Article Text

Abstract
A 78 year old man presented with diarrhoea, anorexia, and progressive lower limb oedema. He was in atrial fibrillation and had a right pleural effusion and ascites. Ultrasound of the abdomen and 24 hour urinary hydroxyindoleacetic acid output indicated metastatic carcinoid syndrome. Cardiac catheterisation revealed pericardial constriction, and pericardial exploration showed a greatly thickened pericardium with no evidence of tumour invasion. The patient died within 24 hours of surgery. Necropsy findings were consistent with a diagnosis of constrictive pericarditis secondary to metastatic carcinoid syndrome.
- carcinoid syndrome
- constrictive pericarditis
- liver metastases
Statistics from Altmetric.com
Carcinoid tumours are neuroendocrine tumours which are usually found in the small intestine or lung. Carcinoid syndrome may cause hypotension, flushing, diarrhoea, and oedema due to the release of serotonin, kinins, and other hormones, and involvement of the heart may cause characteristic tricuspid and pulmonary valve abnormalities; the myocardium and pericardium are rarely affected. We report a new aspect of this complex disease—namely, constrictive pericarditis secondary to a terminal ileal carcinoid tumour, presenting as rapidly progressive oedema.
Case report
A 78 year old man presented with a four week history of watery diarrhoea. He also complained of anorexia, hoarseness, and a one week history of progressive leg oedema. He had been diagnosed with thyrotoxicosis six weeks before, and had had pulmonary tuberculosis when he was 4 years old. On examination he was found to have noticeable bilateral pitting oedema of both lower limbs, which extended to the level of the umbilicus on the anterior abdominal wall. He was in atrial fibrillation with a controlled ventricular response and his venous pressure was raised; he had clinical evidence of ascites and a right pleural effusion.
His liver function tests were abnormal and thyroid function tests were consistent with the diagnosis of thyrotoxicosis (table 1). Urinary outputs of 5-hydroxyindoleacetic acid (5-HIAA) and 5-hydroxytryptamine (5-HT) were raised, and fasting gastrointestinal hormone results were strongly suggestive of a metastatic neuroendocrine tumour originating from a primary mid-gut origin (table2).
Results of liver function, thyroid function and urinary samples
Results of fasting gastrointestinal hormones
Ultrasound of the abdomen showed hepatic lesions in both lobes consistent with metastases. The inferior vena cava was distended and non-oscillatory, and percutaneous ultrasound guided liver biopsy provided tissue which was indicative of a metastatic neuroendocrine tumour, possibly of pancreatic or small intestinal origin. This tissue stained positively for neurone specific enolase and chromogranin, and negative stains were obtained for α fetoprotein; small bowel series failed to show an intestinal lesion.
Computed tomography of the abdomen and chest confirmed the presence of a metastasis in the right lobe of the liver. The pericardium was thickened but there was no evidence of pericardial calcification, and transthoracic and transoesophageal echocardiography showed high filling pressures across the mitral and tricuspid valves. There was no evidence of endocardial thickening or fibrosis. Cardiac catheterisation suggested constrictive pericarditis with equalisation of diastolic pressures: mean right atrial pressure was 17 mm Hg, right ventricular end diastolic pressure was 20 mm Hg, and mean capillary wedge pressure was 19 mm Hg. There was also a classic square root sign from the right ventricular pressure tracing.
The patient was diagnosed with metastatic carcinoid tumour and treated with octreotide 50 μg subcutaneously twice daily. His condition deteriorated and pericardial exploration was performed after high dose octreotide treatment to avoid a carcinoid crisis. The pericardium was very thick and two longitudinal incisions were made to free the anterior border of the heart from the constriction; the left and right sides of the heart were also mobilised. Three litres of straw coloured fluid were drained from the pleural cavities and milky ascites was drained from the abdomen. The patient tolerated the procedure well but 11 hours after the operation he became hypotensive, despite adequate filling pressures. Initially, he responded to infusions of phenylephrine, methylprednisolone, methoxamine, dopamine, and octreotide, but subsequently had a cardiac arrest from which he could not be resuscitated.
