Article Text

Abstract
OBJECTIVE To compare circulating concentrations of N terminal pro-brain natriuretic peptide (N-BNP) and cardiotrophin 1 in stable and unstable angina.
DESIGN AND SETTING Observational study in a teaching hospital.
PATIENTS 15 patients with unstable angina, 10 patients with stable angina, and 15 controls.
MAIN OUTCOME MEASURES Resting plasma N-BNP and cardiotrophin 1 concentrations.
RESULTS N-BNP concentration (median (range)) was 714 fmol/ml (177–3217 fmol/ml) in unstable angina, 169.5 fmol/ml (105.7–399.5 fmol/ml) in stable angina (p = 0.005v unstable angina), and 150.5 fmol/ml (104.7–236.9 fmol/ml) in controls (p < 0.0001v unstable angina; NSv stable angina). Cardiotrophin 1 concentration was 142.5 fmol/ml (42.2–527.4 fmol/ml) in unstable angina, 73.2 fmol/ml (41.5–102.1 fmol/ml) in stable angina (p < 0.05 v unstable angina), and 27 fmol/ml (6.9–54.1 fmol/ml) in controls (p < 0.0005v stable angina; p < 0.0001v unstable angina). Log cardiotrophin 1 correlated with log N-BNP in unstable angina (r = 0.93, p < 0.0001).
CONCLUSIONS Both circulating N-BNP and cardiotrophin 1 are raised in unstable angina, while cardiotrophin 1 alone is raised in stable angina. The role of cardiotrophin 1 and the relation between cardiotrophin 1 and N-BNP in myocardial ischaemia remain to be defined.
- cardiotrophin 1
- brain natriuretic peptide
- angina pectoris
Statistics from Altmetric.com
Cardiotrophin 1, a cytokine of the interleukin 6 (IL-6) family, induces cardiac hypertrophy through the Janus kinase/transcription 3 (JAK/STAT) cascade.1 In addition cardiotrophin 1 has anti-apoptotic effects in myocytes,2 mediated through mitogen activated protein kinase. Cardiotrophin 1 induces heat shock protein accumulation, protecting cultured cardiomyocytes from thermal or ischaemic stress.3
Brain natriuretic peptide (BNP) is synthesised predominantly in the left ventricle as the prohormone prepro-BNP.4 Plasma concentrations of N terminal proBNP (N-BNP or NTproBNP) are likely to reflect de novo synthesis rather than the release of stored BNP, and thus may better reflect natriuretic pathway activation. Raised BNP and N-BNP concentrations occur following myocardial infarction and are inversely related to prognosis.5 Plasma BNP6and IL-67 concentrations are raised in unstable angina. The increased risk of in-hospital coronary events and the worse prognosis associated with raised IL-6 concentrations in unstable angina support a possible role for the IL-6 family in acute coronary syndromes.7
Cardiotrophin 1 stimulates BNP production at a transcriptional level in vitro,8 suggesting that it may be involved in BNP secretion in vivo. N-BNP9 and cardiotrophin 110 are present in human plasma and are raised in heart failure. No data are available on N-BNP or cardiotrophin 1 concentrations in unstable angina. We hypothesised that plasma cardiotrophin 1 and N-BNP may be raised in patients with ischaemic heart disease, particularly in unstable angina.
Methods
SUBJECTS
We compared plasma cardiotrophin 1 and N-BNP concentrations in 15 patients with unstable angina (12 male, three female; median age 71 years, range 45–86 years), 10 patients with stable angina (eight male, two female; median age 70.5 years, range 51–77 years), and 15 normal controls (five male, 10 female; median age 62 years, range 41–79 years). Patients with conditions associated with raised cardiotrophin 1 (history of or current hypertension (systolic blood pressure > 160 mm Hg and/or diastolic blood pressure > 90 mm Hg), clinical or radiological evidence of left ventricular systolic dysfunction, serum creatinine > 140 μmol/l, or valvar heart disease) were excluded.
Unstable angina was defined as class IIIB of Braunwald's classification11 in patients admitted to the coronary care unit of our hospital. All were treated with heparin and oral or intravenous nitrates. Stable angina was defined as a history of cardiac chest pain and positive exercise test. Patients with any increase in frequency or severity of angina in the six weeks preceding the exercise test were excluded. Controls were age matched, on no treatment, and had no evidence of ischaemic heart disease, hypertension, renal failure, or heart failure. The local ethics review committee approved the study.
BLOOD SAMPLING
Following informed consent, 20 ml of venous blood were obtained from each subject after 30–45 minutes of supine rest. In patients with unstable angina blood was drawn within 48 hours of onset of chest pain and in those with stable angina before exercise testing. The blood was transferred into prechilled EDTA tubes containing 500 IU/ml of aprotinin, centrifuged, and plasma separated and stored at −70°C until assay.
