Article Text

Abstract
OBJECTIVE To test the hypothesis that patients with unstable coronary syndromes show accentuated compensatory vessel enlargement compared with patients with stable angina, and that this may in part be related to increased coronary artery distensibility.
DESIGN AND PATIENTS In 23 patients with unstable coronary syndromes (10 with non-Q wave myocardial infarction and 13 with unstable angina), the culprit lesion was investigated by intravascular ultrasound before intervention. The vessel cross sectional area (VA), lumen area (LA), and plaque area (VA minus LA) were measured at end diastole and end systole at the lesion site and at the proximal and distal reference segments. Similar measurements were made in 23 patients with stable angina admitted during the same period and matched for age, sex, and target vessel. Calculations were made of remodelling index (VA at lesion site ÷ VA at reference site), distensibility index ([(ΔA/A)/ΔP] × 103, where ΔA is the luminal area change in systole and diastole and ΔP the difference in systolic and diastolic blood pressure measured at the tip of the guiding catheter during a cardiac cycle), and stiffness index β ([ln(Psys/Pdias)]/(ΔD/D), where Psys is systolic pressure, Pdias is diastolic pressure, and ΔD is the difference between systolic and diastolic lumen diameters). Positive remodelling was defined as when the VA at the lesion was > 1.05 times larger than at the proximal reference site, and negative remodelling when the VA at the lesion was < 0.95 of the reference site.
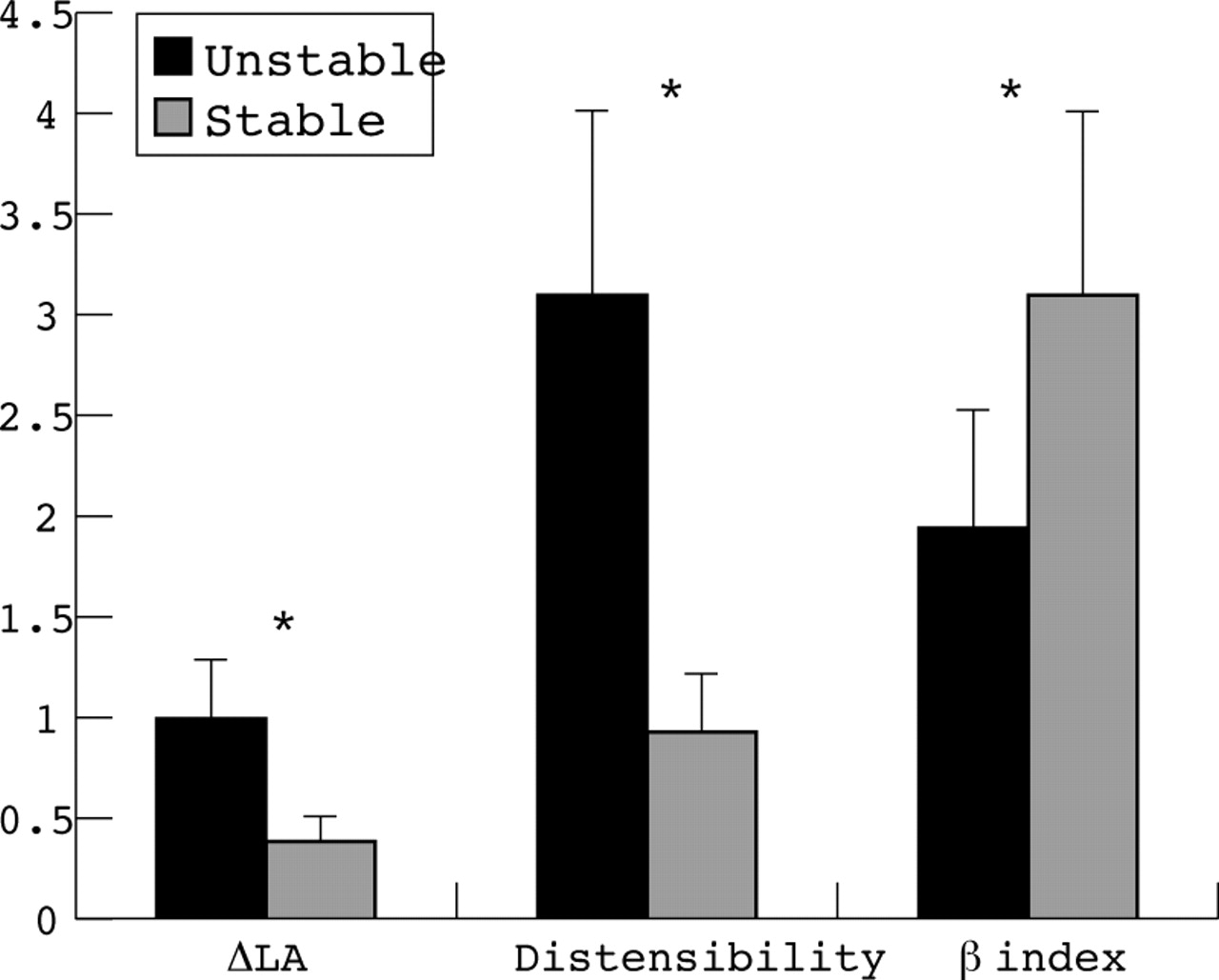
RESULTS Mean (SD) LA at the lesion site was similar in both groups (4.03 (1.8) v4.01 (1.93) mm2), while plaque area was larger in the unstable group (13.29 (4.04) v 8.34 (3.6) mm2, p < 0.001). Remodelling index was greater in the unstable group (1.14 (0.18) v 0.83 (0.15), p < 0.001). Positive remodelling was observed in 15 patients in the unstable group (65%) but in only two (9%) in the stable group (p < 0.001). Negative remodelling occurred only in two patients with unstable symptoms (9%) but in 17 (74%) with stable symptoms. At the proximal reference segment, the difference in LA between systole and diastole was 0.99 (0.66) mm2 in the unstable group and 0.39 (0.3) mm2 in the stable group (p < 0.001), and the calculated coronary artery distensibility was 3.09 (2.69) and 0.94 (0.83) per mm Hg in unstable and stable patients, respectively (p < 0.001). The stiffness index β was lower in patients with unstable angina (1.95 (0.94) v 3.1 (0.96), p < 0.001).