The necropsy revealed a 1.5 cm diameter annular tumour in the terminal ileum arising 25 cm from the ileocaecal valve; a solitary metastasis was found in the right lobe of the liver. The heart was enlarged (445 g) and there was biventricular cavity dilatation, but no valvar stenosis. The pericardium was greatly thickened and constrictive and all the body cavities contained large effusions consistent with pericardial constriction.
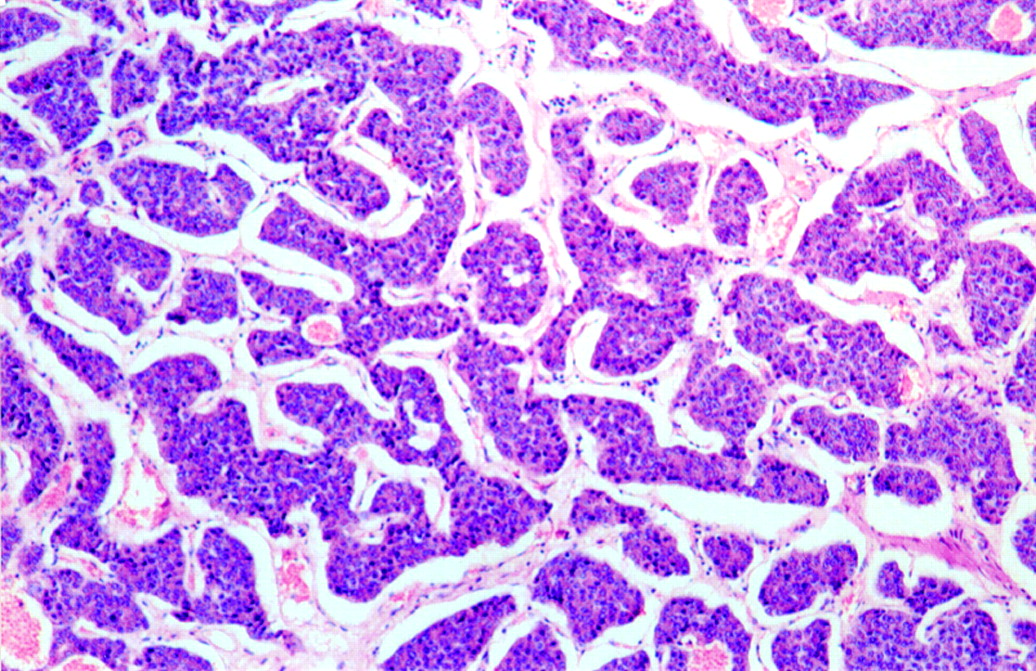
Histology revealed a tumour originating in the small intestinal mucosa and extending through the bowel wall into the mesenteric adipose tissue, and evidence of vascular invasion was found. The tumour cells were arranged in cords and islands, forming an insular pattern of growth (fig 1). Occasional mitoses were present and there was minimal cytological pleomorphism. The histology of the metastatic liver deposit was similar. The tumour cells stained positively after incubation with antibodies against neuroendocrine cell markers, including chromogranin and neurone specific enolase. Tumour extract studies showed raised pancreastatin (593 ng/g), substance P (1325 ng/g), and neurokinin A (1616 ng/g) for both the ileal primary and the liver metastases, which was consistent with a mid-gut carcinoid.

Low power view of the tumour nests in the lamina propria (original magnification ×100).
