Article Text

Abstract
OBJECTIVE To investigate whether genetic diversity of Helicobacter pyloriinfluences its association with coronary heart disease, and specifically whether the risk is confined to infection with the more virulent strains bearing the cytotoxin associated gene-A (cagA) antigen.
DESIGN AND SETTING Case–control study in hospital admitting unselected patients with myocardial infarction.
METHODS AND SUBJECTS Serological status for cagA and H pylori were determined in 342 cases of acute myocardial infarction and 214 population based control subjects free of clinical coronary heart disease.
RESULTS 38.0% of cases and 30.8% of controls were cagA seropositive (odds ratio 1.38, 95% confidence interval (CI) 0.94 to 2.01, p = 0.08). In subjects < 65 years old (153 cases, 153 controls), cagA seropositivity was associated with a 1.80-fold increase (95% CI 1.07 to 3.03, p = 0.02) in myocardial infarction risk, which increased further to 2.25-fold (95% CI 1.12 to 4.53, p = 0.01) in subjects < 55 years. There was no significant association of cagA status with classical coronary heart disease risk factors. H pylori seropositivity was present in 60.2% of cases and 53.7% of controls (odds ratio 1.12, 95% CI 0.83 to 1.51, p = 0.43). H pyloriseropositivity was not increased in young cases and did not show any interaction with age.
CONCLUSIONS The association of chronic H pylori infection with risk of myocardial infarction appears to be restricted to cagA bearing strains. The association is age dependent and stronger in younger subjects. Genetic heterogeneity of H pylori may explain some of the discordant findings with regard to the association of H pylori with coronary heart disease.
- coronary heart disease
- risk factors
- Helicobacter pylori
Statistics from Altmetric.com
Helicobacter pylori is a microaerophilic spiral shaped Gram negative bacterium that colonises the gastric lumen of humans and other primates. Infection is commonly acquired in childhood and is usually chronic.1 Raised concentrations of IgG antibodies toH pylori are a fairly reliable indicator of the presence of infection. The bacterium is now recognised to be of major aetiological importance in peptic ulcer disease2 and in gastric cancer.3 More recently, in conjunction with a variety of other chronic infections, interest in the possible association between H pylori infection and coronary heart disease has developed.4 Mendall and colleagues were the first group to report a higher prevalence ofH pylori seropositivity in patients with coronary heart disease compared with healthy volunteers.5However, subsequent studies have produced conflicting findings6-12 and the significance of the association remains uncertain.4 Confounding by the strong relation ofH pylori infection to other coronary heart disease risk factors such as age and social class may, at least partly, explain the contradictory results. However, recent studies have shown that there is also genetic diversity withinH pylori which affects its virulence. Specifically, strains bearing the cytotoxin associated gene-A (cagA) provoke a heightened inflammatory response in vivo13 and show a stronger relation with peptic ulcer disease14 and gastric cancer.15 There is increasing evidence, from both clinical and experimental observations, that inflammation plays an important role in coronary heart disease.16-18 Thus it is possible that any impact of H pyloriinfection on coronary heart disease is crucially dependent on the type of infecting strain.
In a previous study9 comparing subjects with acute myocardial infarction with population based controls, we observed no overall association between H pyloriseropositivity and myocardial infarction risk despite adjustment for covariates. To investigate whether the type ofH pylori strain causing the infection is of relevance, we have analysed blood samples from our cohorts for anti-cagA antibodies as an indicator of infection with more virulentH pylori strains. We report a significant and age dependent association of infection with cagA positiveH pylori strains and risk of myocardial infarction. Our findings suggest that genetic heterogeneity ofH pylori may explain some of the discordant findings with regard to the association ofH pylori with coronary heart disease.
Methods
SUBJECTS
The recruitment of patients and controls has been previously described.9 Briefly, patients who satisfied the World Health Organisation criteria for myocardial infarction19were recruited from admissions to the coronary care unit (CCU) at Leicester Royal Infirmary. The CCU, serving a population of around 300 000, accounts for more than 65% of admissions of cases with myocardial infarction in Leicester. The period of recruitment was between July 1993 and April 1994, and more than 97% of eligible subjects were recruited. Control subjects were recruited randomly from adult visitors to patients with non-cardiovascular illnesses on general medical and surgical wards at the Leicester Royal Infirmary, to provide subjects likely to be representative of the source population from which the cases came. Those reporting a history of myocardial infarction or angina were excluded from the analysis.
Cases and controls filled in a standard questionnaire about their personal histories, had height and weights measured, and provided blood samples for laboratory analysis. The study was approved by the local research ethics committee.