CONCLUSIONS Compensatory vessel enlargement occurs to a greater degree in patients with unstable than with stable coronary syndromes, and is associated with increased coronary artery distensibility.
- coronary artery disease
- remodelling
- compliance
- angina pectoris
Statistics from Altmetric.com
Compensatory arterial enlargement (vascular remodelling) in response to atherosclerosis was first described in animal experiments1and later demonstrated in humans in a landmark necropsy study.2 Subsequently, intravascular ultrasound (IVUS) confirmed these observations in vivo3 and also showed paradoxical shrinkage of the vessel in reaction to plaque accumulation (negative remodelling).4-6 Although the trigger mechanisms for these different forms of remodelling in response to plaque accumulation are incompletely understood, alterations in flow dynamics—and in particular shear stress—at the surface of the endothelial cell are thought to play a critical role in plaque formation and vessel response.7 ,8 As the ability of the vessel to distend is dependent on intact endothelial function,9 vessel compliance may influence the remodelling pattern. Preliminary data show that eccentric plaques have better remodelling capability,10 which may result from better distensibility and preserved endothelial function.11Whether these factors—remodelling ability, vessel compliance, and plaque topography—influence the clinical presentation is unknown.
Evidence for a relation between arterial remodelling and increased vulnerability to plaque rupture has recently been accumulating. Vulnerability to plaque rupture has traditionally been associated with a decrease in the amount of collagen and smooth muscle cell components, especially in the shoulder region.12 Recently, Pasterkamp and colleagues observed similar findings in positively remodelled vessels, with abundance of inflammatory cells, deficiency of smooth muscle cells, and fibrous caps in femoral arteries at necropsy.13 Preliminary reports from two in vivo IVUS studies have suggested a greater degree of positive remodelling in patients with unstable angina14 and acute myocardial infarction15 than in patients with stable coronary syndromes, suggesting that highly remodelled vessels may serve as a substrate for plaque rupture. On the other hand, mechanical forces such as distensibility at the luminal surface may be a more important determinant of plaque vulnerability. Typically, plaque rupture occurs in the shoulder region,16 suggesting a localised imbalance in strain forces or the transmission of those forces between diseased and less diseased segments of the vessel.
