Article Text

Abstract
OBJECTIVE To study short and long term results after surgical closure of isolated ventricular septal defects (VSDs) from 1976 to 1996, especially in relation to changes in preoperative evaluation during this period.
DESIGN Retrospective study.
SETTING Tertiary referral centre for paediatric cardiac care.
PATIENTS All children under 18 years of age who had corrective surgery for VSD between 1976 and 1996.
MAIN OUTCOME MEASURES Preoperative evaluation, indications for surgery, diagnostic errors, and early and late results.
RESULTS A significant decrease in the use of invasive preoperative studies in favour of non-invasive methods was found; from 1976 to 1990, a total of 109/110 patients had preoperative invasive study as compared to 43/167 from 1991 to 1996 (p < 0.001). Pulmonary hypertension in small children, without detailed information on Qp:Qs ratio, as well as small or modest shunts without pulmonary hypertension, were more frequent indications for surgery in recent years. Early mortality after surgery occurred in 10 patients, with a significantly lower mortality rate found between 1991 and 1996 than between 1976 and 1990 (0.6% v 8.2%, p < 0.001). Children with large VSDs experienced perioperative complications significantly less often between 1991 and 1996 than between 1976 and 1990 (16/105 v 28/96, p < 0.05). Diagnostic errors showed a tendency to decrease between the two time periods. No late deaths occurred.
CONCLUSIONS Significant reductions in early mortality, perioperative complications, and diagnostic mistakes were seen during the study period, even though less invasive diagnostic procedures were being performed.
- ventricular septal defects
- paediatric surgery
- diagnostic measures
- congenital heart defects
Statistics from Altmetric.com
Ventricular septal defect (VSD) is the most common congenital heart defect, and surgical closure of VSDs is one of the most common open heart procedures performed in paediatric cardiac surgery, even though it still carries both mortality and morbidity risks.1-3Significant changes have occurred in the management of patients with VSD, such as early correction of patients with a large VSD with pulmonary hypertension, and in many institutions broader indications for VSD closure in patients with moderate shunts are used.4 There has also been a profound change in the preoperative evaluation of patients with VSD in favour of using mainly non-invasive methodology. While the use of non-invasive methods has simplified diagnosis in children with congenital heart defects,5 ,6 there is a risk of interpreting indications for surgical treatment too liberally, especially for defects with extremely low surgical mortality. In addition, there is little information in the literature on diagnostic errors inherent in the preoperative non-invasive evaluation of VSD. We report our experience on surgical closure of VSD from 1976 to 1996, especially in relation to the changes in diagnostic measures, preoperative evaluation, and indications for surgery during this period.
Methods
All children under 18 years of age who had corrective surgery for VSD in our institution from 1976 to 1996 were studied retrospectively. Patients with complex congenital heart defects (including coarctation of the aorta) in addition to VSD were excluded, but children with VSD and a persistent ductus arteriosus (PDA), atrial septal defect, systemic vein anomalies, tissue tags in the left ventricular outflow tract, dextrocardia, or regurgitation of the atrioventricular or semilunar valves were all included. Children who had had previous surgery for a PDA or banding of the pulmonary artery were also included. One child with a partially anomalous right pulmonary vein diagnosed postmortem was also included, as were all children with extracardiac malformations.
Relevant information was retrieved from the medical records. Basic information, such as sex, gestational age, birth weight, extracardiac malformations, and diseases, was collected, as well as details of diagnostic procedures, surgical methods, complications, and short and long term follow up. Pulmonary hypertension was recorded if one or more of the following criteria were met: systolic main pulmonary artery pressure exceeding 40 mm Hg as measured by catheterisation; a ratio of systolic main pulmonary artery pressure to systemic pressure (PAPs:SPs) of 0.5 or more; and a peak Doppler flow velocity across the VSD ⩽ 3 m/s. A Doppler regurgitation jet in the tricuspid valve with a maximal velocity of 5 m/s was found in one case and was regarded as pulmonary hypertension in the absence of stenosis in the right ventricular outflow tract. Borderline pulmonary hypertension was defined as: an invasively measured systolic main pulmonary artery pressure of 30 mm Hg to < 40 mm Hg; an invasively measured PAPs:SPs ratio ⩾ 0.3 to < 0.5; or a Doppler flow velocity across the VSD of > 3 m/s and < 4 m/s. We applied the χ2test, Student's t test, a life table calculation, and Spearman's rank correlation test. A p value of 0.05 was considered significant.