BIOCHEMICAL MEASUREMENTS
Serum total and high density lipoprotein (HDL) cholesterol were measured using a Kodak Ektachem E700 CXR automatic analyser in a quality controlled hospital biochemistry laboratory. For cases, the first blood sample taken after admission was used for the analysis.
DETERMINATION OF H pylori AND cagA SEROLOGICAL STATUS
H pylori status was determined serologically, as described previously,9 using an established IgG enzyme linked immunosorbent assay (ELISA) based on an ultracentrifuged sonicate antigen. IgG antibodies to the cagA protein were quantified on whole blood samples using a commercial ELISA kit (Helicobacter p120 (CAGA) ELISA, Viva Diagnostics, Hurth, Germany). The ELISA was validated by concurrent western blot analysis of 207 of the samples, randomly chosen, to confirm the presence or absence of anti-cagA antibodies using a reference strain (NCTC 11637, National Collection of Type Cultures, London, UK) as antigen. Optimal sensitivity and specificity values were calculated for the assay from these data. Using an ELISA unit value of 5.2, 17 of 207 ELISA samples were false positive (that is, they had a unit value ⩾ 5.2, but no detectable anti-cagA antibody on immunoblot) and 16 of 207 ELISA samples were false negative (that is, a unit value of < 5.2, but detectable anti-cagA antibody on immunoblot). Therefore, optimal sensitivity and specificity values were 86.7% and 85%, respectively, for use of the ELISA on this study population.
STATISTICAL ANALYSIS
Distribution of cagA seropositivity and qualitative risk factors between cases and controls or qualitative risk factors between cagA positive and cagA negative cases or controls were compared using the χ2 test. Quantitative sample means were compared by analysis of variance. Logistic regression was used to analyse the effects of cagA seropositivity on myocardial infarction status and its interaction with linear age effect adjusted for sex. Adjustment was then made for other covariates by including them in the regression. The effects of these adjustments were tested by comparing the odds ratios associated with cagA and the corresponding age interaction term, when estimated with and without adjustment.20 In these analyses, age was adjusted for by pooling estimates made at different ages to obtain Mantel–Haenszel estimates and separately, by including a linear age term but no interaction, in a logistic regression. The changes in the odds ratio associated with cagA seropositivity adjusted for age were then plotted against the appropriate age cut off.
Results
In all, 556 subjects (342 cases, 214 controls) were analysed. Table 1 summarises their characteristics. Cases were significantly older than controls, and classical risk factors (hypertension, diabetes, smoking, and positive family history) were more prevalent in cases. Body mass index and total and HDL cholesterol concentrations were similar.
Characteristics of cases and controls
Three hundred and twenty one subjects wereH pylori seropositive (206 of 342 cases (60.2%) and 115 of 214 controls (53.7%), odds ratio (OR) 1.12, 95% confidence interval (CI) 0.83 to 1.51, p = 0.43); 196 subjects were cagA seropositive. The distribution of cagA seropositivity in cases and controls is shown in table 2.