Our aim in this study was to assess the degree of remodelling and coronary artery compliance in patients with atherosclerotic coronary artery disease in two distinct clinical scenarios. We hypothesised that vascular distensibility is greater in patients with unstable than with stable coronary syndromes and that this may be related to differences in remodelling patterns.
Methods
PATIENT POPULATION
Patients with unstable coronary syndromes who had undergone a cardiac catheterisation procedure at Stanford University were eligible for inclusion. Of those, 23 patients had undergone IVUS imaging before any catheter based intervention; none had undergone previous intervention to the target lesion. All lesions were located in native vessels; vein grafts were excluded from this analysis. Additionally, 23 patients with stable angina were identified who underwent preinterventional IVUS imaging during the same period. Patients were matched for sex, age, target vessel, and where possible target segment. Two patients in the stable angina group were excluded from analysis because extensive calcification of the target segment precluded precise measurement of vessel area. Informed consent was obtained from all patients.
INTRAVASCULAR ULTRASOUND IMAGE ACQUISITION AND ANALYSIS
A 3.2 French mechanical imaging catheter (Microview, CVIS/Boston Scientific Corporation, San Jose, California, USA) with a single element transducer or a 3.5 French solid state imaging device (Visions five-64, EndoSonics Corporation, Rancho Cordova, California, USA) was used. The mechanical transducer was rotated within the catheter at 1800 rpm to provide cross sectional images on an ultrasound diagnostic imaging console (ClearView, CVIS/Boston Scientific Corporation), or a 64 element phased array system (Oracle, In-Vision, EndoSonics Corporation) was implemented, producing similar cross sectional images in real time. Intracoronary glyceryl trinitrate (200 μg) was given during all IVUS studies before imaging. The IVUS catheter was tracked over a 0.014 inch (0.36 mm) guide wire up to a position distal to the diseased segment. Ultrasound time gain compensation settings were adjusted to allow maximum grey scale differentiation for the cross sectional images within the target segment. All IVUS studies were recorded on ½ inch high resolution super VHS tapes for off-line analysis.
Quantitative (cross sectional) analysis of the IVUS images was performed using a commercially available software program (TapeMeasure, Indec Corporation, Mountain View, California, USA). Validation of qualitative and quantitative IVUS analysis has been reported previously.17 ,18 Plaque plus media cross sectional area was used as a surrogate of plaque area, because media thickness cannot be measured accurately at imaging frequencies between 20 and 40 MHz.19 For each cross section the following measurements were made:
vessel area (assumed to be equal to external elastic membrane area, as adventitial thickness cannot be determined;
lumen area;
plaque area (vessel area minus lumen area);
per cent area stenosis (plaque area divided by vessel area × 100).
Cross sections with excessive calcification (calcium arc > 90°) were excluded from analysis because of acoustic shadowing of deeper structures (which precludes the precise measurement of the vessel area). Lesions with less than 90° of calcium were measured by extrapolation assuming that the vessel circumference is circular, and by examination of adjacent non-calcified segments as described previously.20 Eccentricity was calculated as the ratio of minimum to maximum plaque thickness, and an eccentric lesion was defined by an eccentricity index of < 0.33 or by the presence of an arc of disease-free arterial wall within the lesion. In each coronary artery, a 10–20 mm vessel segment was identified in which the most severe stenosis was included and no side branches were observed. Three sites were selected for analysis: the lesion site that had the smallest lumen area by IVUS and > 50% area stenosis, and the proximal and distal reference sites that had the largest lumen area and < 50% area stenosis. A remodelling index was calculated by dividing the vessel area at the lesion site by the vessel area at the proximal reference site. Positive remodelling was considered present when the ratio of vessel cross sectional area at the lesion site to that at the proximal reference segment exceeded 1.05, and negative remodelling when the ratio was < 0.95. When the vessel area at the lesion site was between those numbers, remodelling was considered to be intermediate. Two independent observers, blinded to each other's dataset and to the clinical patient data, reviewed all IVUS tapes and performed the measurements.