IMMUNOLUMINOMETRIC ASSAYS FOR N-BNP AND CARDIOTROPHIN 1
Methods for assay of cardiotrophin 110 and N-BNP12 have been described previously. Within assay and between assay coefficients of variation were 3.0% and 11.2%, respectively, for N-BNP, and 6.2% and 10.3% for cardiotrophin 1. Each peptide value represents the mean of duplicate measurements determined blind to patient details.
STATISTICAL ANALYSIS
Statistical analyses were performed using a Minitab package (Minitab Inc, Pennsylvania, USA). Circulating N-BNP and cardiotrophin 1 concentrations were not normally distributed, and between group comparisons were made using the Mann-Whitney U test. Pearson's correlation coefficients were computed between plasma N-BNP and cardiotrophin 1. Comparisons with p < 0.05 were considered significant.
Results
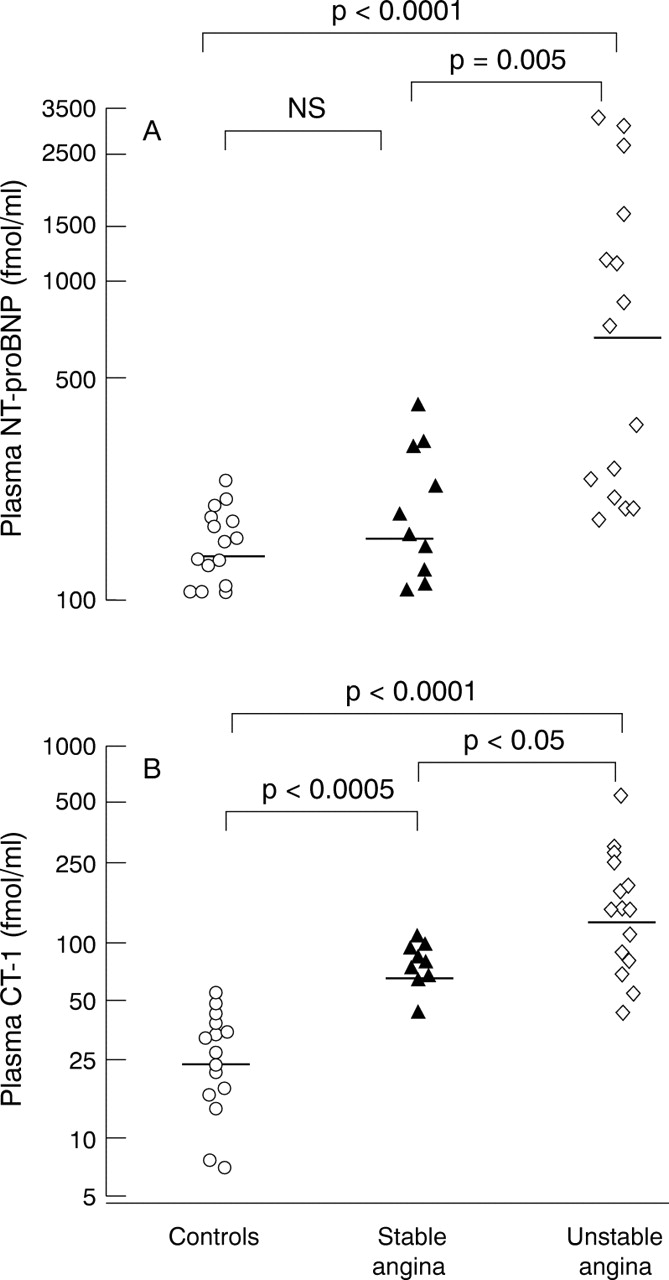
Demographic data for the unstable angina and stable angina subjects are presented in table 1. Mean ages did not differ among the groups (p = 0.26, analysis of variance). N-BNP (median, range) was detected in all normal controls (150.5 fmol/ml, 104.7–236.9 fmol/ml), in patients with stable angina (169.5 fmol/ml, 105.7–399.5 fmol/ml; NS v controls), and in patients with unstable angina (714 fmol/ml, 177–3217 fmol/ml; p < 0.0001 v controls, p = 0.005v stable angina) (fig 1).
Demographic details of patients with unstable and stable angina

Plasma concentrations of N terminal pro-brain natriuretic peptide (N-BNP) (A) and cardiotrophin 1 (CT-1) (B) in control subjects (○), patients with stable angina (▴), and patients with unstable angina (⋄). The uninterrupted line is the median value.