Results
BASIC INFORMATION
In total 277 patients were found, comprising 146 girls and 131 boys (53% and 47%, respectively). The median age at diagnosis was 2.3 months (0 days to 17 years, n = 231). The median age at surgery was 15.3 months (0.8 months to 17 years 11.9 months, n = 277). The median weight at surgery was 9.1 kg (2.6–69 kg, n = 220). The number of children operated upon each year varied from three to 12 between 1976 and 1990, which increased from 20 children in 1991 to 51 in 1996. Syndromes or extracardiac malformations were found in 81 children (29%), 48 of whom had Down's syndrome.
Pulmonary artery banding was performed before corrective surgery in 12 children, six of whom had simultaneous closure of a PDA, two had simultaneous division of an aberrant right subclavian artery, and one had a pulmonary biopsy. Another three patients had closure of a PDA before corrective surgery.
DIAGNOSTIC MEASURES
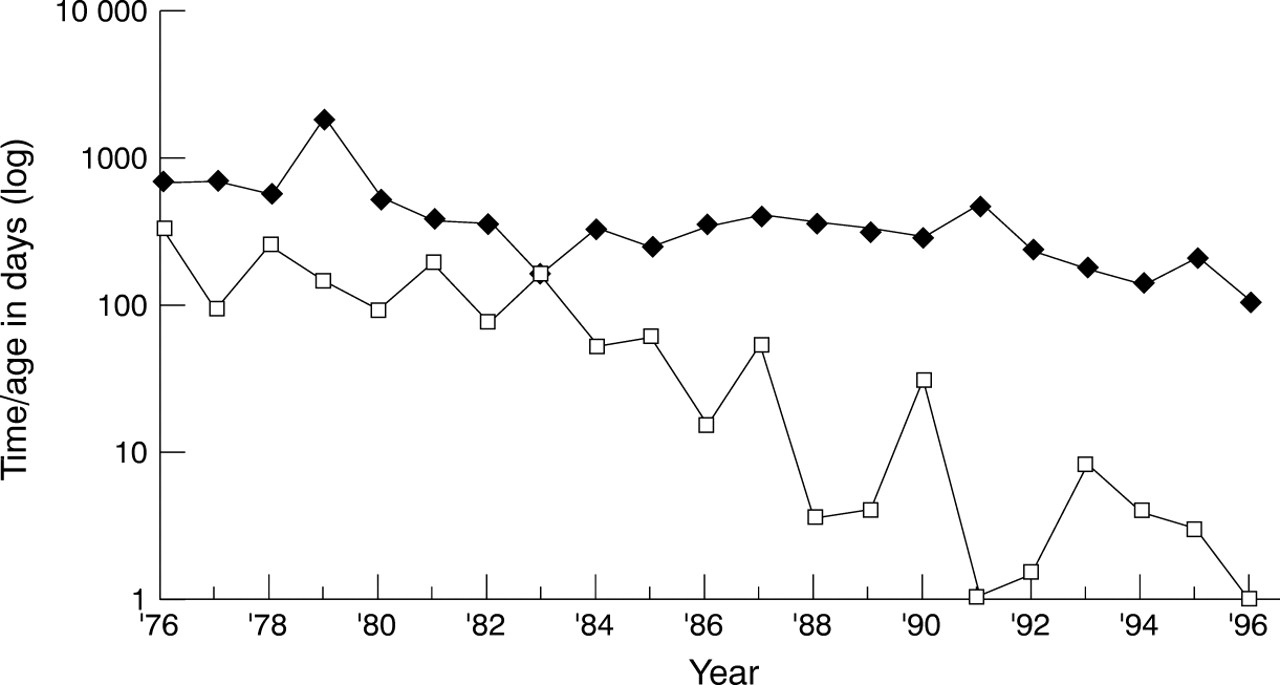
All children underwent chest radiography and electrocardiography before surgery. Invasive study, ultrasound, and shunt estimations by isotope study were used in various combinations to evaluate the VSD. Two dimensional echocardiography has been available in our institution since March 1983, colour Doppler since August 1990, and shunt estimation by isotope study since 1990 (except for one investigation in 1984). The increase in the number of non-invasive studies—that is, two dimensional echocardiography—since 1983 and the steady decrease in the number of preoperative invasive studies since 1992 is shown in fig 1. The median time from suspicion to confirmation of the diagnosis decreased significantly from 10.3 months to 1 day during the study period (p < 0.001), and the median age at surgery in children with pulmonary hypertension decreased from almost 2 years to slightly more than 3 months (p < 0.001) (fig2).