Distribution of cagA seropositivity in cases and controls
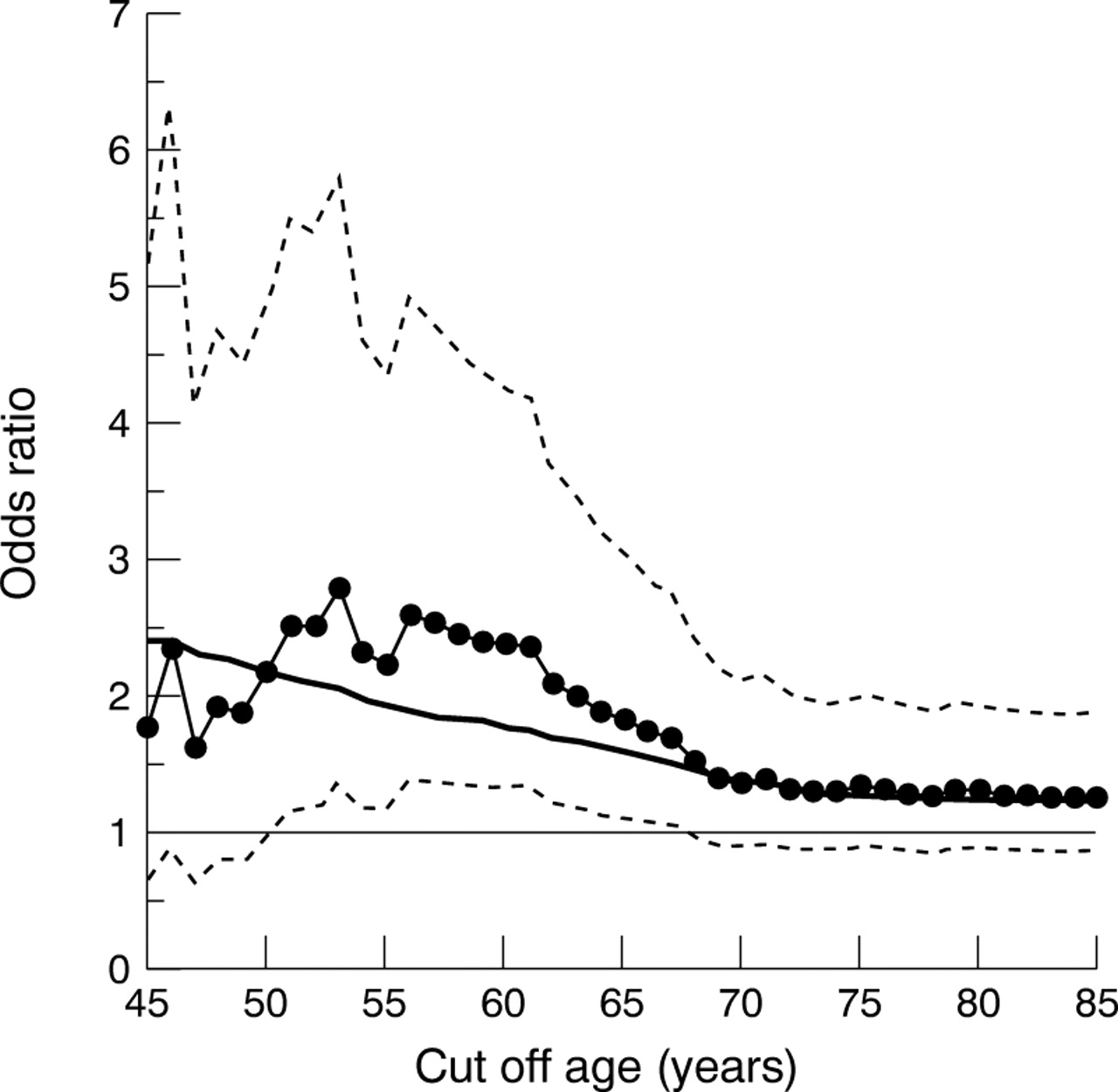
In the whole cohorts, 38.0% of cases and 30.8% of controls were cagA seropositive (odds ratio 1.38, 95% CI 0.94 to 2.01, p = 0.08). Because of the significant difference in age distribution of cases and controls we examined the potential impact of this on the association of cagA seropositivity with risk of myocardial infarction. In subjects under 65 years of age (n = 153 cases, 153 controls) there was 1.80-fold (p = 0.02) increase in myocardial infarction risk associated with cagA seropositivity (prevalence: cases 37.2%, controls 24.8%), which increased further to 2.25-fold (p = 0.01) in subjects less than 55 years old (prevalence: cases 40.9%, controls 23.8%) (table 2). The association remained significant in the younger age groups when adjusted for age and sex (table 2). In the Mantel–Haensel analysis, the age and sex adjusted odds ratio remained significant to an age of about 65 years (fig 1). A logistic regression analysis showed a significant interaction (p = 0.03) between age and the effect of cagA seropositivity on risk of myocardial infarction. The odds ratio associated with cagA seropositivity declined on average by 30% (95% CI, 3–49%) per decade (fig 1, solid line). Analysis forH pylori seropositivity showed no similar increased risk in younger subjects9 or interaction with age (data not shown).
{kind=link}
Age dependency of the association of cagA positive strains of H pylori with risk of myocardial infarction. The odds ratio estimates for risk of myocardial infarction associated with cagA seropositivity for different age cut off values from the Mantel–Haenszel analysis adjusted for age and sex are shown in the line with the closed circles (with 95% confidence intervals in dotted lines). The corresponding estimates from the logistic regression are shown by the solid line.
The distribution of risk factors in cases stratified by cagA status is shown in table 3. There was no significant association of cagA status with any of the risk factors, and adjustment of the logistic regression for the covariates had no significant impact on either the overall association (p = 0.85) or the interaction with age (p = 0.81). There was no significant association of any risk factors with cagA status in controls either (data not shown).
Distribution of risk factors in cases according to cagA status
Discussion
Our finding in this study of a specific association between cagA positive strains of H pylori and the risk of premature myocardial infarction adds to the current debate about the possible role of chronic bacterial infections in the pathogenesis of coronary heart disease.4 ,18 Studies to date on the roleH pylori have produced very conflicting results.5-12 Study size, study design, and the failure to control for potential confounding factors such as socioeconomic class have all been proposed as explanations for the contradictory findings.4 ,18 In this study we provide evidence that any effect of H pylori infection on coronary heart disease risk may also be related to the type of infecting strain. Such risk appeared independent of classical risk factors for coronary heart disease.