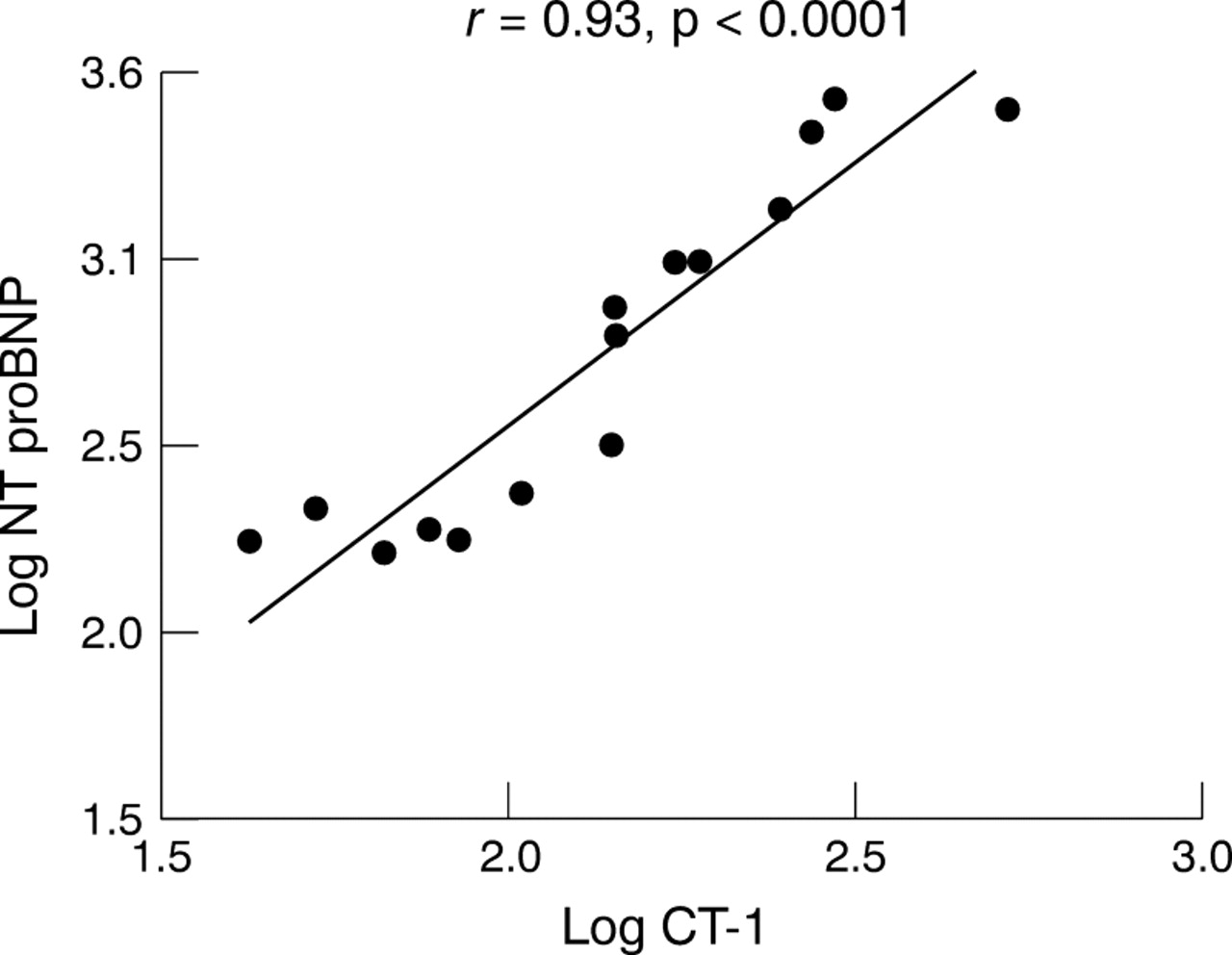
Cardiotrophin 1 (median, range) was detected in all normal controls (27 fmol/ml, 6.9–54.1 fmol/ml), in patients with stable angina (73.2 fmol/ml, 41.5–102.1 fmol/ml; p < 0.0005v controls), and in patients with unstable angina (142.5 fmol/ml, 42.2–527.4 fmol/ml; p < 0.0001v controls; p < 0.05v stable angina) (fig 1). Log cardiotrophin 1 correlated strongly with log N-BNP only in unstable angina (r = 0.93, p < 0.0001) (fig 2). There was no significant correlation between log cardiotrophin 1 and log N-BNP in patients with stable angina or in controls.
{kind=link}
{kind=link}
Correlation between log N terminal pro-brain natriuretic peptide (N-BNP) and log cardiotrophin 1 (CT-1) in subjects with unstable angina.
There were no inpatient deaths among the patients with unstable angina, six of whom underwent early coronary angiography. One of these had an angioplasty and one was referred for coronary artery surgery. In this small study we could not find any association between peptide concentrations and any of these outcomes.