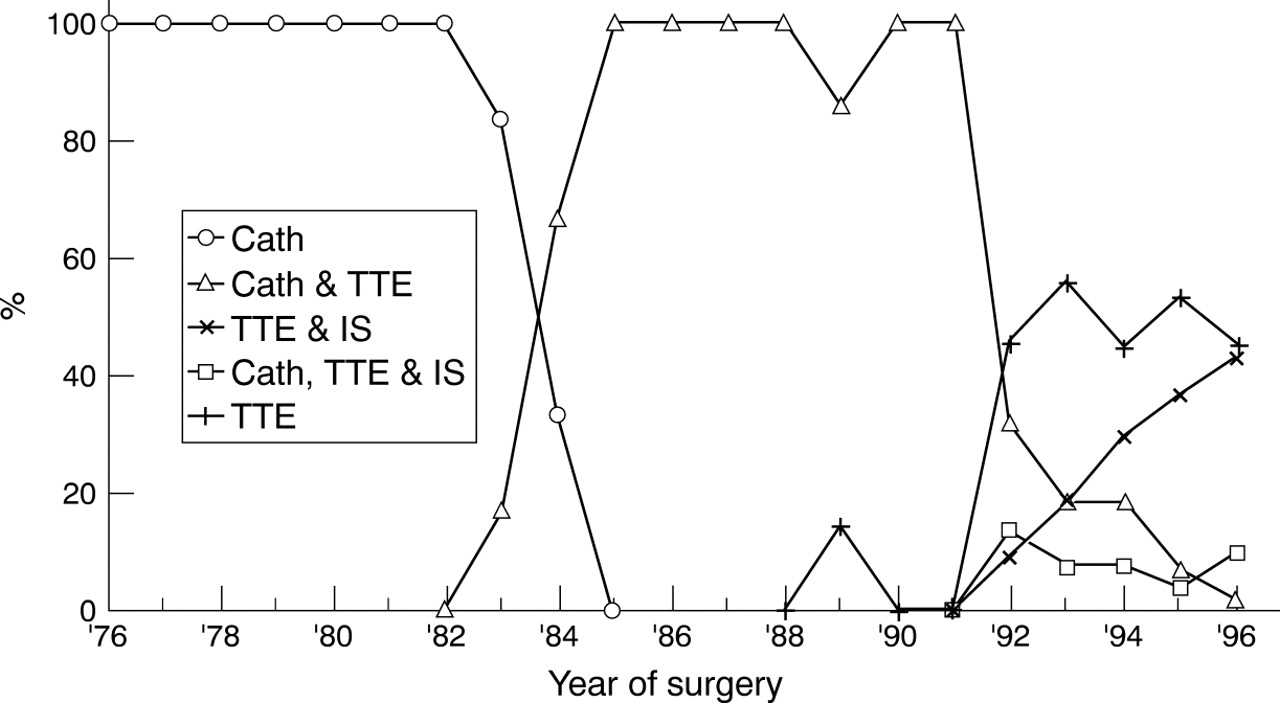
The combinations of methods used in the preoperative evaluation of the ventricular septal defect (n = 277). Thoracic radiography, electrocardiography, and transoesophageal echocardiography are not included. Cath, catheterisation; TTE, transthoracic echocardiography; IS, isotope study.

