the following practice to hospitals with the facilities to perform primary angioplasty.
Choosing primary angioplasty as the treatment of first choice for patients with acute myocardial infarction would enable doctors to become more experienced with the procedure, and thus achieve better results.
Establishing a 24 hour, seven days a week service would enable hospitals to increase the number of patients they treat, especially patients contraindicated for thrombolysis.
Introducing a round the clock service with experienced personnel means the service could be offered to the surrounding hospitals where the facilities are lacking to perform primary angioplasty. Patients with contraindications to thrombolysis, with ineffective thrombolysis, or high risk patients could be transferred to these centres to undergo primary angioplasty within an acceptable time limit.
With such efforts, the goal of treating up to 90% of patients would no longer be restricted to some enthusiastic hospitals but would be achievable for whole regions.
STUDY LIMITATIONS
MITRA is a prospective observational study involving hospitals in the southwest of Germany. Therefore the described practice at hospitals with the facilities to perform primary angioplasty may be different in other countries. We did not collect information on the number of vessels dilated and the rate of technical success (residual stenosis, TIMI grade 3 flow) of the angioplasty procedures.
Acknowledgments
We would like to thank Heinz Hochadel for his assistance with the statistical analysis, and Stefan Wagner and Sinéad Trainor for their helpful comments on the manuscript. This study was supported in part by Zeneca, Ministerium für Gesundheit, Arbeit, Soziales des Landes Rheinland-Pfalz, Landesversicherungsanstalt Rheinland-Pfalz, Betriebskrankenkassen Rheinland-Pfalz. The people and institutions who participated in the MITRA study are listed elsewhere.21