Discussion
We found raised plasma concentrations of N-BNP and cardiotrophin 1 in patients with unstable angina in comparison with both control subjects and patients with stable angina, and a strong correlation between plasma N-BNP and cardiotrophin 1 in unstable angina. Our data are in keeping with previous studies indicating raised concentrations of cytokines such as IL-6 in unstable angina.7
The mechanism of production of these peptides in myocardial ischaemia is unclear. Myocardial ischaemia in unstable angina may increase regional ventricular wall stretch owing to local depression of myocardial contraction. Mechanical stretch can activate the JAK/STAT pathway and may stimulate N-BNP secretion13 and augment the messenger RNA expression of IL-6 and cardiotrophin 1.14 This common mechanism of stimulation may explain the correlation between N-BNP and cardiotrophin 1 in unstable angina. Alternatively, cardiotrophin 1 may directly promote myocardial transcription of BNP.8 This cascade of events is also compatible with the small elevation of cardiotrophin 1 in stable angina. Another explanation could be different release processes in stable and unstable angina.
In man, BNP antagonises the renin–angiotensin system, causing natriuresis and contraction of plasma volume.15 In animals, cardiotrophin 1 elicits dose dependent vasodilatation that may be mediated through nitric oxide.16 Our findings with regard to N-BNP concentrations in unstable angina are analogous to those previously reported for BNP.6 We have observed a pronounced rise in N-BNP following acute myocardial infarction.17 Our findings with regard to cardiotrophin 1 are consistent with those in myocardial infarction18 and chronic heart failure.10 While the significance of these findings is unclear, the cytoprotective effects of cardiotrophin 1 during myocardial ischaemia may be relevant.3
LIMITATIONS
Although we studied small numbers of patients, groups were carefully defined and there was a clear separation in the concentrations of cardiotrophin 1 among the groups and in N-BNP for unstable angina. We set out to compare N-BNP and cardiotrophin 1 for the reasons discussed above. However, we have not compared cardiotrophin 1 concentrations to IL-6 or related cytokines, or N-BNP to BNP. Analysis of the relation of cardiotrophin 1 and N-BNP to markers of microinfarction such as troponin T would be of interest. Similarly the relation of peptide concentrations to echocardiographic indices of left ventricular function and to the angiographic extent of coronary artery disease remains to be established.
The influence of pharmacological treatment on concentrations of each peptide has not been addressed. We found no relation between the number of antianginal drugs and either peptide concentration. Most of the patients with unstable angina were receiving calcium antagonists but we have no direct evidence that this influenced our findings. Importantly, while cardiotrophin 1 stimulates synthesis of BNP, and while we have demonstrated correlation of circulating concentrations of the two peptides, our study does not provide direct evidence for a causal relation between cardiotrophin 1 and N-BNP concentrations. Finally, myocardial ischaemia is a dynamic process and further studies are required to examine the profile of cardiotrophin 1 and N-BNP in both unstable and stable angina.
CONCLUSIONS
This study suggests there is elevation of a cytokine with cytoprotective properties in unstable angina. Cardiotrophin 1 or its analogues may have therapeutic potential in the protection of cardiac cells from ischaemic injury. In the absence of known inhibitors of cardiotrophin 1, it is not currently possible to investigate the consequences of inhibiting the actions of this agent in man. Further studies are now required to elucidate the pathophysiological role of the relation between cardiotrophin 1 and N-BNP in unstable angina, and its prognostic significance.
Acknowledgments
ST was supported by a Leicester Royal Infirmary Research Fellowship. Methyl acridinium esters were a gift from Drs S Woodhead and I Weeks, Molecular Light Technology Ltd, Cardiff, UK.
References
Commentary
Cardiotrophin 1 is a cytokine discovered 5 years ago belonging to the interleukin-6 family. Like so many cytokines, it regulates more than one cellular action. As the name suggests, cardiotrophin 1 primarily exerts growth promoting properties on cardiac myocytes and may play an especially important role in cardiac development. Both the peptide and its receptor proteins are present in normal cardiac myocytes, but it is also found in a number of other cell types. Experimental studies suggest that it is also cardioprotective, reducing the extent of ischaemia–reperfusion injury in cardiac tissue. The report by Talwar and colleagues is of interest in demonstrating that plasma concentrations of cardiotrophin 1 are raised above control levels in patients with ischaemic heart disease and especially in patients with an acute coronary syndrome (unstable angina). The significance of this observation must remain speculative at present. It is presumed that the source of the plasma cardiotrophin 1 is the heart itself and it may be the case that cardiotrophin 1 is elaborated during episodes of myocardial ischaemia as a cardioprotective response in anticipation of further episodes of ischaemia.