Median time (□) from suspicion of a congenital heart defect to confirmation of the diagnosis in all children for whom this information was recorded (rs = 0.90, p < 0.001, n = 191). Age at surgery versus the year of surgery (⧫) in children with pulmonary hypertension (rs = 0.79, p < 0.001, n = 147). Note the logarithmic scale on the y axis. In 18 cases, a congenital heart defect was suspected before 1976; these have been left out to minimise bias.
The different types and locations of the VSDs as diagnosed by invasive studies or by two dimensional transthoracic echocardiography are listed in table 1. A total of 221 single VSDs were classified as perimembranous (85%). In this group, echocardiography was used significantly more often in children in whom extension location was further specified as toward the outflow or inflow tract than in those children in whom extension was not defined. In the second group of children, angiocardiography was used more often (p < 0.01).
Location of the ventricular septal defect as described in the preoperative investigation
Additional cardiac defects were common, atrial septal defects, patent ductus arteriosus, and valve regurgitation being the most frequent. The prevalence of aortic regurgitation, as described in the preoperative investigation, was 20/277 (7%). Fourteen of these cases were considered mild, one was moderate, and one severe. In four cases, the degree of aortic regurgitation was not recorded.
An arbitrary classification, based mainly on the haemodynamic indication for corrective surgery, was constructed (table 2). A Qp:Qs ratio ⩾ 2, as estimated by invasive study, in combination with pulmonary hypertension as the indication for surgery, was significantly more common from 1976 to 1990 than from 1991 to 1996 (p < 0.001). On the other hand, pulmonary hypertension without estimates of Qp:Qs ratio was more common from 1991 to 1996 (p < 0.001). Small shunts without pulmonary hypertension (that is, a Qp:Qs ratio of 1.5–1.9) were significantly more common as an indication for corrective surgery from 1991 to 1996 than from 1976 to 1990 (p < 0.001). This was also found in children with borderline pulmonary hypertension (p < 0.01) and congestive heart failure with a restrictive VSD (p < 0.01). In the group of patients with restrictive VSD and aortic regurgitation in combination, six were considered mild, one moderate, and one severe (data missing for one).
Indication for surgery in relation to preoperative invasive study and age at surgery
SURGERY
There was a high frequency of additional interventions at the time of VSD closure. A total of 89 children had atrial septal defect closure, and in 58 cases a PDA was closed. Twelve children who previously had banding of the pulmonary artery performed were debanded, six undergoing reconstruction of the pulmonary artery. Seven children underwent aortic valve repair, three had mitral valve repair, and two had tricuspid valve repair. Sixteen patients had miscellaneous additional surgical interventions performed. Deep hypothermia and circulatory arrest were used in 10 patients, all operated upon between 1977 and 1985.
Early death (< 30 days after surgery) occurred in 10 children (table3). This mortality rate was significantly lower from 1991 to 1996 (one death, 0.6%) than from 1976 to 1990 (nine deaths, 8.2%) (p < 0.001).
Information about the children who died (n = 277)
Complications were classified as perioperative (occurring in the operating theatre) and postoperative (occurring in the intensive care unit). Using the classification system described in table 2, we compared the complication rates between children with large and with small VSDs. In the group of children with larger VSDs, all had either pulmonary hypertension, a left to right shunt greater than 2:1, overt heart failure, or a combination of these. Children with small VSDs all had restrictive VSDs without pulmonary hypertension, including aortic regurgitation in 10 cases and miscellaneous findings, such as an aneurysm of the sinus of Valsalva or tissue tag in the left ventricular outflow tract, in nine cases. According to this classification, 211 (76%) patients had a “large” VSD and 66 (24%) had a “small” VSD.