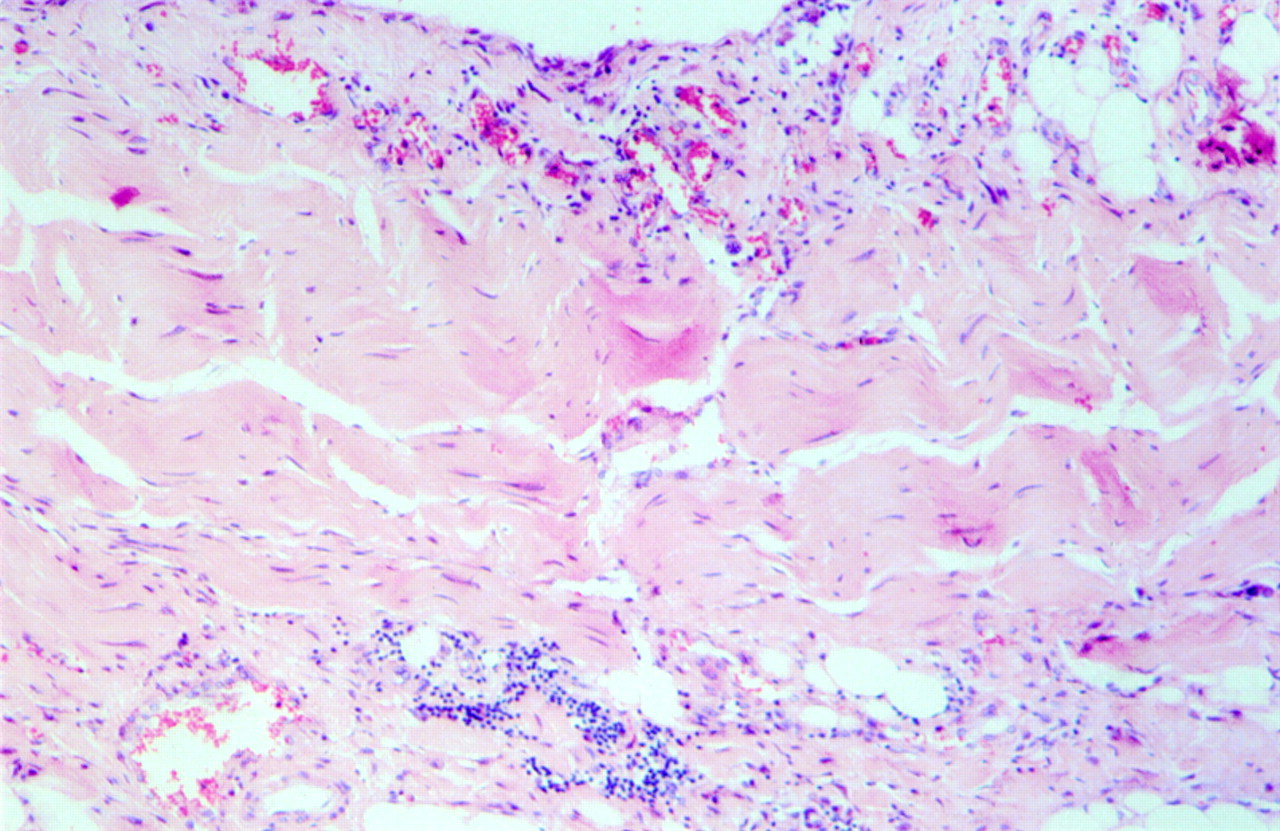
The pericardial specimens obtained at operation and at necropsy showed similar features with noticeable hyaline fibrosis (fig 2) and surrounding chronic inflammation with a predominance of lymphocytes and plasma cells. No granulomas were identified and the Ziehl Neelson stains for acid and alcohol fast bacilli were negative. Sections from both ventricles showed myocardial fibre hypertrophy and mild interstitial fibrosis.

{kind=link}
{kind=link}
Pericardium showing hyaline fibrosis and chronic inflammation.