CORONARY ARTERY DISTENSIBILITY MEASUREMENTS
As baseline vascular tone can affect coronary artery distensibility,21 individual variation of the vascular tone was minimised by giving intracoronary glyceryl trinitrate before the IVUS study. The largest luminal area assessed by IVUS was determined by tracing the lumen–intima border at peak systole, and the smallest luminal area at peak diastole within one cardiac cycle (fig1). Changes in intracoronary pressure during one cardiac cycle were measured at the tip of the guiding catheter. The distensibility index of the coronary artery was defined as [(ΔA/A)/ΔP] × 103/mm Hg, where ΔA represents the luminal area change between systole and diastole, A the smallest luminal area in diastole, and ΔP the difference in systolic and diastolic blood pressure, as described previously.22 ,23Stiffness index, β, a variable considered independent of changes in arterial blood pressure,24 was calculated using the following equation: β = [ln(Psys/Pdias)]/(ΔD/D), where Psys represents the systolic pressure, Pdiasthe diastolic pressure, ΔD the difference between systolic and diastolic lumen diameters, and D the diastolic luminal diameter. All reported measurements represent the average of two independent observers from different cardiac cycles.

Comparison of the pulsatile variation of the cross sectional lumen area of a 77 year old male patient with an unstable lesion in his proximal left anterior descending artery (A) and of an age and target vessel matched patient with stable angina (B). The cyclic variation is graphically illustrated in the left panels, with the corresponding intravascular ultrasound images on the right. The change in luminal area over the cardiac cycle is more pronounced in the unstable patient. Empty circles indicate points of measurements. D, diastole; S, systole.
INTEROBSERVER AND INTRAOBSERVER VARIABILITIES
Cross sectional lumen and vessel areas of the lesion and reference sites of 10 randomly selected patients were measured by two independent observers and by one observer at two separate times. These data were used in the assessment of interobserver and intraobserver variabilities. The results were expressed as the difference between the two sets of measurements, and linear regression was performed.
STATISTICAL ANALYSIS
Data are presented as the mean (SD). Comparison between variables in the two groups was made using the unpaired Studentt test. Non-parametric data were compared using the Mann–Whitney rank sum test. Interobserver and intraobserver variability was evaluated using simple linear regression analysis. A value of p < 0.05 was considered significant.
Results
Baseline characteristics of the two study groups are presented in table 1. Of the 23 patients with unstable coronary syndromes, 10 had suffered a non-Q wave myocardial infarction and the remaining 13 were categorised according to the Braunwald classification of unstable angina.25 Patients in the stable angina group were categorised on the basis of the Canadian Cardiovascular Society grading scale.26 No significant differences between the groups were detected.
Baseline characteristics of the study population
VESSEL REMODELLING
The mean (SD) lumen area, vessel area, and plaque area at the lesion site, together with the remodelling index, are shown in fig 2. Lumen area was similar between groups (4.03 (1.80)v 4.01 (1.93) mm2), while plaque and vessel areas were greater in unstable patients (13.29 (4.04)v 8.34 (3.60) mm2, p < 0.001 and 17.35 (4.66) v 12.35 (4.90) mm2, p < 0.001). The remodelling index was greater in patients with unstable coronary syndromes (1.14 (0.18)v 0.83 (0.15), p < 0.001). Positive vessel remodelling was observed in 15 unstable patients (65%) but in only two of the stable angina group (9%) (p < 0.001). Conversely, negative remodelling occurred only in two patients (9%) with unstable angina but in 17 patients (74%) with stable symptoms.

Cross sectional lumen area (LA), plaque area (PA), and vessel area (VA) are shown for each patient group at the lesion site. Remodelling index (RI) is calculated as VA at the lesion site divided by VA at the proximal reference segment. *p < 0.001.