The single most common peri- and postoperative complication was dysrhythmia (table 4). Comparing patients who had surgery because of a large VSD from 1976 to 1990 (96 operated cases, deaths excluded) with those who had surgery from 1991 to 1996 (105 cases, deaths excluded), there was a significant decrease in the frequency of perioperative complications, from 28 cases (29%) in the early period to 16 cases (15%) in the later period (p < 0.05).There was no significant difference, however, in the rate of postoperative complications between patients with large VSDs operated on in the early (43/96 patients, 45%) or in the later (41/105 patients, 39%) period. Regarding the perioperative complication rate among children operated on from 1991 to 1996, there was no significant difference in perioperative complications between children with large (16/105 patients, 15%) and small VSDs (10/61 patients, 16%). During the same period significantly more postoperative complications (deaths excluded) occurred among children who had a large VSD (41/105 patients, 39%) than among those with a small VSD (9/61, 15%) (p < 0.005). The small number of patients (five children) who underwent surgery for a small VSD from 1976 to 1990 prevented a reasonable statistical comparison with other groups.
Peri- and postoperative complications
Postoperative pulmonary artery pressure was recorded in 139/167 patients (83%) operated on from 1991 to 1996, whereas this was recorded for only 28/110 patients (25%) who had surgery from 1976 to 1990 (p < 0.001). A total of 51 patients with postoperative pulmonary artery hypertension were retrieved from the records.
Diagnostic changes/mistakes after revaluation at surgery showed a tendency to decrease between the two time periods, but this difference was significant only with regard to localisation of the VSD (8.2%v 2.4%, p < 0.05) (table 5).
Re-evaluation of diagnosis at surgery in 1976 to 1990 and in 1991 to 1996
FOLLOW UP STUDY
There were 267 early survivors. No late deaths occurred among 264 of these patients until November 1998 (data missing for three immigrants who probably left the country). The results of clinical follow up were retrieved for 256 patients. The median follow up time was 2.3 years (10 days to 18 years), with a total of 1100 patient years. Nine patients had a reoperation because of residual VSD, one child had a reoperation with reconstruction of the mitral valve, and one child who had reconstruction of the aortic valve performed at the time of corrective surgery was reoperated on twice for aortic regurgitation, the second time with an aortic prosthesis. No mortality occurred at or after reoperation.
Residual VSD leakage was evaluated by postoperative colour Doppler using transthoracic examination in 167 patients, with residual VSD leakage found in 89 (53%). The majority of the leakages were considered insignificant. Of the 267 survivors, 241 (90%) had a transthoracic examination performed at follow up. In 153 children, a colour Doppler study was performed both after surgery and at long term follow up, with a median follow up time of 10.4 months (three days to 4.7 years). In this group, the number of patients with residual leakage in the immediate postoperative period (before hospital discharge) was 81 (53%), and the corresponding number at follow up was 47 (31%) (p < 0.001). If spontaneous closures in this group are separated over time, the mean (SE) cumulative risk of having a residual patch leakage, as studied by colour Doppler, was 8.6 (4.9)% 3–4.5 years after the immediate postoperative study (fig3).

{kind=link}
{kind=link}
{kind=link}
Cumulative risk and standard errors of having residual leakage at transthoracic echocardiography (TTE) at long term follow up. Included are the children with residual VSD/patch leakage postoperatively, detected by colour Doppler, who also had colour Doppler performed at long term follow up (n = 81).
Eight of the 256 children (3.1%) had a complete heart block at follow up (data missing for 11 children). One child who had surgery at 2 months old, with no signs of a patch or valve leakage at transthoracic examination postoperatively, had endocarditis 17 months after surgery. Seven children were found to have cerebral complications postoperatively (table 4), one of whom had a severe sequel with diplegia, hyperkinesia, mental retardation, cortically impaired vision, and epilepsy at follow up, all secondary to anoxic brain damage during surgery. In three children, varying degrees of disturbed mental development were found at follow up, but there was no obvious connection to the surgical procedure.