Discussion
Carcinoid syndrome is characterised by flushing, diarrhoea, oedema, and hypotension due to the release of serotonin, kinins, and other hormones. Tumours may develop in various sites including the bronchus, mid-gut, or ovary. Metastases commonly affect the liver and, rarely, the heart.1 Carcinoid heart disease is one of the most intriguing aspects of this syndrome. Although flushing and diarrhoea usually predate significant valvar dysfunction, discovery of tricuspid regurgitation or stenosis sometimes provide the first clue to the presence of the disease. The most frequent cardiac complications of carcinoid syndrome are tricuspid and pulmonary valve abnormalities, probably due to long term exposure of the endocardium on the right side of the heart to serotonin.2 Involvement of the mitral valve is less frequent and is often associated with a right to left shunt.3 Other uncommon cardiac complications may include granulomatous myocarditis, endocardial fibrosis, restrictive cardiomyopathy, and congestive or right heart failure.4-6
Involvement of the pericardium with carcinoid tumours has been reported. Rich and colleagues and Gelfand et al both presented case reports of direct pericardial invasion by tumour, which was confirmed histologically through pericardial exploration, after successful resection of the primary lesion.7 ,8 Pericarditis and pericardial effusions have been reported in the absence of tumour invasion3 ,6; a small pericardial effusion was present in 14% of a cohort of 74 patients with carcinoid heart disease, assessed by echocardiography.3 However, this is the first report of constrictive pericarditis associated with carcinoid syndrome, without evidence of tumour invasion.
This case also illustrates the hazards of general anaesthesia in patients with carcinoid syndrome, as perioperative release of hormones can lead to severe circulatory and respiratory disturbances.9 The use of invasive haemodynamic monitoring and the avoidance of drugs that can exacerbate the syndrome, is beneficial.10 Octreotide, both prophylactically and acutely, is the best medical treatment available. Although cardiac surgery carries a high perioperative mortality rate in patients with carcinoid syndrome, noticeable symptomatic improvement occurs in survivors11; surgical intervention should therefore be considered when cardiac symptoms become severe. Early deaths may be due to postoperative bleeding or right heart failure.11Adrenaline (epinephrine) is said to be contraindicated in carcinoid syndrome, but could be considered when hypotension results from myocardial depression rather than carcinoid crisis.12
Carcinoid tumours are rare and usually associated with a good prognosis. This case provides the first report of constrictive pericarditis secondary to a carcinoid tumour, which resulted in the initial presentation of the disease. Surgery in such patients can be hazardous and the patient should be treated with octreotide infusions in order to prevent the onset of carcinoid crisis in the perioperative period.
Acknowledgments
We acknowledge the expert opinion of Professor K Buchanan and Dr NSP Campbell and their help in preparing the manuscript, and to thank Dr JSA Collins, the consultant in charge, for permission to submit this case report.
References
eHEART: www.heartjnl.com
The following electronic only articles are published in conjunction with this issue ofHeart. Unusual congenital coronary anomaly and myocardial ischaemia D A Pascual, F Soria, M Valdes Angiography was used to diagnose a rare congenital coronary anomaly with myocardial ischaemia in a woman with typical angina. All three coronary arteries arose from a solitary coronary ostium in the right aortic sinus; the left anterior descending coronary artery followed a septal course, the circumflex coronary artery ran behind the ascending aorta, and the right coronary artery followed a normal course. No significant coronary lumen narrowing was found. Transoesophageal echocardiography confirmed the anomalous origin and course of the aberrant coronary arteries. An exercise test reproduced angina, and ECG changes and myocardial perfusion study showed an anterior reversible defect. In contrast to previous reports, myocardial ischaemia was associated with the septal (intramuscular) course of the left anterior descending coronary artery; there was no other significant coronary artery disease. (Heart1999;82:e7)www.heartjnl.com/cgi/content/full/82/5/e7 Nicorandil abolished repolarisation alternans in a patient with idiopathic long QT syndrome Y Fujimoto, H Morita, K K Fukushima, T Ohe A 23 year old woman with idiopathic long QT syndrome had repeated syncopal attacks associated with torsades de pointes. T wave alternans (TWA) was recorded and the QT interval was abnormally prolonged during treadmill exercise test. Monophasic action potential (MAP) alternans also appeared after an abrupt shortening of the cycle length in electrophysiological study. After intravenous administration of nicorandil 6 mg, both TWA and MAP alternans disappeared. (Heart1999;82:e8)www.heartjnl.com/cgi/content/full/82/5/e8