CORONARY ARTERY COMPLIANCE
Differences in vascular distensibility were maximal at the proximal reference segment as compared with the lesion site and the distal reference segment. Relevant data are given in table 2. The difference in lumen area between systole and diastole was significantly greater in unstable patients. Plaque eccentricity (0.28 (0.17)v 0.33 (0.18)) and plaque area (7.11 (3.33)v 6.31 (2.5) mm2) at the proximal reference site were not significantly different between the two groups. Calculated coronary artery distensibility at the proximal reference was greater in unstable patients (3.09 (2.68)v 0.94 (0.83), p < 0.001), indicating better vessel compliance (fig 3). Similarly, the β stiffness index was lower in patients with unstable symptoms (1.95 (0.94)v 3.10 (0.96), p < 0.001; fig 3). Analysis of the distal reference segment also showed greater vessel distensibility (2.77 (2.14) v 1.19 (0.88), p = 0.002) and lower β stiffness index (2.45 (1.59)v 2.86 (1.0), p = 0.04) in the unstable patient group. At the lesion site, there was no difference in plaque eccentricity (0.35 (0.23) v 0.34 (0.20)), although maximum plaque thickness was greater in patients with unstable angina (2.03 (0.53) v 1.46 (0.36) mm, p < 0.001). Vascular distensibility tended to be greater in the unstable group, but this did not reach significance (1.84 (1.36)v 0.95 (0.53), p = 0.06).
Haemodynamic variables, arterial dimensions, and vascular compliance at the proximal reference segment
{kind=link}
{kind=link}
{kind=link}
Difference in lumen area (ΔLA, mm2), vessel distensibility (per mm Hg), and β stiffness index (B) at the proximal reference site for each patient group. *p < 0.001.
INTEROBSERVER AND INTRAOBSERVER VARIABILITIES
Intraobserver correlation coefficients and mean (SD) differences were 0.996 and 0.03 (0.30) mm2 for vessel area and 0.998 and 0.01 (0.19) mm2 for lumen area; interobserver correlation coefficients and mean (SD) differences were 0.922 and 0.20 (1.10) mm2 for vessel area and 0.930 and 0.16 (1.00) mm2 for lumen area.
Discussion
Our results show that compensatory vessel enlargement occurred significantly more often and to a greater degree in patients with unstable coronary syndromes than in those with stable angina. Vessel shrinkage was observed in most of the patients in the stable angina group but in only two patients with an acute presentation. Furthermore, the compliance of the vessel wall was significantly greater in unstable patients, indicating that there was a relation between vascular distensibility and positive vessel remodelling.
VASCULAR REMODELLING AND PLAQUE VULNERABILITY
The finding that greater degrees of positive remodelling are associated with unstable coronary syndromes is consistent with previous observations from IVUS studies.14 ,15 Tauth and colleagues showed that plaque composition correlated with the degree of remodelling in that fibrocalcific plaques were associated with constrictive remodelling while soft plaques showed more positive remodelling.27 Similarly, Pasterkamp and associates, in a necropsy study of femoral arteries, found that histological markers of plaque vulnerability were seen most often in the vessels that had undergone the most adaptive remodelling.13 Large numbers of macrophages and T lymphocytes, small numbers of smooth muscle cells, and scant collagen were found more often in the cross sections with the largest plaque and vessel area than in those with the least plaque and the smallest vessel area. This phenomenon can be termed the “remodelling paradox”, suggesting that while chronic luminal narrowing caused by plaque formation is retarded, the risk of plaque rupture and acute thrombotic occlusion may be augmented.
Those vessels that readily undergo compensatory enlargement can accumulate a larger plaque burden, while preserving the luminal area, compared with vessels that do not remodel or that undergo negative remodelling. In a necropsy study by Davies and colleagues on aortic plaques from sudden death victims, ulceration and thrombosis were characteristic of plaques with a high proportion of their volume occupied by extracellular lipid, suggesting that a large volume of atheroma within the plaque predisposes to rupture.12 In the present study, patients with unstable coronary syndromes had a significantly larger plaque area at the lesion site than patients with stable angina, indicating that the greater plaque burden was a factor in the pathogenesis of their clinical presentation.