The specific association of cagA positiveH pylori strains with myocardial infarction risk is biologically plausible. The cagA gene and the associated vacuolating cytotoxin (VacA) define type IH pylori strains which produce a more pronounced gastric inflammatory response, including the induction of interleukin 6 and 8 and tumour necrosis factor α, compared with type II (cagA negative) strains,13 ,21 and are more strongly associated with peptic ulcer disease14 and gastric tumours.15 Recent studies have shown that this enhanced response in type I strains reflects the presence of a 40 kb DNA insertion flanking cagA (the cag region), which has the typical features of a pathogenicity island (PAI) encoding for several virulent factors which promote the inflammatory response.22Increasing evidence suggests that inflammation (both systemically as well as locally) plays an important role in the development of coronary heart disease and particularly the progression to acute coronary syndromes.16-18 Systemic markers of inflammation such as C reactive protein and acute phase reactants such as fibrinogen and serum amyloid A have been shown to be associated prospectively with myocardial infarction risk,23-28 and part of the beneficial effects of aspirin on coronary risk may be related to its anti-inflammatory rather than its antiplatelet effect.28Thus it is possible that cagA positiveH pylori strains increase the risk of myocardial infarction through the promotion of an enhanced inflammatory response. Indeed, H pylori seropositivity has been associated with raised concentrations of fibrinogen and C reactive protein,29 ,30 although, as in the case of the association with coronary heart disease, results have been mixed; a recent meta-analysis31 suggested that the correlations reflected chance or publication bias. However, studies in such populations have not taken into account the genetic heterogeneity ofH pylori.
The association of cagA positive H pyloristrains with coronary heart disease has also been examined by Pasceri and colleagues.32 In 88 patients with ischaemic heart disease (mean (SD) age 57 (8) years, 74 men) and in 88 matched controls, they observed a 3.8-fold adjusted increase in risk of ischaemic heart disease in cagA positive subjects (prevalence of cagA seropositivity: cases 43%, controls 17%). Interestingly, they also observed an increase in overall prevalence ofH pylori seropositivity in cases (62%v 40%). Prevalence of cagA negative strains was similar in patients and controls (19% v23%). Pasceri and colleagues studied patients with a range of coronary syndromes including severe unstable angina, acute myocardial infarction, and chronic stable angina, while our larger study was focused on acute myocardial infarction only. Although the prevalence of infection by cagA positive strains was similar in Pasceri's three patient groups, further studies are needed to define the precise relation of infection with cagA bearing strains with different coronary syndromes, especially as a recent study by Koenig and colleagues found no association in 312 patients with stable coronary heart disease compared with 479 control subjects.33 However, our findings emphasise the point that the ability to detect any overall association of H pylori seropositivity with coronary heart disease may depend not only on the population prevalence of H pylori infection but also on the relative proportion infected with cagA positive strains. Studies have shown there is wide variation (28–82%) in cagA seroprevalence in different countries.34
The finding that the association of risk of myocardial infarction with cagA positive H pylori strains was age dependent is not entirely unexpected as the associations of most vascular risk factors with coronary heart disease tend to be stronger in younger than in older individuals. Although this is the most likely explanation, it needs also to be noted that several studies have shown that the accuracy of serological testing forH pylori, and in particular the specificity, declines with age.35 ,36 The reasons for this are unclear but cross reactivity between antibodies owing to increased antigenic exposure with age may be a factor. However, although this could explain why an association was not observed in older subjects in our study, it is important to emphasise that it does not affect the significance of the association seen in subjects under 65 years.
LIMITATIONS
Our study has several limitations common to cross sectional studies. In particular we cannot exclude the possibility that unrecognised population stratification for relevant factors influenced the findings. Specifically, socioeconomic status is known to affect both the prevalence of H pylori infection and the risk of coronary heart disease.4 ,18 Although our controls were recruited from hospital visitors, specifically to provide healthy subjects likely to be representative of the source population from which the cases came, details of socioeconomic status were not obtained, and we were not able to adjust for this. However, the specific association with cagA seropositivity in the absence of an overall increase in H pylori prevalence in cases argues against this being the explanation for the finding. Another limitation is that, although the effect of infection with cagA strains appeared independent of classical coronary heart disease risk factors, the study does not provide direct mechanistic information. Therefore, the association of cagA positive strains ofH pylori on risk of coronary heart disease needs to be confirmed in further—ideally prospective—studies, and whether the effect is mediated through an enhanced inflammatory response needs to be determined. Such studies are worthwhile not only because they may provide important insights on the pathophysiological basis of coronary syndromes, but also because of the considerable potential, if the association is proven, of new forms of therapeutic and preventative treatments directed towards infection eradication.