Discussion
The main objective of the present study was to evaluate the management of children with isolated VSD, particularly the results of surgery in relation to the diagnostic mode. Exclusion criteria were established to find a population in which the VSD was supposed to be the main prognostic factor. Even with such strict exclusion criteria, it was impossible not to include patients who received other significant surgery besides VSD closure and also had other significant heart disease. The increasing number of patients with VSD who had surgery in the later years is explained by the concentration of paediatric cardiac surgery in Sweden to two centres, including ours. In addition, the move towards liberalising indications for surgical intervention in patients with isolated VSD at our institution explains the higher number of patients in the later years, thus skewing the results. The limitations of a retrospective study of clinical decision making covering a 20 year period are obvious, namely, that not all information based on the different diagnostic methods is available for all patients and that changes in criteria for surgical intervention and changes in surgical techniques, extracorporeal circulation, and postoperative care occurred throughout the study period. We chose to compare the periods 1976 to 1990 and 1991 to 1996 mainly because colour Doppler became available in the recent time period. In addition, since 1991, paediatric cardiology, paediatric cardiac surgery, and the intensive care unit have been located in the same hospital building, facilitating the collaboration between these specialities.
A main finding of the present study is the dramatic change in diagnostic procedures used for children receiving surgery for VSD—the significant decrease in the use of invasive preoperative study in favour of non-invasive methods (fig 1). We found a decrease in the median time from suspicion of a congenital heart defect to confirmation of the VSD diagnosis from 10.3 months in 1976 to one day in 1996 (p < 0.001), largely as the result of the development and use of two dimensional echocardiography (fig 2). Early diagnosis is a prerequisite for early surgery in children with pulmonary hypertension at risk for the development of pulmonary obstructive disease, and in the present study there was a steady decline in the median age at surgery in such cases, from almost 2 years to slightly more than 3 months (fig 2).
It has long been known that two dimensional echocardiography provides a detailed assessment of the ventricular septum, especially if combined with colour Doppler.5 ,7-12 In children with perimembranous defects, the definition of the defect was more precise as to the extension to the outflow or inflow septum by non-invasive assessment than by angiocardiography (table 1). This is in line with the finding of Helmcke and colleagues that colour Doppler compared favourably with angiocardiography in the detection and localisation of VSDs.13
In the early era of colour Doppler echocardiography, great caution was taken to omit preoperative invasive evaluation in patients with VSD.6 ,14 Since then, non-invasive imaging techniques in paediatric cardiology have replaced invasive methods in the diagnosis of a number of congenital heart defects.5 ,15 Currently in our department, the main indications for invasive study in children with isolated VSD are estimation of the pulmonary vascular resistance in cases of suspected pulmonary obstructive disease, regardless of age, and the angiocardiographic localisation of possible multiple defects, when the specificity and sensitivity of colour Doppler alone is uncertain and when an associated cardiac defect is suspected.6 ,14 ,16 The change in recent years to non-invasive preoperative evaluation in children with VSD is shown in fig 1.
During the study period, hospital mortality fell significantly, with only one death during later years (8.2% v0.6%, p < 0.001), suggesting that our current preoperative management is sufficient. In studies based on cases with surgery performed before 1980, mortality rates ranged between 9.8% and 21.6%,17-20 while a trend similar to the one seen in the present study is reflected in mortality rates ranging between 0% and 3.7% in later years.1 ,4 ,21 The explanation for these improved surgical results is obviously multifactorial, related to factors such as improvements in the management of extracorporeal circulation in small children, improved surgical techniques, and better postoperative care. All deaths in our study occurred in children with preoperative pulmonary hypertension. The significant increase in later years in recording postoperative pulmonary artery pressure provided a better understanding for proper management of postoperative pulmonary hypertension. Indeed, modern drugs for the treatment of pulmonary hypertension, such as prostacyclines and nitric oxide, have been increasingly used in the postoperative period after VSD surgery at our institution.
Even though we used invasive preoperative diagnostic studies less frequently in later years, there was a decrease in the frequency of diagnostic errors in that time period, although this was significant with regard only to the location of the VSD (table 5). The most common diagnostic errors were undiagnosed atrial septal defects and, in later years, undiagnosed persistence of the left superior vena cava, PDAs, additional VSDs, or incorrectly classified VSDs, including one case of an undiagnosed prolapse of an aortic cusp.