Patients who undergo compensatory vessel enlargement may accommodate substantial atheromatous plaque while remaining free of anginal symptoms, and may thus remain undiagnosed. Even at diagnostic coronary angiography, luminal encroachment is often not present, leading to an erroneous underestimation of the degree of plaque burden. Comparing IVUS with coronary angiography, Mintz and colleagues showed a significant amount of plaque accumulation by IVUS that went undetected by angiography.28 This factor may contribute to the high incidence of plaque rupture at angiographically insignificant lesion sites.29-31
VASCULAR COMPLIANCE AND COMPENSATORY VESSEL ENLARGEMENT
To further evaluate differences between patients with acute and stable coronary syndromes, we determined vascular distensibility in each patient group and found it to be significantly greater in the unstable patients. Two recent studies of coronary artery distensibility using IVUS in patients with coronary artery disease illustrate the influence of plaque topography on vessel compliance.22 ,23In eccentric lesions, increasing thickness of the intima–media complex was associated with a progressive decrease in vascular distensibility. Other factors influencing vessel compliance include age, vessel size, and intimal composition.32 Our present study is the first to measure both vascular distensibility and remodelling in patients with stable and unstable coronary syndromes. The results suggest a relation between compensatory vessel enlargement and increased vascular distensibility. In addition to distensibility, the stiffness index β was determined as the slope of the exponential function between the relative arterial pressure and the distension ratio of the artery.33 This index has been shown to be independent of the intraluminal pressure within the physiological range24and is thus a more robust measure of vessel compliance. Using the β stiffness index in the present study, significant differences were detected: patients with stable angina had stiffer vessels than those with unstable coronary syndromes.
The association between increased vessel compliance and unstable coronary syndromes can be explained in several ways. Greater compliance may augment positive remodelling by increased pulsatile stretch, leading to heightened activity of metalloproteinases.34These enzymes have been linked to degradation of the matrix skeleton of the vessel and thus may weaken the vascular wall.35Additional mechanisms could lead to a change in the matrix content, potentially promoting the remodelling process—for example, shifts in the ratio of collagen to elastin affect the elastic behaviour of arterial walls.36 As vulnerable plaques are known to contain less collagen,12 it is possible that these structural differences between unstable and stable plaques led to the differences in vascular distensibility observed. Recently, de Korte and colleagues studied the mechanical properties of human femoral arteries in vitro using IVUS elastography,37 a technique that determines the relative local displacement between IVUS images acquired at different intravascular pressure levels. The results indicated that vulnerable plaques were more compliant than fibrocalcific plaques. Thus it would be of interest to investigate the extent to which vascular distensibility, as measured by IVUS, is related to vulnerable plaque markers at necropsy examination. Finally, as vascular compliance has been shown to depend on nitric oxide mediated smooth muscle cell relaxation,9 differences in endothelial function between stable and unstable plaques may be reflected in differences in both remodelling and compliance.
LIMITATIONS
First, the patient groups are only of moderate size; however, despite the sample size, significant differences in compensatory vessel enlargement and increased vascular distensibility at the proximal reference site were detected. The lack of a significant difference in distensibility at the lesion site, however, may reflect inadequate numbers of patients in the two groups. Second, elasticity of the arterial wall decreases with age; hence this study involved an age matched control group to minimise the risk of confounding. Third, the potential vasoactive effects of glycoprotein IIb/IIIa inhibitors, circulating catecholamines, or unfractionated heparin on local endothelial function are unknown; therefore interpretation of our results should account for these possible confounders. Additionally, effects of distal disease, run off, collateral flow, and vessel calcification may influence vascular distensibility and potentially confound the results. Fourth, pressure measurements for the calculation of vascular distensibility and stiffness were made at the ostium of the coronary artery by the guiding catheter, which is only a surrogate for the actual pressure at the lesion site. A pressure drop across the lesion site can therefore not be ruled out. Finally, vascular distensibility and β stiffness index showed significant differences between stable and unstable patients at the proximal and distal reference segments only, rather than at the lesion site (although there was a strong tendency towards increased distensibility in the unstable group). At the reference segments, minimal plaque accumulation was present (and plaque area was similar in both groups), allowing a fair comparison of vessel compliance in each individual patient. At the lesion site, vessel mobility is likely to be restricted by a large amount of atheroma.22
CONCLUSIONS
Patients with unstable coronary syndromes show positive remodelling to a significantly greater extent than patients with stable angina, in whom the majority had vessel shrinkage. Vascular distensibility was also found to be increased in the unstable patient group, suggesting a positive relation between compensatory remodelling and vessel compliance. These findings support the concept that, while positive vascular remodelling protects patients from chronic stable angina, this may be at the cost of increased risk of plaque rupture and the associated clinical syndromes of unstable angina, acute myocardial infarction, and sudden death.
Acknowledgments
AJ was supported by a grant from the German Academic Exchange Service (DAAD, Bonn, Germany).