Complications at corrective surgery were frequent and represented all those seen at surgery to repair more complicated congenital heart defects (table 4). Dysrhythmia in isolation or in combination with other complications was most common, both peri- and postoperatively. A comparison with other studies is difficult since study populations differ and complications are reported in differing degrees of detail. Hardin and colleagues reported an intraoperative complication rate of 4.2% in children who had surgery between 1986 and 1991, while major and minor postoperative complications occurred in 10.4% and 29.2%, respectively, of their patients.3 We found no significant differences in the number of perioperative complications when we compared children with large and small VSDs in later years (15% and 16%, respectively); however, postoperative complications were significantly more common in children with large VSDs than in children with small VSDs during the same time period (39% and 15%, respectively, p < 0.005). In the present study, perioperative complications were significantly lower in children with large VSDs operated upon in later years than in the early period (2% and 15%, p < 0.05), probably reflecting better intraoperative management.
No controversy exists regarding early closure of an unrestrictive VSD in order to avoid pulmonary vascular obstructive disease,3 ,22-24 but surgical closure of a restrictive VSD in an asymptomatic patient with a modest or even small shunt is more controversial.4 ,25 ,26 The deliberate change toward more liberal indications for VSD closure in our institution, exemplified by the increased number of children with restrictive VSD and small or modest shunts (Qp:Qs 1.5 to 1.99) in the latter part of the study (table 2), was largely based on significant haemodynamic abnormalities at rest and exercise in a long term follow up study of untreated patients with a restrictive VSD.27 ,28 Numerous reports have shown a high rate of spontaneous closure in small VSDs,22 ,29-33 which certainly would favour postponing the discussion of surgery in the asymptomatic child with such a defect until at least the age of 4–5 years.
There is less controversy about the indication for VSD closure in patients with concurrent aortic regurgitation.34 ,35 In an early study, the prevalence of aortic regurgitation was reported to be approximately 5% in all children with VSD.36 The progressive nature of this lesion is well illustrated by the finding of Otterstad and colleagues.37 We found aortic regurgitation in 7% of all patients, constituting the indication for VSD closure in 5% of our cases in recent years, as opposed to 1% before 1991 (table2). The best opportunity to prevent progressive aortic regurgitation may well be early in the course of this complication, but the optimal timing of surgical intervention in this subgroup of patients with VSD remains to be defined in long term follow up studies.
Reoperations because of patch leakage were performed in nine children (3.4%), which is similar to the rate reported in other studies (0.6–4.7%).1 ,2 ,18 ,23 ,24 ,38 ,39 In spite of a high incidence of patch leakages revealed by colour Doppler in the immediate postoperative period after VSD surgery, few studies have concerned the fate of such leakages over time. In the present study, the number of children with a patch leakage, as studied by colour Doppler, was found to decrease over time (fig 3). This is in agreement with the finding by Hardin and colleagues, who reported that the number of children with patch leakage decreased from 41.7% to 10.4% after surgery for large VSDs.3 Although the colour Doppler technique is the most accurate non-invasive way to detect small VSDs, its sensitivity and specificity are severely affected by improper gain settings, which may skew the results in both directions. Underestimation of the number of children with a small patch leakage may be caused by the relative inaccuracy of colour Doppler in detecting a small leakage in older children. With these limitations in mind, our findings suggest that minor residual VSDs/patch leakages can be expected to close spontaneously.
In this study, no late mortality occurred, in contrast to findings in other studies in which late mortality ranged from 9.0% to 20.3% in surgical procedures performed before 198018 ,19 ,38 and from 0% to 4.3% in studies after 1980.1 ,3 ,4 Serious long term complications were found in the present study and included developmental retardation in at least one patient caused by severe cerebral complications at the time of surgery. A comprehensive analysis of such complications is needed but was not within the scope of the present study.
Acknowledgments
Our thanks to Mrs Ingegerd Tiblad for excellent secretarial help.